Acute pancreatitis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Searching PubMed
"acute pancreatitis"[MeSH Terms] AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Acute Pancreatitis
Definition and Epidemiology
Acute pancreatitis (AP) is a sudden inflammatory disease of the pancreas triggered by inappropriate intracellular activation of digestive enzymes. It is one of the most common indications for inpatient hospitalization. Incidence in the US is approximately 111 cases per 100,000 persons per year. The disease is self-limited in 85-90% of cases, resolving within 3-7 days, but 5-10% develop necrotizing disease with significant mortality risk.
- Current Surgical Therapy 14e, p. 604
- Harrison's Principles of Internal Medicine 22E, p. 2790
Etiology ("I GET SMASHED" mnemonic)
| Cause | Notes |
|---|---|
| Gallstones | Most common overall cause |
| Alcohol | Second most common; direct acinar cell toxicity |
| Hypertriglyceridemia | Triglycerides >1000 mg/dL precipitates AP |
| Hypercalcemia | Activates trypsinogen |
| Post-ERCP | Iatrogenic; significant risk |
| Medications | Valproate, L-asparaginase, azathioprine, thiazides, steroids |
| Trauma | Usually blunt abdominal trauma |
| Tumor / Structural | Pancreas divisum, ampullary tumors |
| Infections | Mumps, CMV, coxsackievirus, Mycoplasma, HIV |
| Autoimmune | IgG4-related disease |
| Hereditary / Genetic | PRSS1, SPINK1, CFTR mutations |
| Idiopathic | 5% of cases; micro-lithiasis often occult cause |
- Grainger & Allison's Diagnostic Radiology, p. 677
- Current Surgical Therapy 14e, p. 604
Pathophysiology
The central mechanism is premature, intrapancreatic activation of trypsinogen to trypsin, which then activates other proteolytic enzymes (chymotrypsin, elastase, phospholipase A2, kallikrein). This triggers:
- Autodigestion of pancreatic parenchyma and peripancreatic fat
- Local inflammatory cascade - cytokine release (IL-1, IL-6, TNF-α) causes acinar cell necrosis
- Systemic inflammatory response syndrome (SIRS) - in severe cases, systemic spillover of activated enzymes and cytokines causes distant organ injury (ARDS, AKI, cardiovascular collapse)
The degree of acinar cell death and vascular injury determines whether the disease is interstitial edematous (mild, most common) or necrotizing (5-10%, high mortality).
Diagnosis
Diagnosis requires 2 of 3 criteria (Revised Atlanta Classification, 2012):
- Abdominal pain characteristic of AP (epigastric, radiating to the back, onset over hours, aggravated by eating)
- Serum lipase or amylase ≥3× upper limit of normal
- Characteristic imaging findings on CT, MRI, or ultrasound
Note: Lipase is preferred over amylase - it is more sensitive and specific, and remains elevated longer. Amylase can be normal in hypertriglyceridemia-induced AP.
Abdominal ultrasound is the initial imaging of choice to evaluate for biliary etiology (gallstones, common bile duct dilation). CT with contrast is reserved for: (a) diagnostic uncertainty, (b) failure to improve after 72 hours, or (c) assessment for necrosis.
- Grainger & Allison's Diagnostic Radiology, p. 677
- Harrison's 22E, p. 2789
CT Evolution of Necrotizing Pancreatitis
Harrison's Principles of Internal Medicine 22E, Fig. 359-1 - Evolution of changes of acute necrotizing pancreatitis:
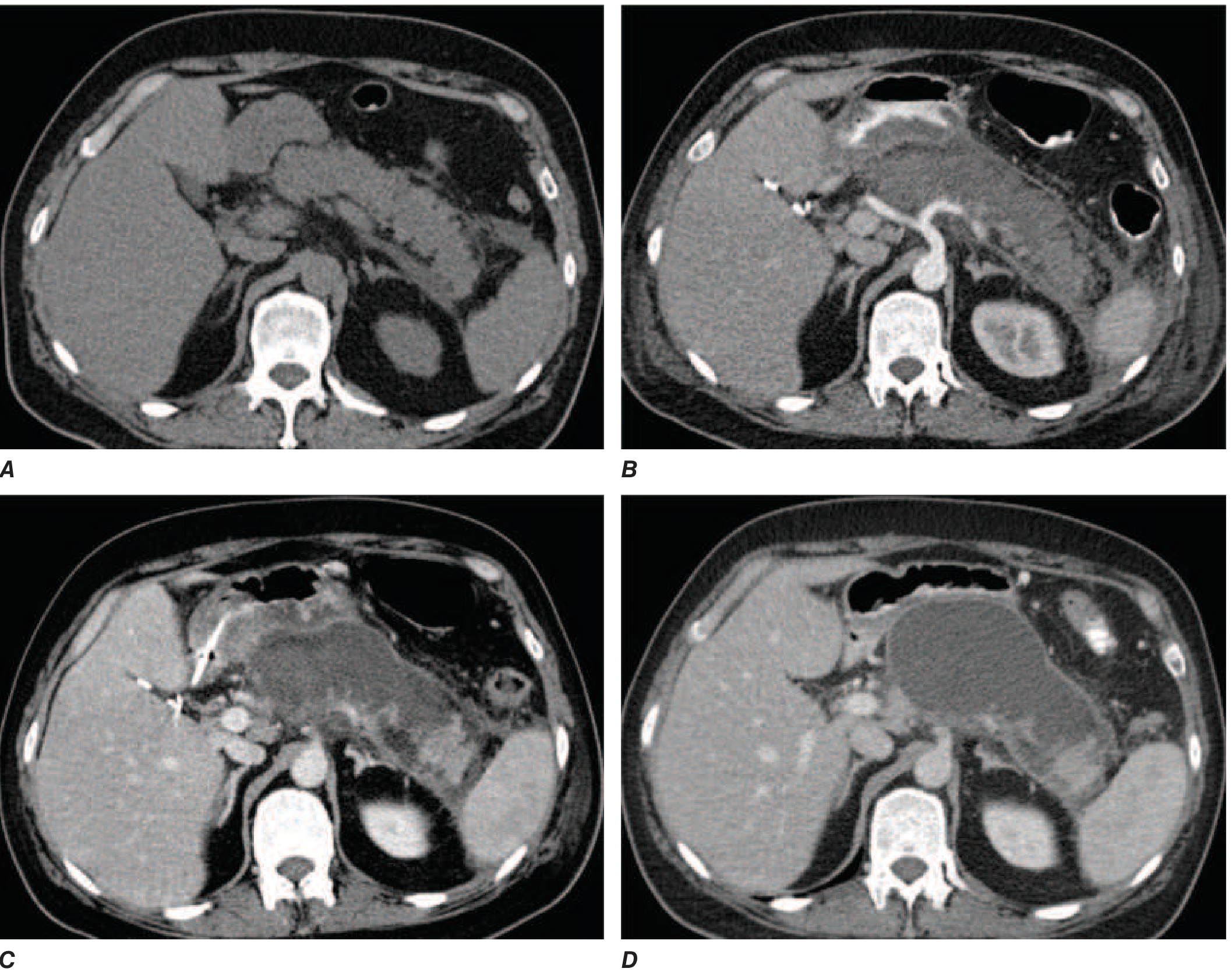
A - Admission: mild peripancreatic fat stranding | B - 1 week: extensive pancreatic body necrosis (absent contrast enhancement) | C - 2 weeks: acute necrotic collection (heterogeneous, semi-organized) | D - Several weeks: walled-off necrosis (well-encapsulated, essentially replacing the pancreas)
Severity Classification (2012 Revised Atlanta)
| Grade | Organ Failure | Local/Systemic Complications | Mortality |
|---|---|---|---|
| Mild | Absent | Absent | Very rare (<5%) |
| Moderately Severe | Transient (<48 h) | Present, without persistent organ failure | Low |
| Severe | Persistent (>48 h) | Present | 36-50%; extremely high with infected necrosis |
- Current Surgical Therapy 14e, Table 1
Severity Scoring Systems
Ranson's Criteria
(Schwartz's Principles of Surgery 11th Ed, Table 33-7)
Non-gallstone AP:
| At Admission | During Initial 48 h |
|---|---|
| Age >55 y | Hematocrit fall >10 points |
| WBC >16,000/mm³ | BUN elevation >5 mg/dL |
| Blood glucose >200 mg/dL | Serum Ca²⁺ <8 mg/dL |
| LDH >350 IU/L | PaO₂ <60 mmHg |
| AST >250 U/dL | Base deficit >4 mEq/L |
| Fluid sequestration >6 L |
Gallstone AP uses slightly different thresholds (age >70, WBC >18,000, glucose >220, LDH >400, fluid sequestration >4 L).
Interpretation: <3 criteria = mild disease; ≥6 criteria = severe disease, 50% mortality risk.
BISAP Score (≥3 = high risk)
- (B) BUN >25 mg/dL
- (I) Impaired mental status (GCS <15)
- (S) SIRS (≥2 of 4 criteria present)
- (A) Age >60 years
- (P) Pleural effusion on imaging
APACHE II Score
- ≥8 at 24 h predicts severe disease; performs similarly to Ranson's criteria
CT Severity Index (CTSI / Balthazar Score)
- Combines degree of pancreatic inflammation (grades A-E) with extent of necrosis (0%, <33%, 33-50%, >50%)
- CTSI ≥7 associated with high morbidity and mortality
Additional Severity Markers
| Parameter | High-Risk Threshold |
|---|---|
| CRP | >150 mg/L at 48 h |
| Hematocrit (admission) | >44% (hemoconcentration) |
| BUN (admission) | >20 mg/dL |
| BMI | >30 kg/m² |
| Age | >60 years |
- Harrison's 22E, Table 359-2
Local Complications (2012 Revised Atlanta Definitions)
| Term | Definition | Timing |
|---|---|---|
| Interstitial edematous pancreatitis | Diffuse gland enlargement, edema, no necrosis; homogeneous contrast enhancement | - |
| Acute Peripancreatic Fluid Collection (APFC) | Homogeneous, non-encapsulated fluid collection, no necrosis | <4 weeks |
| Pancreatic Pseudocyst | Well-defined encapsulated fluid, no solid component | >4 weeks |
| Acute Necrotic Collection (ANC) | Heterogeneous collection with non-liquid components; pancreatic +/- peripancreatic necrosis | <4 weeks |
| Walled-Off Necrosis (WON) | Mature encapsulated collection of necrotic debris | >4 weeks |
Most APFCs and pseudocysts resolve spontaneously. Necrotizing pancreatitis carries organ failure prevalence >50% and carries mortality risk of up to 50% with multiorgan failure.
- Current Surgical Therapy 14e, Tables 1-2
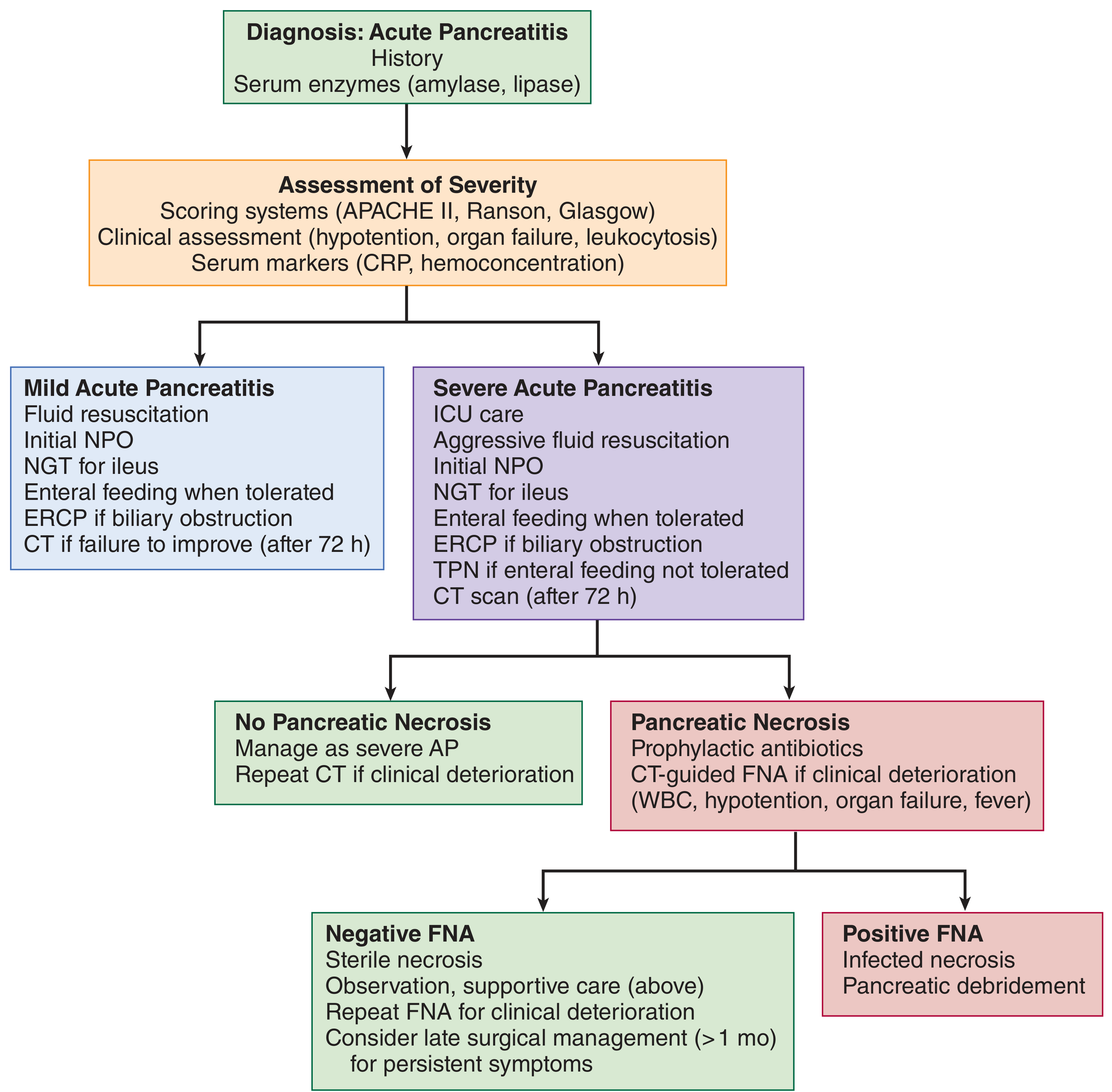
Management
Management Algorithm (Maingot's Abdominal Operations)
1. Fluid Resuscitation
The single most important early intervention.
- Preferred fluid: Lactated Ringer's (LR) - shown to decrease systemic inflammation (lower CRP) vs. normal saline; avoids hyperchloremic acidosis
- Traditionally: bolus 15-20 mL/kg, then 2-3 mL/kg/h
- A 2022 RCT (WATERFALL trial) demonstrated that moderate resuscitation (10 mL/kg bolus, then 1.5 mL/kg/h) is preferred over aggressive, as aggressive hydration increases fluid overload risk without improving outcomes
- Monitor: urine output >0.5 mL/kg/h, hematocrit, BUN every 8-12 h; falling Hct and BUN at 12-24 h confirms adequate resuscitation
- Avoid overresuscitation - abdominal compartment syndrome is a recognized complication
2. Analgesia
- IV opioids are standard; no evidence favors one agent over another
- Earlier concerns about morphine causing sphincter of Oddi spasm are not clinically significant
3. Nutrition
- Mild AP: resume oral diet as soon as tolerated (often within 24-48 h), typically starting with low-fat soft diet
- Moderate-severe AP: early enteral nutrition (EN) is preferred over TPN - maintains gut mucosal integrity, reduces bacterial translocation, reduces infectious complications
- Route: nasojejunal (NJ) or nasogastric (NG) tube feeding is equally effective; NJ is traditional but NG is simpler
- TPN only if EN is not tolerated or contraindicated
4. Antibiotics
- Not routinely indicated in AP, even with necrosis
- Indications: confirmed infected necrosis (positive FNA cultures, gas in necrosis on CT), or concurrent cholangitis
- Prophylactic antibiotics in sterile necrotizing pancreatitis: NOT recommended (multiple RCTs show no benefit and risk of fungal superinfection)
- If infected necrosis: broad-spectrum agents penetrating pancreatic tissue (carbapenems, fluoroquinolones + metronidazole)
5. Etiology-Specific Management
- Gallstone pancreatitis with cholangitis - urgent ERCP within 24-48 h
- Gallstone pancreatitis without cholangitis - cholecystectomy during same admission (mild AP) or after recovery (severe AP) to prevent recurrence; biliary sphincterotomy for non-surgical candidates
- Hypertriglyceridemia-induced AP - IV insulin to lower triglycerides; NPO for 24-36 h; long-term fibrates/omega-3s
- Drug-induced AP - withdraw offending agent immediately
6. Management of Necrosis
-
Sterile necrosis - conservative management; surgical debridement only for persistent symptoms after ≥4 weeks
-
Infected necrosis (fever, leukocytosis, gas on CT, positive FNA):
- Step-up approach is standard: percutaneous or endoscopic drainage first, escalating to minimally invasive or open necrosectomy only if needed
- Timing: delay intervention until necrosis is "walled-off" (>3-4 weeks) to reduce morbidity
- Endoscopic ultrasound-guided transmural drainage increasingly preferred for WON adjacent to the stomach/duodenum
-
Harrison's 22E, pp. 2790-2792
-
Current Surgical Therapy 14e, pp. 604-608
Systemic Complications
| System | Complication |
|---|---|
| Pulmonary | ARDS, pleural effusion (left > right), atelectasis |
| Renal | Acute kidney injury |
| Cardiovascular | Hypotension, shock |
| Hematologic | DIC |
| Metabolic | Hypocalcemia, hyperglycemia |
| GI/Vascular | Splenic/portal vein thrombosis, mesenteric ischemia |
| Hemorrhagic | Erosion into peripancreatic vessels (splenic artery pseudoaneurysm) |
Notable cutaneous signs:
- Grey Turner's sign - flank ecchymosis (retroperitoneal hemorrhage)
- Cullen's sign - periumbilical ecchymosis Both indicate hemorrhagic pancreatitis and poor prognosis.
Summary: Key Clinical Points
| Feature | Key Fact |
|---|---|
| Diagnosis | 2 of 3: pain + lipase/amylase ≥3× ULN + imaging |
| First-line imaging | Abdominal ultrasound (biliary workup) |
| Best fluid | Lactated Ringer's (moderate resuscitation preferred) |
| Antibiotics | Only for confirmed infected necrosis |
| Nutrition | Early enteral feeding preferred; resume oral diet ASAP in mild AP |
| Necrosectomy timing | Delay ≥4 weeks; use step-up approach |
| Gallstone AP | Cholecystectomy same admission (mild); ERCP if cholangitis |
| Severity marker | Persistent SIRS at 24 h predicts organ failure and necrosis |
Sources: Harrison's Principles of Internal Medicine 22E; Current Surgical Therapy 14e (Ye & Hines); Schwartz's Principles of Surgery 11th Ed; Grainger & Allison's Diagnostic Radiology; Maingot's Abdominal Operations; Sleisenger and Fordtran's Gastrointestinal and Liver Disease; ROSEN's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.