Anatomy and blood supply of heart
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Excellent - I have rich textbook content and high-quality diagrams. Now I'll compile the comprehensive answer.
Anatomy and Blood Supply of the Heart
Sources: Gray's Anatomy for Students; Goldman-Cecil Medicine; Fuster and Hurst's The Heart, 15th ed.
1. Position and External Features
The heart is a hollow, conical muscular organ located in the middle mediastinum, enclosed within the pericardial sac. It sits obliquely - roughly two-thirds of its mass lies to the left of the midline. It has:
- Base - the posterior flat surface formed mainly by the left atrium, facing posteriorly and slightly superiorly
- Apex - points inferiorly, anteriorly, and to the left; formed by the left ventricle (felt as apex beat in the 5th intercostal space, midclavicular line)
- Sternocostal (anterior) surface - mainly right ventricle
- Diaphragmatic (inferior) surface - mainly left ventricle
- Right pulmonary surface - mainly right atrium
- Left pulmonary surface - mainly left ventricle (forms the cardiac notch of the lung)
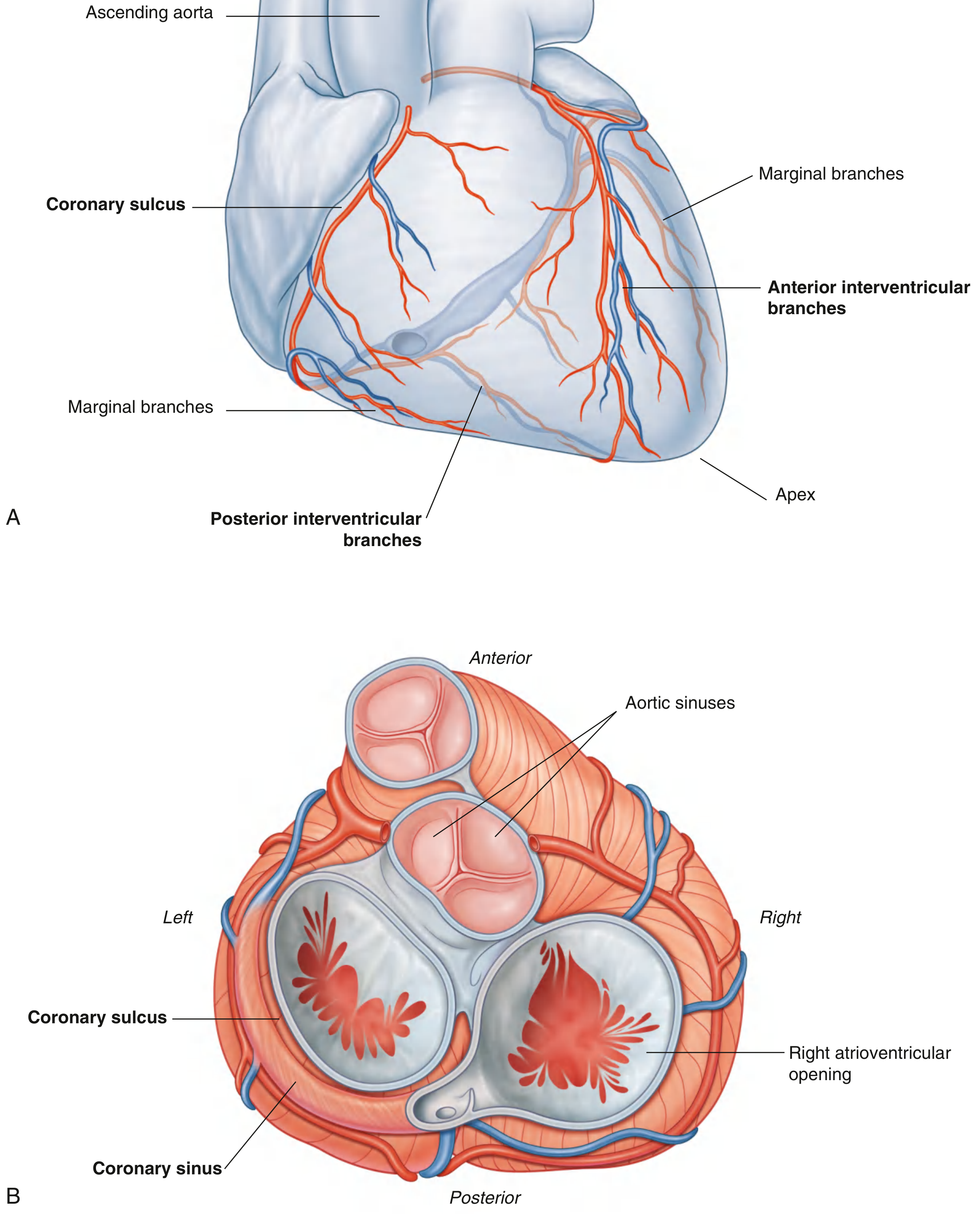
External Grooves (Sulci)
| Sulcus | Contents | Significance |
|---|---|---|
| Coronary (atrioventricular) sulcus | Coronary arteries, coronary sinus, fat | Separates atria from ventricles; runs around the heart in a near-horizontal plane |
| Anterior interventricular sulcus | Left anterior descending (LAD) artery + great cardiac vein | Marks IV septum on anterior surface |
| Posterior interventricular sulcus | Posterior descending artery (PDA) + middle cardiac vein | Marks IV septum on posterior surface |
2. Chambers of the Heart
Right Atrium
- Receives deoxygenated blood from the superior vena cava (SVC), inferior vena cava (IVC), and coronary sinus
- Internal features: crista terminalis (smooth-rough divide), pectinate muscles (rough anterior part), fossa ovalis (remnant of foramen ovale), sinus venarum (smooth posterior part)
- Opens into right ventricle via the tricuspid (right AV) valve
Right Ventricle
- Crescent-shaped in cross-section (wraps around the left ventricle)
- Internal: trabeculae carneae, papillary muscles (anterior, posterior, septal), moderator band (carries right bundle branch)
- Blood exits through the pulmonary valve into the pulmonary trunk
- Wall thickness: ~3-5 mm (low pressure circuit)
Left Atrium
- Forms most of the base of the heart
- Receives four pulmonary veins (two from each lung)
- Opens into left ventricle via the mitral (bicuspid/left AV) valve
- Smooth-walled with a small left auricle anteriorly
Left Ventricle
- Ellipsoid chamber; wall thickness ~8-12 mm (3x the right ventricle)
- Primary pumping chamber; generates ~120 mmHg systolic pressure
- Internal: papillary muscles (anterolateral and posteromedial), trabeculae carneae, chordae tendineae
- Blood exits through the aortic valve into the ascending aorta
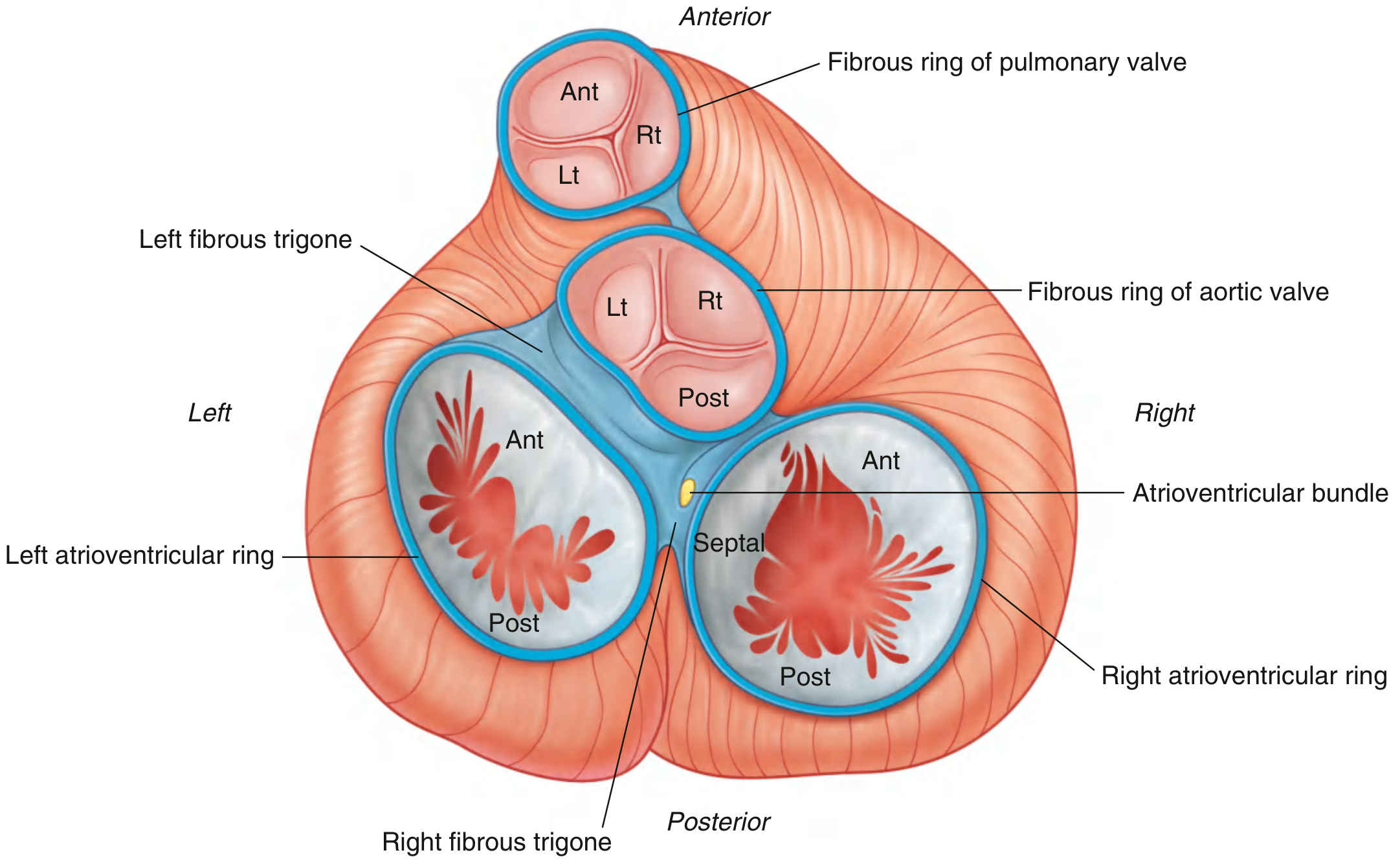
3. Cardiac Valves and Skeleton
The Four Valves
| Valve | Type | Leaflets | Location |
|---|---|---|---|
| Tricuspid | AV (right) | 3 - anterior, posterior, septal | Right AV orifice |
| Mitral (bicuspid) | AV (left) | 2 - anterior, posterior | Left AV orifice |
| Pulmonary | Semilunar | 3 cusps | Base of pulmonary trunk |
| Aortic | Semilunar | 3 cusps (L, R, posterior/non-coronary) | Base of ascending aorta |
All four valves open and close passively in response to pressure gradients.
Cardiac Skeleton
The fibrous skeleton anchors the valves, provides electrical insulation between atria and ventricles, and serves as attachment for myocardium. It consists of:
- Fibrous rings (annuli fibrosi) around all four valves
- Right and left fibrous trigones - dense collagenous masses between the aortic, mitral, and tricuspid valve rings
- The atrioventricular bundle (Bundle of His) passes through the right fibrous trigone
4. Layers of the Heart Wall
| Layer | Description |
|---|---|
| Epicardium | Visceral pericardium; serous layer of mesothelium + fat; coronary vessels run here |
| Myocardium | Cardiac muscle; thickest in left ventricle |
| Endocardium | Inner endothelial lining of chambers and valves |
The pericardium is a fibroserous sac with:
- Fibrous pericardium - tough outer layer
- Serous pericardium - parietal (lines fibrous) and visceral (= epicardium) layers with ~15-50 mL of pericardial fluid between them
5. Blood Supply - Coronary Arteries
Both coronary arteries arise from the aortic sinuses (sinuses of Valsalva) in the initial portion of the ascending aorta, just above the aortic valve. They travel in the epicardium.
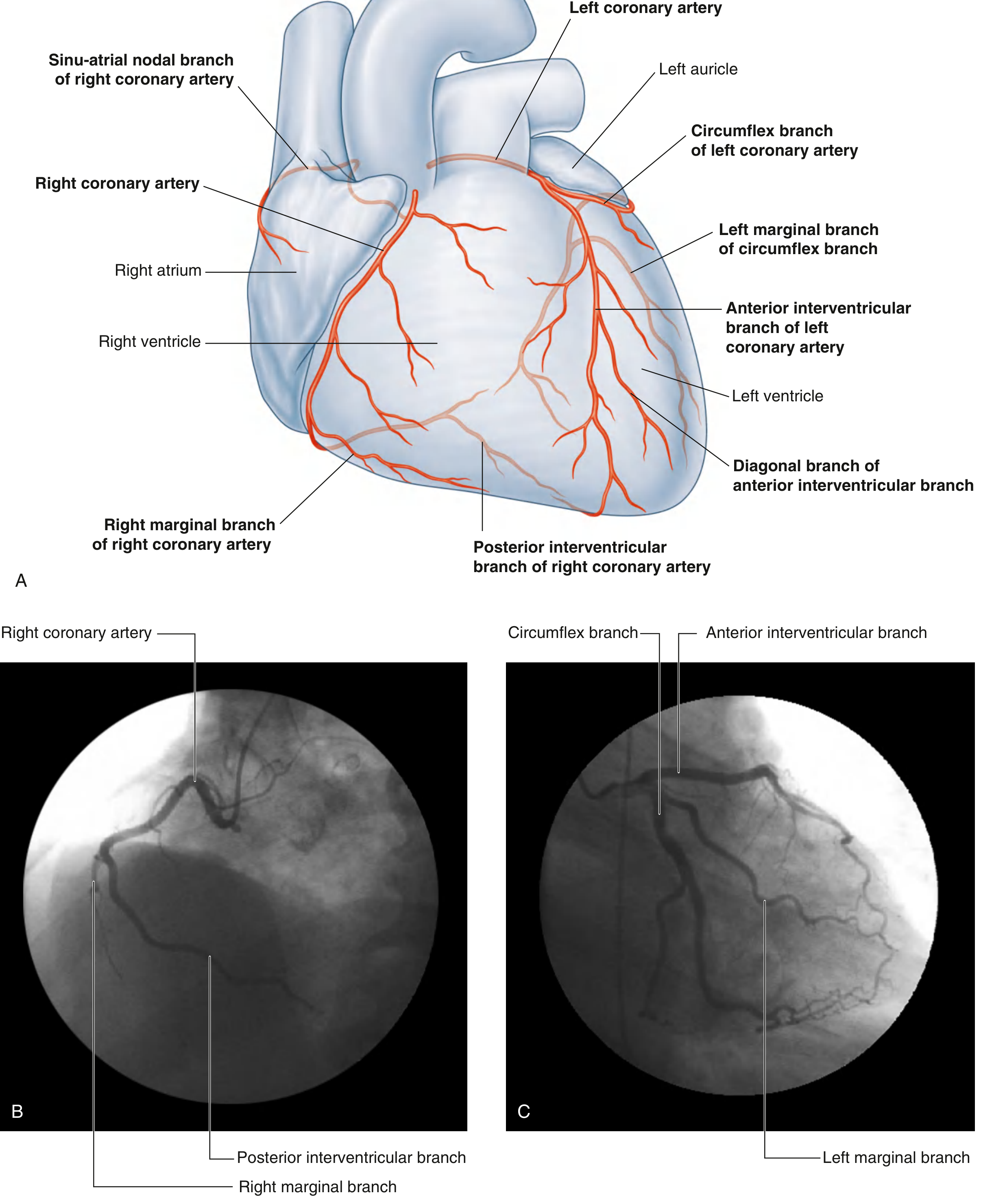
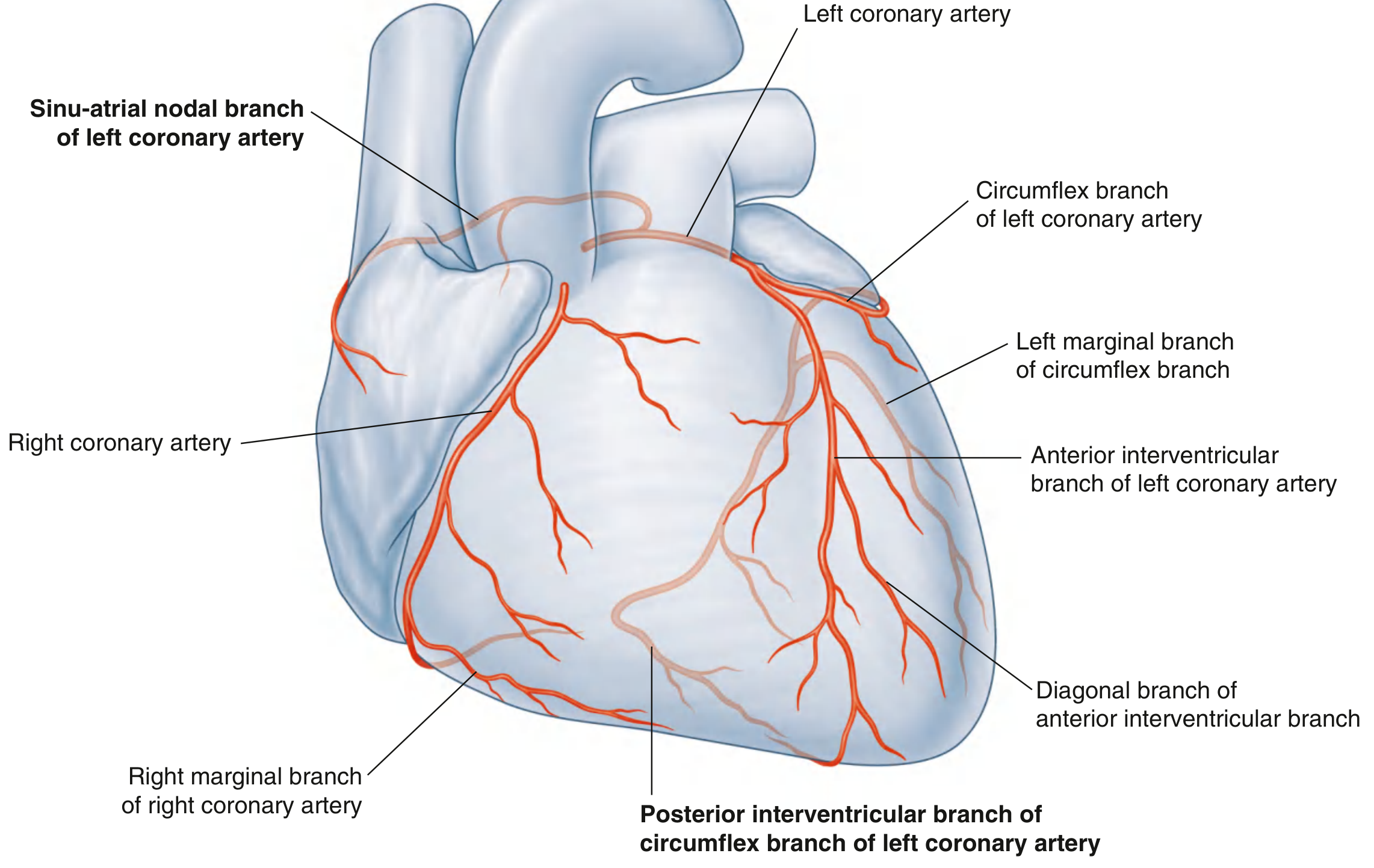
Right Coronary Artery (RCA)
- Origin: Right aortic sinus
- Course: Descends in the coronary sulcus between the right atrium and right ventricle; turns posteriorly at the inferior margin; continues along the base/diaphragmatic surface
Key branches:
| Branch | Territory |
|---|---|
| SA nodal branch (from early atrial branch) | Sinoatrial node (in ~60% from RCA) |
| Right marginal branch | Acute margin of right ventricle toward the apex |
| AV nodal branch | Atrioventricular node (in most cases) |
| Posterior interventricular branch (PDA) | Posterior 1/3 of interventricular septum, posterior left ventricle |
Supply territory of RCA:
- Right atrium and right ventricle
- SA and AV nodes (in right-dominant hearts)
- Interatrial septum and a portion of left atrium
- Posteroinferior 1/3 of the interventricular septum
- Posterior part of the left ventricle
Left Coronary Artery (LCA)
- Origin: Left aortic sinus
- Course: Passes between the pulmonary trunk and left auricle, then divides into its two terminal branches
LCA divides into:
1. Left Anterior Descending (LAD) / Anterior Interventricular Artery
- Descends in the anterior interventricular sulcus toward the apex
- Wraps around the apex to supply a small portion of the posterior surface
| Branch | Territory |
|---|---|
| Diagonal branches (1-2 large) | Anterolateral left ventricle |
| Septal perforating branches | Anterior 2/3 of interventricular septum including Bundle of His |
2. Circumflex Branch (LCx)
- Courses in the coronary sulcus toward the left and onto the base/diaphragmatic surface
- Usually ends before reaching the posterior interventricular sulcus (in right-dominant hearts)
| Branch | Territory |
|---|---|
| Left marginal (obtuse marginal) artery | Obtuse (left) margin of heart |
| Posterior interventricular branch | Only in left-dominant pattern |
Supply territory of LCA:
- Most of left atrium and left ventricle
- Most of the interventricular septum (anterior 2/3)
- AV bundle and its branches
- Anterolateral papillary muscle
Coronary Dominance
Dominance is determined by which artery gives rise to the posterior descending artery (PDA):
| Pattern | Frequency | PDA from |
|---|---|---|
| Right dominant | ~70% | RCA |
| Left dominant | ~10% | LCx branch of LCA |
| Codominant | ~20% | Both RCA and LCx |
In left dominant hearts, the circumflex is enlarged and supplies most of the posterior left ventricle, while the RCA is relatively small.
Clinical Correlations of Coronary Occlusion
| Artery Occluded | Area of Infarction | ECG Changes |
|---|---|---|
| LAD (most common) | Anterior wall + anterior septum of LV | ST elevation V1-V4 |
| RCA | Inferior wall LV; RV; SA/AV nodes | ST elevation II, III, aVF; bradycardia/blocks |
| LCx | Lateral/posterior LV wall | ST elevation I, aVL, V5-V6 |
6. Coronary Blood Flow Physiology
From Goldman-Cecil Medicine:
- Diastolic aortic pressure drives most coronary flow (especially to the subendocardium)
- During systole, intramyocardial pressure compresses the inner (endocardial) coronary vessels - so subendocardial flow is almost exclusively diastolic
- Epicardial vessels receive flow in both systole and diastole
- Flow can increase up to 6-fold during exercise via vasodilators: nitric oxide, adenosine, bradykinin, prostaglandins, CO2
This explains why the subendocardium is most vulnerable to ischemia (first zone to become ischemic in hypotension or tachycardia).
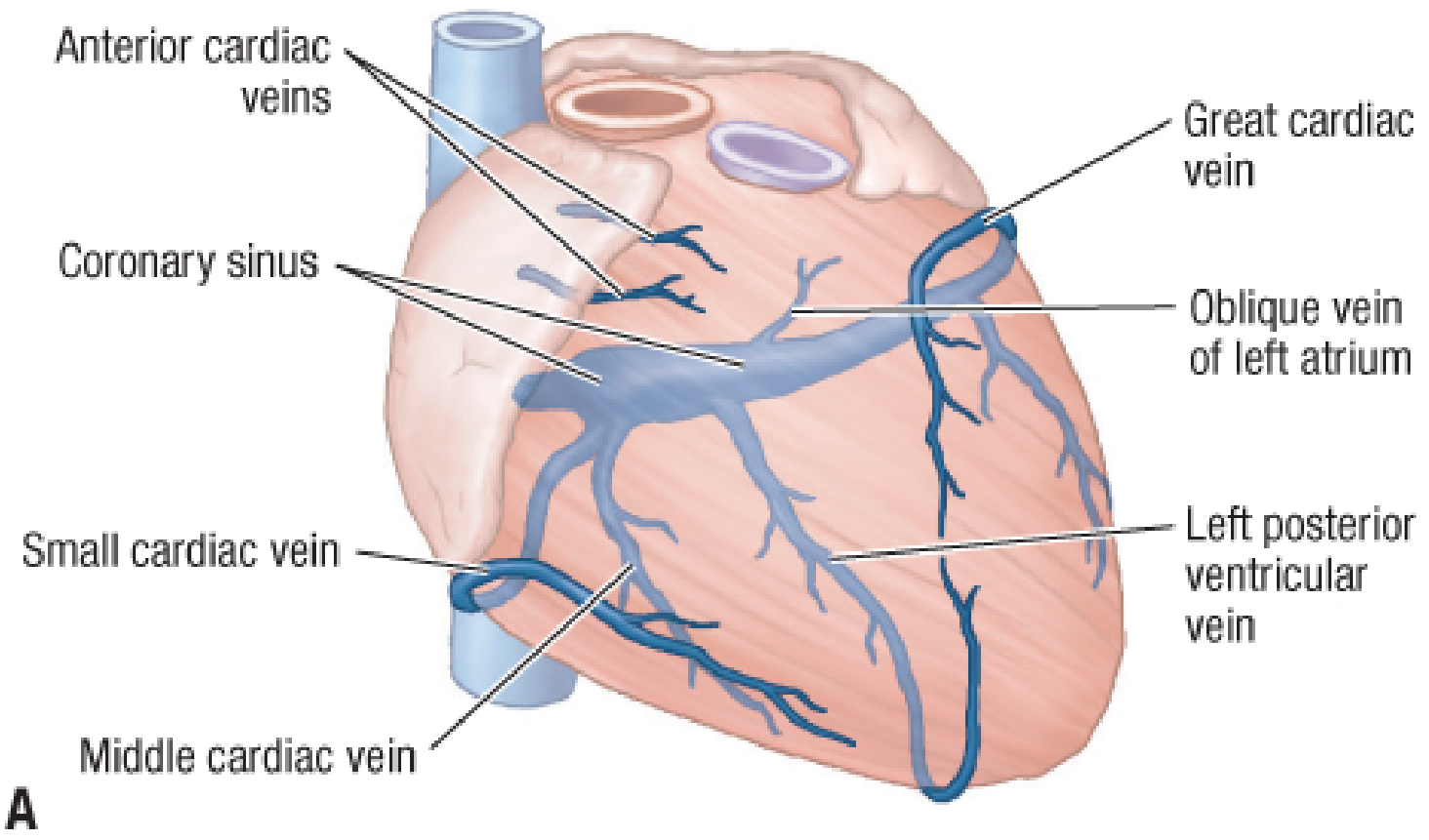
7. Venous Drainage
Most venous blood returns via cardiac veins draining into the coronary sinus:
| Vein | Runs with | Drains |
|---|---|---|
| Great cardiac vein | LAD (anterior IV sulcus) | Anterior heart; joins coronary sinus at left end |
| Middle cardiac vein | PDA (posterior IV sulcus) | Posterior heart |
| Small cardiac vein | Right marginal artery | Right margin |
| Oblique vein of left atrium (Marshall) | - | Left atrium |
| Coronary sinus | Posterior coronary sulcus | Receives great, middle, small veins → right atrium |
Smaller vessels that bypass the coronary sinus:
- Anterior cardiac veins - drain directly into the right atrium
- Venae cordis minimae (Thebesian veins) - tiny veins opening directly into cardiac chambers (a cause of physiologic right-to-left shunting)
The coronary sinus (the largest cardiac vein) lies in the coronary sulcus on the posterior surface between the left atrium and left ventricle, and empties into the right atrium between the IVC opening and the right AV orifice.
8. Nerve Supply
| Type | Source | Function |
|---|---|---|
| Sympathetic | T1-T4 via cardiac plexus | Increases rate (chronotropy) and force (inotropy); vasodilation of coronaries |
| Parasympathetic | Vagus (CN X) via cardiac plexus | Decreases rate; minimal effect on ventricles |
| Visceral afferents (pain) | Follow sympathetic fibers → T1-T4 | Referred cardiac pain to left arm, jaw, chest |
Cardiac referred pain enters the spinal cord at T1-T4, which explains pain in the left arm, jaw, and chest during myocardial ischemia.
Sources: Gray's Anatomy for Students (9780323934237); Goldman-Cecil Medicine (9780323930345); Fuster and Hurst's The Heart, 15th Edition (9781264257560)
Anatomy and blood supply of heart
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
All diagrams retrieved. Now I have comprehensive content from four textbooks plus six high-quality images. Composing the full answer:
Anatomy and Blood Supply of the Heart
Sources: Gray's Anatomy for Students | Goldman-Cecil Medicine | Color Atlas of Human Anatomy Vol. 2 | Fischer's Mastery of Surgery 8e
1. Position, Orientation and External Surfaces
The heart is a hollow, conical muscular organ in the middle mediastinum, enclosed within the pericardial sac. About two-thirds of its mass lies to the left of the midline. Its size approximates a closed fist (~12 cm long, 9 cm wide).
Surfaces
| Surface | Formed by | Faces |
|---|---|---|
| Sternocostal (anterior) | Mostly right ventricle | Anteriorly |
| Diaphragmatic (inferior) | Mostly left ventricle | Inferiorly onto central tendon |
| Base (posterior) | Mostly left atrium, some right atrium | Posteriorly/superiorly |
| Right pulmonary | Right atrium | Right lung |
| Left pulmonary | Left ventricle | Left lung (forms cardiac notch) |
- Apex - formed by the left ventricle, points inferiorly, anteriorly, and to the left; felt as the apex beat at the 5th intercostal space in the midclavicular line
- Base - the posterior flat surface, receives the great veins
External Sulci (Grooves)
| Sulcus | Contents | Significance |
|---|---|---|
| Coronary (atrioventricular) sulcus | Coronary arteries, coronary sinus, fat | Separates atria from ventricles; runs horizontally around the heart |
| Anterior interventricular sulcus | LAD artery + great cardiac vein | Marks IV septum anteriorly |
| Posterior interventricular sulcus | PDA + middle cardiac vein | Marks IV septum posteriorly |
2. Layers of the Heart Wall
| Layer | Detail |
|---|---|
| Pericardium | Fibroserous sac: outer fibrous pericardium + serous (parietal + visceral layers); 15-50 mL pericardial fluid |
| Epicardium | Visceral pericardium; mesothelium + subepicardial fat; coronary vessels run here |
| Myocardium | Cardiac muscle; thickest in LV (~12 mm); thinnest in atria |
| Endocardium | Inner endothelial lining of all chambers and valve surfaces |
3. The Four Chambers
Right Atrium
- Receives deoxygenated blood via SVC, IVC, and coronary sinus
- Internal landmarks: crista terminalis (smooth/rough divide), pectinate muscles (rough anterior wall), fossa ovalis (remnant of foramen ovale), sinus venarum (smooth posterior inflow region)
- Opens into right ventricle via tricuspid valve
Right Ventricle
- Crescent-shaped in cross-section; wall ~3-5 mm (low-pressure circuit)
- Internal: trabeculae carneae, moderator band (carries right bundle branch from septum to anterior papillary muscle - surgically important), three papillary muscles (anterior, posterior, septal)
- Outflow through pulmonary valve into pulmonary trunk
- Separated from LV by the interventricular septum
Left Atrium
- Forms most of the base of the heart
- Receives four pulmonary veins (2 from each lung)
- Smooth-walled; left auricle projects anteriorly
- Opens into left ventricle via mitral (bicuspid) valve
Left Ventricle
- Ellipsoid; wall ~8-12 mm; generates ~120 mmHg systolic pressure
- Two papillary muscles: anterolateral (supplied by LCx + LAD) and posteromedial (supplied by PDA only - most vulnerable to ischemia)
- Outflow through aortic valve into ascending aorta
4. Heart Valves and Cardiac Skeleton
The Four Valves
| Valve | Type | Cusps/Leaflets | Auscultation Site |
|---|---|---|---|
| Tricuspid | Atrioventricular (right) | 3: anterior, posterior, septal | Left lower sternal border |
| Mitral (bicuspid) | Atrioventricular (left) | 2: anterior, posterior | Apex (5th ICS MCL) |
| Pulmonary | Semilunar | 3 cusps | Left 2nd ICS |
| Aortic | Semilunar | 3 cusps: L, R, posterior (non-coronary) | Right 2nd ICS |
All valves open and close passively via pressure gradients. The AV valves are tethered by chordae tendineae to papillary muscles, preventing prolapse during systole.
Cardiac Skeleton
A framework of dense fibrous tissue that:
- Provides rigid attachment rings (annuli fibrosi) for all four valves
- Electrically insulates atria from ventricles (the AV bundle/His is the only electrical bridge)
- Provides myocardial attachment points
Components: fibrous rings of all four valves + right and left fibrous trigones (dense masses between aortic, mitral, and tricuspid rings)
5. Blood Supply - Coronary Arteries
Both coronary arteries arise from the aortic sinuses (sinuses of Valsalva) in the initial ascending aorta, just above the aortic valve leaflets. They are the first branches of the aorta. Their stems lie in the subepicardial fat of the coronary sulcus.
Right Coronary Artery (RCA)
Origin: Right aortic sinus
Course: Passes anteriorly, descends in the coronary sulcus between RA and RV; reaches the inferior (acute) margin, turns posteriorly onto the diaphragmatic surface and base of the heart
| Branch | Territory / Notes |
|---|---|
| SA nodal branch (from early atrial branch) | SA node - passes posteriorly around the SVC; present in ~60% from RCA |
| Right marginal branch | Acute margin of RV toward the apex |
| AV nodal branch | AV node - given off as RCA reaches the crux of the heart |
| Posterior interventricular artery (PDA) | Lies in posterior IV sulcus; supplies posterior 1/3 of IV septum |
Total territory of RCA:
- Right atrium and right ventricle
- SA and AV nodes (in right-dominant hearts)
- Interatrial septum + part of left atrium
- Posteroinferior 1/3 of the interventricular septum
- Posterior part of the left ventricle (diaphragmatic surface)
Left Coronary Artery (LCA / Left Main)
Origin: Left aortic sinus
Course: Short stem (1-2 cm) passes between pulmonary trunk and left auricle, then divides into two terminal branches
Branch 1: Anterior Interventricular Artery (LAD - Left Anterior Descending)
- Descends in the anterior interventricular sulcus toward the apex
- Wraps around the apex to anastomose with PDA on the posterior surface
| Sub-branch | Territory |
|---|---|
| Diagonal branches (1-3 large) | Anterolateral wall of LV |
| Septal perforating branches | Anterior 2/3 of IV septum including Bundle of His and bundle branches |
Branch 2: Circumflex Artery (LCx)
- Courses left in the coronary sulcus onto the base/diaphragmatic surface
- Usually ends before the posterior IV sulcus (in right-dominant hearts)
| Sub-branch | Territory |
|---|---|
| Left marginal (obtuse marginal) artery | Obtuse (left) margin of the LV |
| Posterior IV artery | Only present in left-dominant pattern |
Total territory of LCA:
- Most of left atrium and left ventricle
- Anterior 2/3 of the interventricular septum
- AV bundle (Bundle of His) and its branches
- Anterolateral papillary muscle
Right Dominant Pattern (most common)
Coronary Dominance
Dominance = determined by which vessel gives rise to the posterior descending artery (PDA) and supplies the diaphragmatic LV surface
| Pattern | Frequency | PDA from | Notes |
|---|---|---|---|
| Right dominant | ~70% | RCA | RCA large, LCx small |
| Codominant | ~20% | Both RCA and LCx | Both contribute to PDA territory |
| Left dominant | ~10% | LCx (enlarged) | RCA small; LCx supplies posterior LV; SA/AV nodes may be from LCx |
Important: Although coronary arteries form small anastomoses with each other, these are functionally insufficient for acute collateral rescue if a vessel occludes suddenly. Coronary arteries are therefore considered functional end arteries. Over 90% of acute MIs arise from fresh coronary thrombosis on a ruptured atherosclerotic plaque. - Color Atlas of Human Anatomy
Clinical Terminology
In clinical practice, anatomical names are shortened:
| Anatomical Name | Clinical Name |
|---|---|
| Short left coronary artery | Left main stem |
| Anterior interventricular artery | LAD (Left Anterior Descending) |
| Circumflex branch | LCx |
| Posterior interventricular artery | PDA (Posterior Descending Artery) |
| Right marginal artery | RMA or acute marginal |
| Left marginal artery | OM (Obtuse Marginal) |
6. Coronary Blood Flow Physiology
(Goldman-Cecil Medicine)
- Coronary arteries fill from the aorta just above the aortic valve
- Diastolic aortic pressure drives the majority of coronary flow - coronary vessels are compressed during systole by the contracting myocardium
- Subendocardial flow is almost exclusively diastolic (these vessels are compressed the most during systole)
- Epicardial vessels receive flow in both systole and diastole
- Coronary flow can increase up to 6-fold during exercise via: nitric oxide, adenosine, bradykinin, prostaglandins, CO₂
- This explains why the subendocardium is the most ischemia-vulnerable zone in hypotension, tachycardia, or severe aortic stenosis
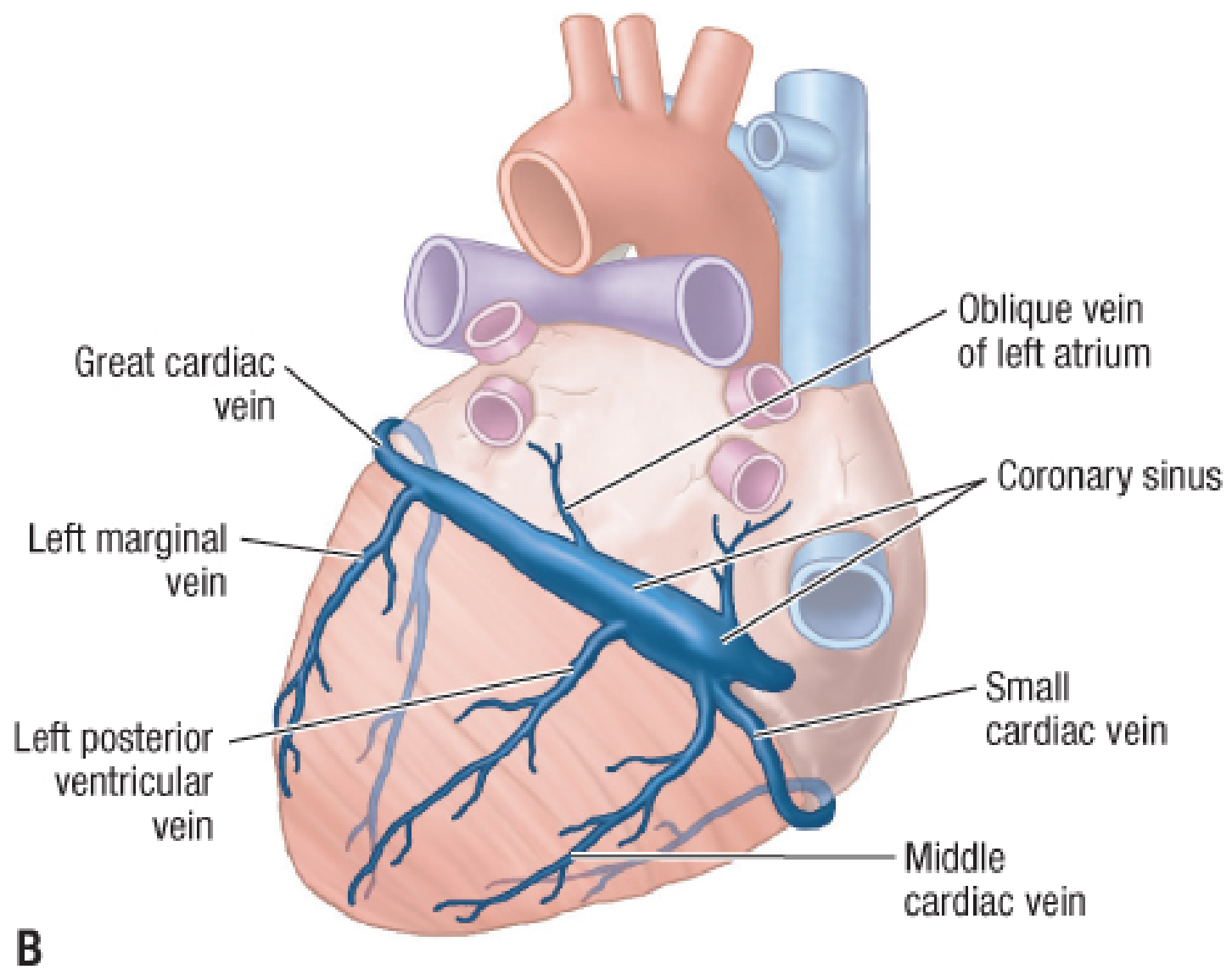
7. Venous Drainage - Cardiac Veins
Most venous blood (about two-thirds) drains into the coronary sinus, which lies in the posterior coronary sulcus between LA and LV, then opens into the right atrium between the IVC orifice and the right AV opening.
Tributaries of the Coronary Sinus
| Vein | Companion Artery | Course / Drains |
|---|---|---|
| Great cardiac vein (begins as anterior interventricular vein) | LAD | Starts at apex, ascends in anterior IV sulcus, then left in coronary sulcus into coronary sinus at its left end |
| Middle cardiac vein | PDA | Starts at apex, ascends in posterior IV sulcus, drains into right end of coronary sinus |
| Small cardiac vein | Right marginal artery | Right side of heart; turns posteriorly in coronary sulcus to right end of coronary sinus |
| Left posterior ventricular vein | - | Diaphragmatic LV surface → coronary sinus |
| Oblique vein of left atrium (of Marshall) | - | Left atrial wall → forms the beginning of the coronary sinus; embryological remnant of the left SVC |
Veins Bypassing the Coronary Sinus
| Vein | Drains Directly Into |
|---|---|
| Anterior cardiac veins (3-4 small veins) | Right atrium directly, crossing over RCA |
| Venae cordis minimae (Thebesian veins) | Directly into cardiac chambers (mostly atria); cause minor physiological right-to-left shunting |
8. Nerve Supply
| Type | Origin | Effect |
|---|---|---|
| Sympathetic | T1-T4 via superior, middle, inferior cervical cardiac nerves + thoracic cardiac nerves → cardiac plexus | ↑ heart rate (chronotropy), ↑ force (inotropy), coronary vasodilation |
| Parasympathetic | Vagus nerve (CN X) via cardiac branches → cardiac plexus | ↓ heart rate; slows AV conduction; little direct ventricular effect |
| Visceral afferents (pain) | Follow sympathetic fibers → enter spinal cord T1-T4 | Referred pain to left arm, jaw, epigastrium during ischemia |
The cardiac plexus lies anterior to the bifurcation of the trachea, with superficial and deep components. Stimulation of T1-T4 visceral afferents explains why cardiac pain is referred to the same dermatomes as the left arm and jaw.
9. Clinical Correlation - Artery Occlusion & Infarct Territory
| Artery Occluded | Zone of Infarction | ECG Changes | Other Effects |
|---|---|---|---|
| LAD (most common) | Anterior wall + anterior septum of LV | ST elevation V1-V4 | Bundle branch blocks; anterior wall motion abnormality |
| RCA | Inferior wall of LV; RV; SA/AV nodes | ST elevation II, III, aVF | Bradycardia, AV blocks (especially in right-dominant hearts) |
| LCx | Lateral/posterior LV wall | ST elevation I, aVL, V5-V6 (or posterior changes V1-V2) | Posteromedial papillary muscle ischemia → mitral regurgitation |
| Left main | Massive - both LAD + LCx territories | Global ST changes | Cardiogenic shock; often fatal |
The posteromedial papillary muscle has single blood supply (PDA) making it far more vulnerable to ischemia and rupture causing acute mitral regurgitation than the anterolateral papillary muscle (dual supply).
Sources:
- Gray's Anatomy for Students (9780323934237)
- Goldman-Cecil Medicine (9780323930345)
- Color Atlas of Human Anatomy Vol. 2 - Internal Organs (9783132424487)
- Fischer's Mastery of Surgery 8th Edition (9781975176433)
This is a shared conversation. Sign in to Orris to start your own chat.