Q. Describe the etiopathology, clinical features and management of malignant otitis externa in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
malignant otitis externa etiopathology Pseudomonas aeruginosa diabetic immunocompromised
search_medical_text
malignant necrotizing otitis externa clinical features diagnosis management treatment
search_medical_image
malignant otitis externa CT scan MRI imaging skull base osteomyelitis
GradeResponse
GradeResponse
GradeResponse
search_medical_text
malignant otitis externa antibiotics ciprofloxacin surgical treatment prognosis staging
search_medical_text
necrotizing otitis externa cranial nerve palsy facial nerve skull base osteomyelitis complications
Here is a comprehensive, examination-ready answer on Malignant Otitis Externa (MOE) for 50 marks, compiled from Harrison's Principles of Internal Medicine (21st ed.), Scott-Brown's Otorhinolaryngology, Cummings Otolaryngology, Dhingra's Diseases of Ear Nose and Throat, Stell & Maran's Head and Neck Surgery, Hazarika's Textbook of ENT, and peer-reviewed literature.
MALIGNANT OTITIS EXTERNA (Necrotizing Otitis Externa)
1. DEFINITION
Malignant Otitis Externa (MOE), also called Necrotizing Otitis Externa (NOE), is an aggressive, potentially life-threatening osteomyelitis of the external auditory canal (EAC) and skull base, predominantly caused by Pseudomonas aeruginosa, occurring almost exclusively in immunocompromised and elderly diabetic patients.
The term "malignant" was coined by Chandler (1968) — not to imply neoplasia, but to emphasize its aggressive and life-threatening nature. Many modern authors prefer "necrotizing" as it is more pathologically accurate. (Scott-Brown's Otorhinolaryngology, 8th ed.)
2. EPIDEMIOLOGY
| Parameter | Details |
|---|---|
| Age | Predominantly elderly (>60 years) |
| Sex | Males > Females |
| Underlying condition | Diabetes mellitus (~90% of cases) |
| Other associations | HIV/AIDS, hematological malignancies, organ transplant, long-term steroid use |
| Causative organism | Pseudomonas aeruginosa (>95%) |
| Rare organisms | Aspergillus spp. (in non-diabetic immunocompromised), Staphylococcus, Proteus |
| Mortality (historical) | Up to 50%; reduced to <15% with modern treatment |
3. ETIOPATHOLOGY
3a. Predisposing Factors
┌─────────────────────────────────────────────────────────────────────┐
│ PREDISPOSING CONDITIONS │
│ │
│ Diabetes Mellitus (most common) ─────────────────────────────┐ │
│ • Microangiopathy → reduced tissue perfusion │ │
│ • Impaired neutrophil function (chemotaxis, phagocytosis) │ │
│ • Impaired T-cell mediated immunity ├──► SUSCEPTIBILITY │
│ │ │
│ Immunocompromise │ │
│ • HIV/AIDS (CD4 <200) │ │
│ • Post-chemotherapy, organ transplant │ │
│ • Long-term corticosteroid therapy │ │
│ • Hematological malignancies (leukemia, lymphoma) ┘ │
└─────────────────────────────────────────────────────────────────────┘
3b. Causative Organisms
- Primary: Pseudomonas aeruginosa — a Gram-negative, oxidase-positive bacillus
- Produces exotoxin A (inhibits protein synthesis), elastase, phospholipase C, pyocyanin
- These enzymes destroy cartilage, soft tissue, and bone
- Forms biofilms resistant to antibiotics and host immunity
- Fungal (rare): Aspergillus fumigatus / Aspergillus flavus — seen in non-diabetic immunocompromised (HIV, post-transplant). More aggressive, worse prognosis (Cummings, 7th ed., p. 2007)
- Others: Staphylococcus aureus, Klebsiella, Proteus mirabilis (rare)
3c. Pathogenesis
┌─────────────────────────────────────────────────────────────────────────────────┐
│ PATHOGENESIS OF MOE │
│ │
│ P. aeruginosa colonizes │
│ external auditory canal (EAC) │
│ │ │
│ ▼ │
│ Impaired local immunity (diabetic microangiopathy, earwax changes) │
│ │ │
│ ▼ │
│ Infection of skin of EAC → Perichondritis → Chondritis │
│ │ │
│ ▼ │
│ Spread through FISSURES OF SANTORINI │
│ (defects in cartilaginous floor of EAC) │
│ │ │
│ ├──────────────────────────────────────────────────┐ │
│ ▼ ▼ │
│ PAROTID space / TMJ MASTOID / MIDDLE EAR │
│ │ │ │
│ ▼ ▼ │
│ Infratemporal fossa SKULL BASE OSTEOMYELITIS │
│ │ │ │
│ └──────────────────┬─────────────────────────┘ │
│ ▼ │
│ CRANIAL NERVE INVOLVEMENT │
│ (VII → IX → X → XI → XII) │
│ │ │
│ ▼ │
│ Sigmoid sinus thrombosis / Meningitis / Brain abscess │
│ │ │
│ ▼ │
│ DEATH │
└─────────────────────────────────────────────────────────────────────────────────┘
Key anatomical pathway: The fissures of Santorini (surgical defects in the cartilaginous EAC floor) and the osseocartilaginous junction are the critical portals of deep spread. From the floor of the EAC, infection tracks into the stylomastoid foramen (VII nerve), then to the jugular foramen (IX, X, XI), then across the skull base to the hypoglossal canal (XII). (Dhingra, 7th ed.)
3d. Role of Diabetes in Pathogenesis
- Microangiopathy → reduced oxygen delivery → impaired healing
- Hyperglycemia → acidic tissue environment → Pseudomonas thrives
- Reduced cerumen secretion (antibacterial barrier lost)
- Neutrophil dysfunction → reduced phagocytosis and oxidative burst
- ESR >100 mm/hr common, correlating with disease activity (Hazarika)
4. CLINICAL FEATURES
4a. Symptoms (by Stage)
Stage I — Early (Soft Tissue Stage)
- Severe, unrelenting otalgia (disproportionate to local findings — hallmark)
- Otorrhoea — purulent, foul-smelling
- Decreased hearing (CHL due to debris)
- Granulation tissue at osseocartilaginous junction (floor of EAC at 6 o'clock position) — pathognomonic clinical finding
- Tenderness anterior to tragus, extending to TMJ
Stage II — Bone Invasion (Osteomyelitis Stage)
- All above features + worsening
- Facial nerve palsy (VII) — most common CN involved (50–67% of cases); seen at stylomastoid foramen involvement
- TMJ involvement → trismus, jaw pain
- Parotid gland involvement → parotid swelling
Stage III — Skull Base / Intracranial Stage
- Glossopharyngeal (IX), Vagus (X), Accessory (XI) — jugular foramen syndrome (Vernet's syndrome)
- Hypoglossal (XII) — tongue deviation
- Abducens (VI) — diplopia (Gradenigo's extension)
- Sigmoid sinus thrombosis
- Meningitis, epidural abscess, brain abscess
- Septicaemia → multiorgan failure
4b. Signs
| Sign | Significance |
|---|---|
| Granulation tissue at EAC floor (osseocartilaginous junction) | Pathognomonic of MOE |
| Tenderness at tragus / preauricular region | Extension to parotid/TMJ |
| Facial nerve palsy (LMN type) | Stylomastoid foramen involvement |
| Trismus | TMJ/infratemporal fossa involvement |
| Multiple CN palsies | Skull base osteomyelitis |
| Normal TM (usually) | Infection tracks below, not through TM |
"The tympanic membrane is often intact in MOE — this distinguishes it from chronic otitis media with bone erosion." (Scott-Brown's, 8th ed.)
5. INVESTIGATIONS
5a. Laboratory
| Test | Findings / Significance |
|---|---|
| Blood glucose | Elevated (diabetes control) |
| ESR | Markedly elevated (>100 mm/hr); used for monitoring response |
| CRP | Elevated; monitor treatment response |
| CBC | Leukocytosis (may be absent in immunocompromised) |
| HbA1c | Assesses chronic diabetic control |
| Ear swab culture & sensitivity | Confirm P. aeruginosa; guide antibiotics |
| Blood culture | Positive in septicaemia |
5b. Imaging
CT Scan (Investigation of Choice for Bone)
- Shows erosion of cortical bone of EAC, mastoid, skull base
- Identifies soft tissue extension, parapharyngeal involvement
- Limitations: Bone changes lag behind clinical improvement — not ideal for monitoring
MRI (Best for Soft Tissue / Intracranial Extension)
- T1: Low signal in marrow (osteomyelitis)
- T2: High signal in soft tissue edema/abscess
- Gadolinium-enhanced T1: Shows extent of granulation tissue, dural involvement, cavernous sinus thrombosis
- "Ink smudge" pattern on T2 — characteristic of Pseudomonas granulation tissue (Harrison's 21st ed., p. 4839)
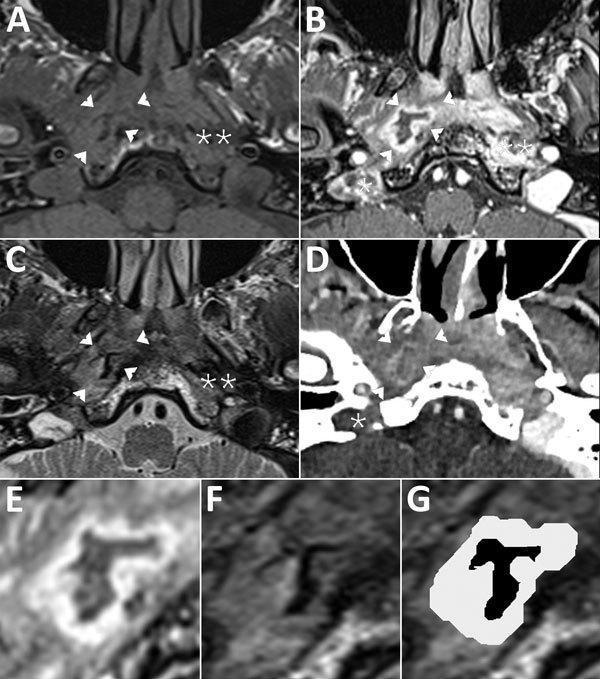
Composite MRI/CT scan of MOE: Panel A (T1 MRI), B/E (Gd-enhanced T1 with fat sat), C/F/G (T2 MRI), D (iodine CT). Findings: right parapharyngeal abscess (arrowheads) with 'ink smudge' T2 pattern, right jugular vein/bulb thrombosis (single asterisk), deep-space cellulitis in carotid and perivertebral spaces (double asterisks), and osteolysis of mastoid, styloid, and occipital bones — indicating extensive skull base osteomyelitis. (PMC Clinical VQA Dataset)
Radionuclide Scanning
| Scan | Isotope | Use |
|---|---|---|
| Technetium-99m bone scan | ⁹⁹ᵐTc-MDP | Early diagnosis; high sensitivity but low specificity; positive even early when CT is normal |
| Gallium-67 scan | ⁶⁷Ga-citrate | Specific for active infection; used for monitoring treatment response — normalises when infection resolves |
| Indium-111 WBC scan | ¹¹¹In | Acute phase; high sensitivity for active osteomyelitis |
"Gallium scan is the gold standard for monitoring treatment response in MOE — it normalises with resolution of infection, unlike the bone scan which may remain positive for months." (Cummings, 7th ed.)
PET-CT (Recent Advance)
- 18F-FDG PET-CT has emerged as superior to gallium scintigraphy for monitoring
- High sensitivity (~100%) and specificity (~93%)
- Guides duration of antibiotic therapy (Rubin Grandis, 2020; Laryngoscope)
6. DIAGNOSTIC CRITERIA
Chandler's Criteria (1968):
- Elderly diabetic
- Severe persistent otalgia
- Purulent otorrhoea
- Granulation tissue in EAC
- Growth of P. aeruginosa
- Failure to respond to conventional treatment
Levenson's Criteria (Modified):
Major criteria: Refractory otorrhoea >1 month, granulation tissue in EAC, osteomyelitis on imaging
Minor criteria: DM/immunosuppression, positive culture for P. aeruginosa, ESR >100
7. STAGING (Chandler's / Cohen's Classification)
| Stage | Features |
|---|---|
| Stage I | Soft tissue only — EAC, perichondritis, no bone erosion |
| Stage II | Bone involvement (EAC floor/mastoid), granulation, mild CN involvement |
| Stage III | Skull base osteomyelitis, multiple CN palsies |
| Stage IV | Intracranial extension, meningitis, sinus thrombosis, brain abscess |
Facial nerve involvement correlates with Stage III; involvement of lower cranial nerves (IX–XII) indicates Stage IV in many classifications (Stell & Maran, 5th ed.)
8. DIFFERENTIAL DIAGNOSIS
| Condition | Differentiating features |
|---|---|
| Simple otitis externa | Mild, responds to topical treatment; no granulation at osseocartilaginous junction |
| Carcinoma of EAC | Biopsy shows malignant cells; does not respond to antibiotics |
| Ramsay Hunt syndrome | Herpetic vesicles, CN VII palsy, no bone erosion |
| Cholesteatoma with erosion | TM perforation, cholesteatoma pearl, CT shows expansion |
| Osteomyelitis from OM | TM perforation, chronic discharge; CT differentiates |
9. MANAGEMENT
MANAGEMENT FLOWCHART
┌────────────────────────────────────────────────────────────────┐
│ SUSPECTED MALIGNANT OTITIS EXTERNA │
│ (Severe otalgia + Granulation in EAC + DM/Immunocomp.) │
└──────────────────────────────┬─────────────────────────────────┘
│
┌───────────────▼───────────────┐
│ CONFIRM DIAGNOSIS │
│ • Ear swab C&S │
│ • Blood glucose, ESR, CRP │
│ • CT temporal bone / MRI │
│ • Tc-99 bone scan / PET-CT │
└───────────────┬───────────────┘
│
┌───────────────▼───────────────┐
│ HOSPITALIZATION │
│ (All cases — initially) │
└───────────────┬───────────────┘
│
┌──────────────────────┼────────────────────────┐
▼ ▼ ▼
MEDICAL SURGICAL ADJUNCTIVE
MANAGEMENT MANAGEMENT MEASURES
(Primary) (If needed)
│ │ │
▼ ▼ ▼
• IV Ciprofloxacin • Debridement EAC • Diabetic control
(anti-pseudomonal) • Biopsy (r/o Ca) • Hyperbaric O₂
• ± Aminoglycoside • Rarely: mastoidectomy • Nutritional support
• Topical treatment • Facial nerve • Pain management
• Duration 6–8 wks decompression (rarely) • Gallium scan monitoring
│
▼
MONITOR RESPONSE
• ESR/CRP weekly
• Gallium scan / PET-CT
• Symptoms regression
│
┌────┴────┐
▼ ▼
IMPROVED NOT IMPROVED
Step down Switch antibiotics
oral Cipro Surgical debridement
6–12 wks Hyperbaric O₂
9a. Medical Management (Mainstay)
First-Line Antibiotic Therapy
| Antibiotic | Route | Dose | Notes |
|---|---|---|---|
| Ciprofloxacin (drug of choice) | IV then oral | 400 mg IV BD → 750 mg oral BD | Anti-pseudomonal fluoroquinolone; excellent bone penetration; oral bioavailability ~80% |
| Piperacillin-Tazobactam | IV | 4.5 g TDS | For resistant strains |
| Ceftazidime | IV | 2 g TDS | 3rd gen cephalosporin; anti-pseudomonal |
| Imipenem/Meropenem | IV | 500 mg QID | Carbapenem; for multi-drug resistant Pseudomonas |
| Tobramycin / Gentamicin | IV | Dose-adjusted | Synergy with beta-lactams; monitor nephrotoxicity |
Duration: Minimum 6–8 weeks IV antibiotics, followed by oral ciprofloxacin for 6–12 weeks total. Duration guided by gallium scan / PET-CT normalization and ESR normalization, not just clinical improvement. (Cummings, 7th ed.)
For Fungal MOE (Aspergillus)
- Voriconazole — drug of choice (200 mg BD)
- Liposomal Amphotericin B — alternative
- Duration: minimum 12–16 weeks (Harrison's, 21st ed.)
Topical Therapy
- Ciprofloxacin ear drops (0.3%) — adjunctive
- Aural toilet and regular cleaning of EAC debris
- Acetic acid 2% drops (not sufficient alone; adjunct only)
9b. Control of Diabetes
- Tight glycaemic control is critical — improves neutrophil function, tissue perfusion, and response to antibiotics
- IV insulin infusion in acute phase; target blood glucose 6–10 mmol/L
- HbA1c must be optimized during prolonged antibiotic therapy
9c. Surgical Management
Surgery plays a secondary/adjunctive role in MOE. Primary surgical indications are:
| Indication | Procedure |
|---|---|
| Diagnostic uncertainty (rule out carcinoma) | Biopsy of granulation tissue — mandatory |
| Debulking of necrotic tissue | Local debridement of EAC |
| Abscess formation | Incision and drainage |
| Failed medical therapy with localized mastoid disease | Mastoidectomy (canal wall down) — rarely needed |
| Facial nerve palsy with evidence of nerve compression | Facial nerve decompression — controversial |
| Intracranial complications | Neurosurgical referral |
"Radical surgery is no longer recommended as the primary modality; aggressive medical therapy with prolonged anti-pseudomonal antibiotics has replaced the surgical approach." (Zakir Hussain, ENT Surgery, 3rd ed.)
9d. Hyperbaric Oxygen Therapy (HBO)
- Mechanism: Increases tissue pO₂ in hypoxic bone → enhanced neutrophil bactericidal activity → improved antibiotic penetration
- Indication: Refractory cases, multiple cranial nerve palsies, failed first-line antibiotics
- Protocol: 2.0–2.4 atmospheres, 100% oxygen, 90 min sessions, 30–60 sessions
- Evidence: Case series show benefit in refractory and fungal MOE (Mader, 1989; Ress, 2003)
- Not universally available; limited to tertiary centres (Scott-Brown's, 8th ed.)
9e. Monitoring Treatment Response
MONITORING PROTOCOL FOR MOE
━━━━━━━━━━━━━━━━━━━━━━━━━━━
Weekly:
→ ESR, CRP, blood glucose
→ Clinical assessment (pain, otorrhoea, granulation)
Every 4 weeks:
→ MRI (soft tissue response)
→ CT if bone progression suspected
End of therapy:
→ Gallium-67 scan / PET-CT
→ ONLY discontinue antibiotics if scan NORMALIZES
→ ESR should return to near-normal (<30 mm/hr)
━━━━━━━━━━━━━━━━━━━━━━━━━━━
10. COMPLICATIONS
| Complication | Mechanism | Outcome |
|---|---|---|
| Facial nerve palsy | Stylomastoid foramen osteomyelitis | 50% partial recovery |
| Jugular foramen syndrome (Vernet's) | IX, X, XI involvement | Poor prognosis |
| Sigmoid sinus thrombosis | Direct extension | Septic emboli, pulmonary abscess |
| Meningitis | Intracranial extension | High mortality |
| Brain abscess | Haematogenous or direct | Neurosurgical emergency |
| Petrous apicitis | Extension medially | Gradenigo's syndrome (VI palsy + ipsilateral facial pain) |
| Death | Sepsis, intracranial complications | Mortality 10–20% modern era; was 50% pre-antibiotic era |
11. PROGNOSIS
| Prognostic Factor | Good Prognosis | Poor Prognosis |
|---|---|---|
| CN involvement | None | Multiple CN palsies |
| Causative organism | P. aeruginosa | Aspergillus |
| Underlying condition | Controlled DM | HIV, malignancy |
| Gallium scan at 6 weeks | Normalizing | Persistently positive |
| Response to antibiotics | Rapid | Slow/refractory |
| Intracranial extension | Absent | Present |
- Recurrence rate: 9–27% even after apparent cure — long-term follow-up essential (Cummings)
- Facial nerve palsy recovery: Partial in 50–60%; full recovery uncommon once palsied (Dhingra, 7th ed.)
12. RECENT ADVANCES (RGUHS-Relevant)
12a. Diagnostic Advances
- 18F-FDG PET-CT: Now considered superior to Gallium-67 scanning for both initial staging and monitoring treatment response. Standardised Uptake Value (SUV) can be quantified (Stern Ginat et al., Laryngoscope 2020)
- Diffusion-weighted MRI (DWI): Detects subtle intracranial complications earlier than conventional MRI
- PCR-based pathogen identification: Faster than conventional culture; identifies resistant genes (e.g., OXA-type carbapenemases in Pseudomonas)
12b. Therapeutic Advances
- Oral ciprofloxacin step-down therapy: Validated for stable patients after initial IV therapy; equivalent outcomes to prolonged IV (Grandis et al.)
- Ceftolozane-tazobactam / Ceftazidime-avibactam: New beta-lactam/beta-lactamase inhibitor combinations for MDR Pseudomonas in MOE (FDA approved; Infectious Diseases Society of America 2022)
- Voriconazole monotherapy for Aspergillus MOE: replaced Amphotericin B as first-line (ESCMID 2022 guidelines)
- Anti-biofilm strategies: Gallium nitrate (disrupts Pseudomonas iron metabolism and biofilm) — experimental
- Immunotherapy adjuncts: G-CSF (granulocyte colony-stimulating factor) in neutropenic MOE — investigational
12c. Fungal MOE (Emerging Entity)
- Increasing incidence with rising immunosuppression (post-COVID, biologics, immunotherapy)
- Aspergillus MOE: earlier intracranial spread, worse prognosis, does NOT respond to ciprofloxacin
- Voriconazole TDM (therapeutic drug monitoring) essential for dosing (Sohal et al., 2021)
13. SUMMARY TABLE
| Parameter | Details |
|---|---|
| Organism | P. aeruginosa (95%), Aspergillus (rare) |
| Population | Elderly diabetics, immunocompromised |
| Hallmark sign | Granulation tissue at EAC floor (osseocartilaginous junction) |
| Key symptom | Severe unrelenting otalgia disproportionate to signs |
| Most common CN | Facial nerve (VII) |
| Best investigation | MRI + Gallium-67 scan / PET-CT |
| Drug of choice | Ciprofloxacin (IV then oral) for 6–12 weeks |
| Monitoring | ESR, CRP, Gallium-67 scan normalization |
| Prognosis marker | Gallium scan normalization + ESR |
| Poor prognostic sign | Multiple CN palsies, Aspergillus, intracranial extension |
14. REFERENCES
- Harrison's Principles of Internal Medicine, 21st Edition — p. 4839 (Pseudomonas and MOE)
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery, 8th Edition — Chapter on Otitis Externa
- Cummings Otolaryngology — Head and Neck Surgery, 7th Edition — Chapter 137: Infections of the External Ear
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th Edition — Chapter 5: Diseases of External Ear
- Stell & Maran's Head and Neck Surgery and Oncology, 5th Edition
- Hazarika P — Textbook of Ear Nose and Throat Diseases, 12th Edition
- Zakir Hussain — ENT Surgery (Practical ENT), 3rd Edition
- Chandler JR (1968) — Original description of MOE; Laryngoscope 78:1257–1294
- Grandis JR et al. (1995) — Ciprofloxacin in MOE; Laryngoscope
- Stern Ginat D et al. (2020) — PET-CT in MOE monitoring; Laryngoscope
- ESCMID/ECMM/ERS 2022 Guidelines — Aspergillosis management
RGUHS Examination Tip: MOE is a high-yield topic in ENT theory exams. Key points to always include: (1) Fissures of Santorini as spread pathway, (2) Granulation at osseocartilaginous junction as pathognomonic sign, (3) Gallium scan for monitoring (not CT), (4) Ciprofloxacin as DOC, (5) Staging by CN involvement, (6) PET-CT as a recent advance replacing Gallium scanning.
This is a shared conversation. Sign in to Orris to start your own chat.