Q. Describe the various audiological tests for retrocochlear pathology. in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
search_medical_text
audiological tests retrocochlear pathology pure tone audiometry speech tests
search_medical_text
ABR auditory brainstem response BAER retrocochlear lesion acoustic neuroma
search_medical_image
audiological tests retrocochlear pathology ABR BAEP diagram
GradeResponse
GradeResponse
GradeResponse
search_medical_text
SISI test tone decay test Bekesy audiometry retrocochlear stapedius reflex
search_medical_text
acoustic neuroma vestibular schwannoma diagnosis audiometry speech discrimination rollover
Here is a comprehensive, exam-ready answer for a 50-mark RGUHS question on audiological tests for retrocochlear pathology, synthesized from Harrison's Principles of Internal Medicine (21st Ed.), Scott-Brown's Otorhinolaryngology, Cummings Otolaryngology, Dhingra, Hazarika, Zakir Hussain, Stell & Maran, and relevant literature.
Audiological Tests for Retrocochlear Pathology
Introduction
Retrocochlear pathology refers to lesions affecting the auditory pathway proximal to the cochlea — i.e., the VIII nerve (cochlear division), cochlear nuclei, and central auditory pathways up to the auditory cortex. The most common and clinically significant retrocochlear lesion is vestibular schwannoma (acoustic neuroma), though other causes include meningioma, multiple sclerosis, cerebellopontine angle (CPA) tumors, brainstem infarcts, and demyelinating diseases.
The hallmark audiological feature is disproportionately poor speech discrimination relative to pure tone thresholds and abnormal fatigue (tone decay) of the auditory nerve.
Classification of Audiological Tests for Retrocochlear Pathology
┌────────────────────────────────────────────────────┐
│ AUDIOLOGICAL TESTS FOR RETROCOCHLEAR │
│ PATHOLOGY │
└───────────────────┬────────────────────────────────┘
│
┌─────────────┼──────────────────┐
▼ ▼ ▼
BEHAVIORAL ELECTROPHYSIOLOGICAL ACOUSTIC
TESTS TESTS IMMITTANCE
│ │ TESTS
│ │ │
┌─────┴────┐ ┌──────┴──────┐ ┌────┴────────┐
│Pure Tone │ │ ABR/BAEP │ │ Acoustic │
│Audiometry│ │ (BERA) │ │ Reflex │
│ │ │ │ │ Decay Test │
│Speech │ │ ECochG │ │ │
│Audiometry│ │ │ │ Acoustic │
│(SDS,PI-PB│ │ ASSR │ │ Reflex │
│Rollover) │ │ │ │ Threshold │
│ │ │ ACAEP/CAEP │ └─────────────┘
│Tone Decay│ │ │
│(ABLB/ │ └─────────────┘
│Carhart) │
│ │
│SISI │
│ │
│Bekesy │
│Audiometry│
└──────────┘
A. BEHAVIORAL (PSYCHOACOUSTIC) TESTS
1. Pure Tone Audiometry (PTA)
Principle: Measures hearing thresholds at frequencies 250–8000 Hz for both air conduction (AC) and bone conduction (BC).
Retrocochlear features on PTA:
- Sensorineural hearing loss (SNHL), usually unilateral
- Loss is more pronounced at high frequencies (sloping audiogram)
- Air-bone gap is absent (purely sensorineural)
- The degree of loss may appear mild to moderate, but speech discrimination is disproportionately poor
| Feature | Cochlear | Retrocochlear |
|---|---|---|
| Audiogram shape | Flat/sloping | Sloping; may be flat |
| Recruitment | Present | Absent |
| Tone decay | Absent/mild | Marked (>30 dB) |
| Speech discrimination | Commensurate | Disproportionately poor |
| Bekesy | Type II | Type III/IV |
(Dhingra, Diseases of ENT Head & Neck Surgery, 7th Ed.)
2. Speech Audiometry
A. Speech Recognition Threshold (SRT)
- Defined as the lowest intensity at which 50% of spondee words are correctly repeated.
- In retrocochlear lesions: SRT-PTA gap may be wide (SRT worse than expected from PTA).
B. Speech Discrimination Score (SDS) / Word Recognition Score (WRS)
- Uses phonetically balanced (PB) word lists at comfortable loudness level.
- Retrocochlear pattern: SDS is disproportionately poor (often <50%) compared to the degree of pure tone loss.
C. Performance-Intensity Function for PB words (PI-PB / Rollover)
- At increasing intensities, WRS initially rises then falls — this fall is called Rollover.
WRS (%)
100 ┤ ●●
80 ┤ ● ●
60 ┤ ● ● ← Rollover (Retrocochlear)
40 ┤ ●
20 ┤ ●
0 ┤────────────────────
20 40 60 80 100
Intensity (dB SL)
- Rollover Index (RI) = (Maximum PB score − Score at highest intensity) / Maximum PB score
- RI > 0.45 is significant for retrocochlear pathology (Jerger & Jerger, 1971)
- This is one of the most sensitive behavioral indicators of VIII nerve lesion (Scott-Brown, 8th Ed., Vol. 2)
3. Tone Decay Tests (Auditory Adaptation Tests)
Principle: The auditory nerve fatigues abnormally fast in retrocochlear lesions (excessive adaptation). A continuous tone is presented; the patient signals as long as they can hear it.
A. Carhart's Tone Decay Test
- A tone is presented 5 dB above threshold.
- If heard for <60 seconds → intensity raised by 5 dB.
- Process repeated.
- Total decay > 30 dB = retrocochlear (Carhart, 1957)
B. Rosenberg Tone Decay Test
- Tone presented at threshold for 60 seconds.
- Noted how many dB must be added to maintain audibility.
- >30 dB decay in 60 seconds = positive for retrocochlear pathology.
C. Olsen-Noffsinger Tone Decay Test
- Threshold-level presentation for 60 seconds.
- Grading:
- 0–5 dB: Normal
- 5–10 dB: Slight
- 15–20 dB: Moderate
- 25–30 dB: Marked retrocochlear
FLOW CHART — Tone Decay Test (Carhart's)
[Present tone at threshold + 5 dB]
↓
[Patient hears for 60 sec?]
YES ↙ NO ↘
[NORMAL] [Increase intensity by 5 dB]
↓
[Repeat until heard for 60 sec]
↓
[Calculate total dB added above threshold]
↓
>30 dB added → RETROCOCHLEAR
<15 dB → NORMAL/COCHLEAR
(Hazarika, Textbook of ENT Head & Neck Surgery)
4. SISI Test (Short Increment Sensitivity Index)
Principle: Tests ability to detect 1 dB increments superimposed on a continuous tone 20 dB above threshold.
- 20 increments are presented; each correct detection = 5% score.
| Score | Interpretation |
|---|---|
| 0–20% | NEGATIVE = Retrocochlear or normal |
| 20–70% | Indeterminate |
| 70–100% | POSITIVE = Cochlear (recruitment) |
- Retrocochlear lesions give LOW SISI scores (0–20%) because recruitment is absent.
- (Zakir Hussain, ENT Textbook)
5. Alternate Binaural Loudness Balance Test (ABLB)
- Applicable only in unilateral hearing loss.
- A tone is alternated between ears; patient adjusts intensity in affected ear to match loudness in normal ear.
- Laddering pattern absent in retrocochlear (no recruitment).
- Retrocochlear: No recruitment (loudness grows at normal or subnormal rate).
6. Bekesy Audiometry
Principle: Patient controls tone intensity in response to continuous (C) and interrupted (I) tones across frequencies.
| Type | Description | Pathology |
|---|---|---|
| Type I | C and I traces overlap | Normal / CHL |
| Type II | C trace drops 10–20 dB below I at high frequencies | Cochlear SNHL |
| Type III | C trace drops rapidly below I, crossing by 1000 Hz | Retrocochlear (severe) |
| Type IV | C trace drops 20–25 dB below I from low frequencies | Retrocochlear |
| Type V | I trace drops below C | Non-organic HL |
- Types III and IV are pathognomonic of retrocochlear lesions, especially acoustic neuroma.
- (Scott-Brown, Otorhinolaryngology Head & Neck Surgery; Cummings, 6th Ed.)
Bekesy Audiogram — Retrocochlear (Type III)
dB HL
0 ─────────────────── Interrupted (I)
10 ─────────
20 ──────
30 ────────────────────────── Continuous (C)
40 ───────────────────────────────────────
250 500 1k 2k 4k 8k Hz
↑
Crossover at ~1000 Hz → TYPE III → RETROCOCHLEAR
B. ACOUSTIC IMMITTANCE TESTS
7. Acoustic Reflex (Stapedius Reflex) Testing
The stapedius reflex (SR) is mediated via: Cochlea → CN VIII → Cochlear nucleus → Superior olivary complex → Facial nucleus → CN VII → Stapedius muscle.
In retrocochlear pathology:
- Reflex present at normal thresholds but DECAYS on sustained stimulus (most important sign)
- Elevated or absent acoustic reflex threshold at ipsilateral and contralateral sides
- Retrocochlear lesions on the afferent arc (CN VIII) cause absent ipsilateral AND contralateral reflex when the affected ear is stimulated.
Acoustic Reflex Decay Test
ACOUSTIC REFLEX DECAY TEST PROTOCOL
[Present 500 Hz or 1000 Hz tone at 10 dB above reflex threshold]
↓
[Observe reflex response for 10 seconds]
↓
[Measure amplitude at 0 sec and 5 sec]
↓
Amplitude at 5 sec / Amplitude at 0 sec
↓
< 50% (i.e., decay >50%) = POSITIVE = RETROCOCHLEAR
≥ 50% remaining = NORMAL
- Positive Decay = amplitude falls to <50% of initial within 5 seconds at 500 Hz or 1000 Hz
- Sensitivity ~65–85% for acoustic neuroma (Cummings Otolaryngology, 6th Ed.)
Acoustic Reflex Pattern Summary
| Probe Ear | Stimulus Ear | Normal | Cochlear HL | Retrocochlear (CN VIII lesion) |
|---|---|---|---|---|
| Right | Right (ipsilateral) | Present | Elevated | Absent |
| Left | Right (contralateral) | Present | Present | Absent |
| Right | Left (contralateral) | Present | Present | Present |
| Left | Left (ipsilateral) | Present | Elevated | Present |
(Stell & Maran's Head and Neck Surgery)
C. ELECTROPHYSIOLOGICAL TESTS
8. Auditory Brainstem Response (ABR) / Brainstem Evoked Response Audiometry (BERA) / BAEP
This is the GOLD STANDARD electrophysiological test for retrocochlear pathology.
Principle: Click stimuli elicit a series of electrical potentials from the auditory nerve and brainstem, recorded via scalp electrodes and averaged by computer.
ABR Wave Generators (Neural Sources)
┌─────────────────────────────────────────────────────────┐
│ ABR WAVEFORM COMPONENTS │
├────────┬───────────────────────────────────────────────┤
│ Wave I │ Distal VIII nerve (cochlear end) │
│ Wave II │ Proximal VIII nerve / cochlear nucleus │
│ Wave III│ Superior olivary complex (pons) │
│ Wave IV │ Lateral lemniscus / Nuclei │
│ Wave V │ Inferior colliculus (most robust, most used) │
└────────┴───────────────────────────────────────────────┘
(Harrison's Principles of Internal Medicine, 21st Ed., p. 1041)
Normal ABR Absolute Latencies
| Wave | Normal Latency (ms) |
|---|---|
| Wave I | ~1.5 ms |
| Wave III | ~3.5–3.8 ms |
| Wave V | ~5.5–5.8 ms |
Inter-peak Latencies (IPL) — Most Diagnostically Useful
| Interval | Normal | Retrocochlear (Abnormal) |
|---|---|---|
| I–III IPL | 2.0–2.2 ms | > 2.5 ms |
| III–V IPL | 2.0 ms | > 2.4 ms |
| I–V IPL | 4.0–4.4 ms | > 4.6 ms (KEY finding) |
| Inter-aural Wave V latency difference | < 0.4 ms | > 0.4 ms |
ABR Abnormalities in Retrocochlear Lesions:
- Prolonged I–V inter-peak latency (most sensitive)
- Prolonged III–V IPL (more specific for central lesion)
- Absent or poorly formed waves beyond Wave I (Wave I present but no III/V)
- Inter-aural latency difference for Wave V > 0.4 ms
- Complete absence of all waves (profound involvement)
- Increased I–III IPL with normal III–V (CN VIII/pontine junction lesion)
ABR in Retrocochlear vs. Cochlear Lesion
Normal ABR:
─────────────────────────────────────────
I II III IV V
↑ ↑ ↑
1.5ms 3.8ms 5.8ms
Cochlear SNHL (Threshold shift only):
─────────────────────────────────────────
All waves present, normal IPL, may have
elevated thresholds; wave V latency may
shift with hearing level
Retrocochlear ABR (Acoustic Neuroma):
─────────────────────────────────────────
I (III absent/late)
↑ ← Absent/flat beyond →
1.5ms Waves III, IV, V absent
OR prolonged I–V IPL > 4.6ms
(Scott-Brown's Otorhinolaryngology, 8th Ed.; Cummings Otolaryngology, 6th Ed.)
Sensitivity: ABR has ~90–98% sensitivity for detecting acoustic neuromas >1 cm.
Limitation: May miss small intracanalicular tumors (<1 cm); gadolinium-enhanced MRI is definitive.
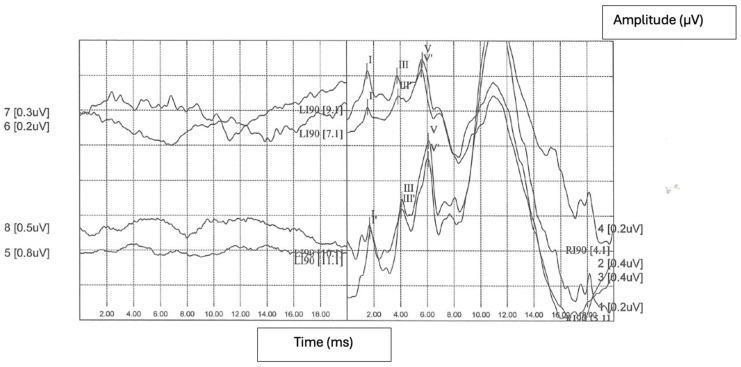
ABR Waveform Example from Literature:
9. Electrocochleography (ECochG)
- Measures: Cochlear microphonic (CM), Summating Potential (SP), and Action Potential (AP) of CN VIII
- In retrocochlear lesions: AP is absent or poorly formed; SP/AP ratio may be normal
- More useful to exclude cochlear pathology (endolymphatic hydrops) than to confirm retrocochlear
- Abnormally elevated SP/AP ratio (>0.4) = Menière's disease (cochlear), not retrocochlear
- Absence of AP with preserved CM = CN VIII lesion (retrocochlear)
10. Auditory Steady-State Response (ASSR)
- Frequency-specific electrophysiological threshold estimation
- Uses modulated tones (80–100 Hz carrier); responses detected by statistical analysis
- In retrocochlear: ASSR thresholds may be absent or highly elevated, frequency-dependent
- Useful as an objective audiogram, particularly when ABR is inconclusive
- Less specific for retrocochlear than ABR (Recent advances, Picton, 2011)
11. Middle Latency Response (MLR) and Cortical Auditory Evoked Potentials (CAEP)
- MLR assesses primary auditory cortex (waves Na, Pa, Nb at 15–50 ms)
- CAEP (P1, N1, P2, N2, P300) assesses higher cortical processing
- Used in central auditory processing disorders and cortical lesions
- Limited role in peripheral retrocochlear diagnosis
D. OTOACOUSTIC EMISSIONS (OAE) IN RETROCOCHLEAR DIAGNOSIS
Principle: OAEs (TEOAEs, DPOAEs) reflect outer hair cell (OHC) function — a purely cochlear measure.
Diagnostic utility in retrocochlear:
| Cochlear Lesion | Retrocochlear Lesion | |
|---|---|---|
| OAE | Absent (OHC damage) | Present (OHC intact) |
| ABR | Normal IPL or threshold shift | Abnormal IPL, absent waves |
- The combination of Present OAE + Absent/Abnormal ABR = "OAE/ABR Mismatch" is a hallmark of retrocochlear pathology (auditory neuropathy spectrum disorder included).
- (Scott-Brown, 8th Ed.; Cummings, 6th Ed.)
E. DIAGNOSTIC FLOWCHART FOR RETROCOCHLEAR PATHOLOGY
PATIENT PRESENTS WITH:
Unilateral SNHL / Asymmetric hearing loss / Poor speech discrimination /
Tinnitus / Vertigo
↓
┌─────────────────────┐
│ PURE TONE │
│ AUDIOMETRY (PTA) │
└──────────┬──────────┘
↓
Unilateral SNHL / Asymmetric PTA
↓
┌───────────────┼────────────────┐
▼ ▼ ▼
SPEECH TONE DECAY IMMITTANCE
AUDIOMETRY TEST AUDIOMETRY
(SDS/WRS) (Carhart) (SR + Decay)
│ │ │
SDS <50% >30 dB decay SR Decay >50%
PI-PB Rollover (positive) in 5 seconds
RI >0.45
│ │ │
└───────────────┼────────────────┘
↓
┌─────────────────────┐
│ BEKESY AUDIOMETRY │
│ (Type III/IV) │
└──────────┬──────────┘
↓
Retrocochlear suspected
↓
┌─────────────────────┐
│ OAE (TEOAE/DPOAE) │
│ Present → OHC OK │
└──────────┬──────────┘
↓
┌─────────────────────┐
│ ABR / BERA │
│ (GOLD STANDARD) │
└──────────┬──────────┘
↓
Prolonged I-V IPL / Absent Waves III-V
Inter-aural Wave V difference >0.4 ms
↓
┌─────────────────────┐
│ GADOLINIUM-ENHANCED │
│ MRI IAC/CPA │
│ (Definitive) │
└──────────┬──────────┘
↓
ACOUSTIC NEUROMA / CPA TUMOR
confirmed → Surgical/Radiological Rx
F. RECENT ADVANCES (Important for RGUHS)
1. High-Resolution MRI (Gd-DTPA Enhanced)
- Has largely replaced ABR as the definitive confirmatory test for acoustic neuromas.
- ABR sensitivity ~90–95% but MRI detects 100% of tumors, including intracanalicular ones <5 mm.
- ABR still cost-effective as a screening test before MRI.
2. Auditory Neuropathy Spectrum Disorder (ANSD)
- Characterized by: Present OAE + Absent/Abnormal ABR — the classic retrocochlear "mismatch."
- Lesion may be at inner hair cells, synapse, or CN VIII.
- First described by Starr et al. (1996).
- Management: Cochlear implants (CI) are often effective.
3. Chirp-Evoked ABR
- Uses frequency-swept chirp stimuli to compensate cochlear travel time, producing larger Wave V amplitude.
- Improves SNR and sensitivity of ABR in screening.
- Particularly useful in neonatal hearing screening programs.
4. Stacked ABR (Don et al., 2005)
- Summates energy from all frequency regions simultaneously.
- Increases sensitivity for small tumors (<1 cm) missed by conventional click-ABR.
- Reported sensitivity of 95% for small intracanalicular tumors.
5. ABR with Bone Conduction
- Useful when air-conduction thresholds are too high to generate clear waveforms.
6. VEMP (Vestibular Evoked Myogenic Potential)
- cVEMP (cervical): Saccular function via inferior vestibular nerve.
- oVEMP (ocular): Utricular function via superior vestibular nerve.
- In vestibular schwannoma: cVEMP is absent or elevated threshold on affected side.
- Increasingly used in the workup of CPA lesions (Recent literature, Murofushi et al.)
7. Auditory Change Complex (ACC)
- Can detect changes in ongoing sounds in real time.
- Future role in assessing central auditory processing in retrocochlear disorders.
G. COMPARATIVE SENSITIVITY/SPECIFICITY TABLE
| Test | Sensitivity for Retrocochlear | Specificity | Notes |
|---|---|---|---|
| Pure Tone Audiometry (asymmetric SNHL) | 75–80% | Low | Screening only |
| Speech Discrimination (SDS <50%) | 70–75% | Moderate | Low cost, quick |
| PI-PB Rollover (RI >0.45) | 65–70% | Moderate | Useful for VIII nerve |
| Tone Decay (>30 dB) | 55–70% | Moderate | Fatigue test |
| Bekesy (Type III/IV) | 55–60% | Moderate | Not widely used now |
| SISI (Low score) | 50–60% | Moderate | Supports cochlear/retro |
| Acoustic Reflex Decay | 65–85% | Moderate-High | Quick, objective |
| ABR / BERA (I–V IPL) | 90–98% | High | Gold standard electrophysiology |
| OAE + ABR Mismatch | High for ANSD | High | Diagnostic for ANSD |
| Gadolinium MRI | ~100% | Highest | Definitive imaging |
(Scott-Brown, 8th Ed.; Cummings, 6th Ed.; Dhingra; Hazarika)
H. SUMMARY: KEY RETROCOCHLEAR AUDIOLOGICAL FINGERPRINTS
┌──────────────────────────────────────────────────────────────┐
│ RETROCOCHLEAR AUDIOLOGICAL HALLMARKS │
├──────────────────────────────────────────────────────────────┤
│ • Unilateral SNHL with POOR speech discrimination │
│ • PI-PB Rollover Index > 0.45 │
│ • Tone Decay > 30 dB (Carhart's Test) │
│ • SISI Score 0–20% (LOW — no recruitment) │
│ • Bekesy Type III or IV │
│ • NO recruitment (ABLB negative) │
│ • Acoustic Reflex Decay (>50% in 5 seconds) │
│ • ABR: Prolonged I–V IPL (>4.6 ms) / Absent III–V │
│ • Inter-aural Wave V latency difference > 0.4 ms │
│ • OAE Present + ABR Absent = ANSD pattern │
└──────────────────────────────────────────────────────────────┘
Conclusion
The audiological evaluation of retrocochlear pathology requires a battery of tests, no single test being 100% sensitive. The traditional behavioral battery (tone decay, SISI, Bekesy, speech audiometry) provides a strong clinical suspicion. ABR/BERA remains the electrophysiological gold standard with sensitivity >90%, detecting delayed or absent neural transmission at the CN VIII and brainstem level. OAE/ABR dissociation is pathognomonic for auditory neuropathy spectrum disorder. In all suspected cases, gadolinium-enhanced MRI of the internal auditory canal (IAC) and cerebellopontine angle (CPA) is mandatory for definitive diagnosis, as up to 10% of acoustic neuromas may be missed even by ABR. Recent advances including stacked ABR, chirp-ABR, and VEMP have further refined the diagnostic capability for retrocochlear pathology.
References
- Harrison's Principles of Internal Medicine, 21st Ed. (pp. 1037–1041)
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery, 8th Ed., Vol. 2
- Cummings Otolaryngology, Head & Neck Surgery, 6th Ed.
- Dhingra PL — Diseases of Ear, Nose and Throat, 7th Ed.
- Hazarika P — Textbook of ENT, Head & Neck Surgery
- Stell & Maran's Head and Neck Surgery, 4th Ed.
- Zakir Hussain — ENT Textbook
- Jerger JF, Jerger S — Performance-Intensity Functions in Sensorineural Hearing Loss, JASA, 1971
- Don M, Masuda A, Nelson R, Brackmann D — Stacked ABR, Am J Otol, 2005
- Starr A et al. — Auditory Neuropathy, Brain, 1996
- Murofushi T et al. — VEMP in vestibular schwannoma, Acta Otolaryngol, 2012
This is a shared conversation. Sign in to Orris to start your own chat.