Explain extrahepatic biliary apparatus in full detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have rich, comprehensive content from multiple authoritative textbooks. Let me compile the full detailed response.
The Extrahepatic Biliary Apparatus
The extrahepatic biliary apparatus comprises all the bile-conducting structures that lie outside the liver parenchyma: the right and left hepatic ducts, the common hepatic duct, the gallbladder, the cystic duct, the common bile duct (choledochus), the ampulla of Vater, and the sphincter of Oddi. Together they form the conduit through which bile is transported from the liver to the duodenum, with the gallbladder serving as a storage and concentration reservoir.
1. Embryological Development
The entire system - liver, gallbladder, and biliary ducts - arises as a ventral endodermal outgrowth called the hepatic diverticulum, which buds from the distal foregut early in the 4th week of embryonic development. The Wnt/beta-catenin signaling pathway is central to this process, driving proliferation and differentiation of hepatoblasts into hepatocytes and cholangiocytes (epithelial cells of the biliary ducts). FGFs secreted by the developing heart induce formation of the hepatic diverticulum from bipotential endodermal cells.
The hepatic diverticulum grows into the septum transversum (a mass of splanchnic mesoderm separating the pericardial and peritoneal cavities) and rapidly divides into two parts:
- Larger cranial part - the primordium of the liver; proliferating endodermal cells form interlacing cords of hepatocytes and give rise to the intrahepatic biliary epithelium
- Smaller caudal part - the primordium of the gallbladder and cystic duct
The connection between the hepatic diverticulum and the foregut narrows to form the bile duct. Development of the intrahepatic biliary system depends on Notch signaling, while vascular endothelial growth factor Flk-1 signaling governs early morphogenesis of the hepatic sinusoids.
- The Developing Human: Clinically Oriented Embryology, p. 620-621
2. The Gallbladder
2a. Gross Anatomy and Position
The gallbladder is a pear-shaped, distensible sac that lies in a fossa on the visceral (inferior) surface of the right lobe of the liver, nestled between the right and quadrate lobes. In adults it is approximately 3 cm wide and 7 cm long, with a capacity of 30-50 mL.
It has three main parts:
- Fundus - the rounded blind end; may project from the inferior border of the liver at the level of the right lateral border of the rectus abdominis and the 9th costal cartilage
- Body - the main part lying against the transverse colon (anteriorly) and the superior part of the duodenum (posteriorly); perforation here can create cholecystoenteric fistulas
- Neck - the narrow tapered part that continues as the cystic duct; its mucosa forms the spiral valve of Heister, which regulates flow in and out of the gallbladder
Between the body and neck, the infundibulum is a region of tapering. An outpouching from the infundibulum's inferior surface is called Hartmann's pouch - a clinically important site where gallstones can become impacted, obstructing the cystic duct and causing acute cholecystitis. Extensive inflammation at Hartmann's pouch can compress the adjacent common hepatic duct, producing Mirizzi syndrome.
The gallbladder is covered anteriorly by an adventitia fused with the liver capsule (Glisson's capsule) and posteriorly/at the apex by visceral peritoneum.
2b. Microscopic Structure
The gallbladder wall consists of:
- Mucosa - a single layer of tall columnar epithelial cells over a lamina propria; numerous prominent folds (rugae) greatly expand the absorptive/secretory surface
- Lamina propria - contains connective tissue, blood vessels, and lymphatics
- Tunica muscularis - a thick layer with an interlocking array of longitudinal and spiral smooth muscle fibers; smooth muscle cells are largely circumferentially oriented
- Serosa (peritoneum) - covers the free surfaces
- Adventitia - covers the hepatic surface
Tubuloalveolar mucous glands are found particularly in the neck region, contributing to mucus secretion. Rokitansky-Aschoff sinuses are deep invaginations of the mucosa through the muscularis, important in cholecystitis pathology.
2c. Vascular Supply
Arterial supply: The cystic artery - typically a branch of the right hepatic artery - is the sole arterial supply. It divides near the gallbladder neck into:
- A superficial branch supplying the serosal surface
- A deep branch supplying the inner layers of the gallbladder wall
Because the cystic artery is an end artery with no collateral supply, the gallbladder is highly susceptible to ischemic injury and necrosis from inflammation or interruption of hepatic arterial flow. Variations in cystic artery origin and course are common and surgically important.
Venous drainage: The cystic vein drains into the portal vein, or occasionally directly into the hepatic sinusoids.
Lymphatics: Subserosal and submucosal lymphatics empty into a lymph node at the gallbladder neck (the cystic lymph node of Lund) and connect with lymphatics of Glisson's capsule.
2d. Nerve Supply
- Sympathetic: from the celiac axis, traveling with hepatic artery branches and portal vein. Visceral pain is referred via sympathetic fibers to the right subcostal, epigastric, and right scapular regions.
- Parasympathetic: from both vagus nerves, contributing to gallbladder motility regulation.
2e. Function
The gallbladder is a storage reservoir that allows bile acids to be delivered in high concentration and in a controlled manner to the duodenum for solubilization of dietary lipids. Between meals, the sphincter of Oddi is closed and bile accumulates in the gallbladder. It concentrates bile 5-10-fold by actively absorbing water and sodium. Upon eating (particularly fatty meals), cholecystokinin (CCK) is released from I-cells of the duodenum, causing gallbladder smooth muscle contraction and simultaneous sphincter of Oddi relaxation, expelling bile into the duodenum.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1168
- Gray's Anatomy for Students, p. 393
3. The Bile Ducts
3a. Hepatic Ducts
Bile is produced by hepatocytes and drains via the intrahepatic biliary canaliculi into progressively larger intrahepatic ducts, ultimately forming the right hepatic duct (draining the right lobe) and the left hepatic duct (draining the left lobe, caudate lobe, and quadrate lobe). These two ducts exit the liver at the porta hepatis and join to form the common hepatic duct.
3b. Common Hepatic Duct
The common hepatic duct descends in the free edge of the hepatoduodenal ligament (the right border of the lesser omentum) anterior to the portal vein and to the right of the hepatic artery proper. It is approximately 2-3 cm long before being joined by the cystic duct to form the common bile duct.
3c. Cystic Duct
The cystic duct is approximately 4 cm long and connects the gallbladder neck to the common hepatic duct. It maintains continuity with the gallbladder's columnar epithelium, lamina propria, muscularis, and serosa. The mucosa forms the spiral valve of Heister, which provides some resistance to backflow.
Cystic duct anatomy is highly variable:
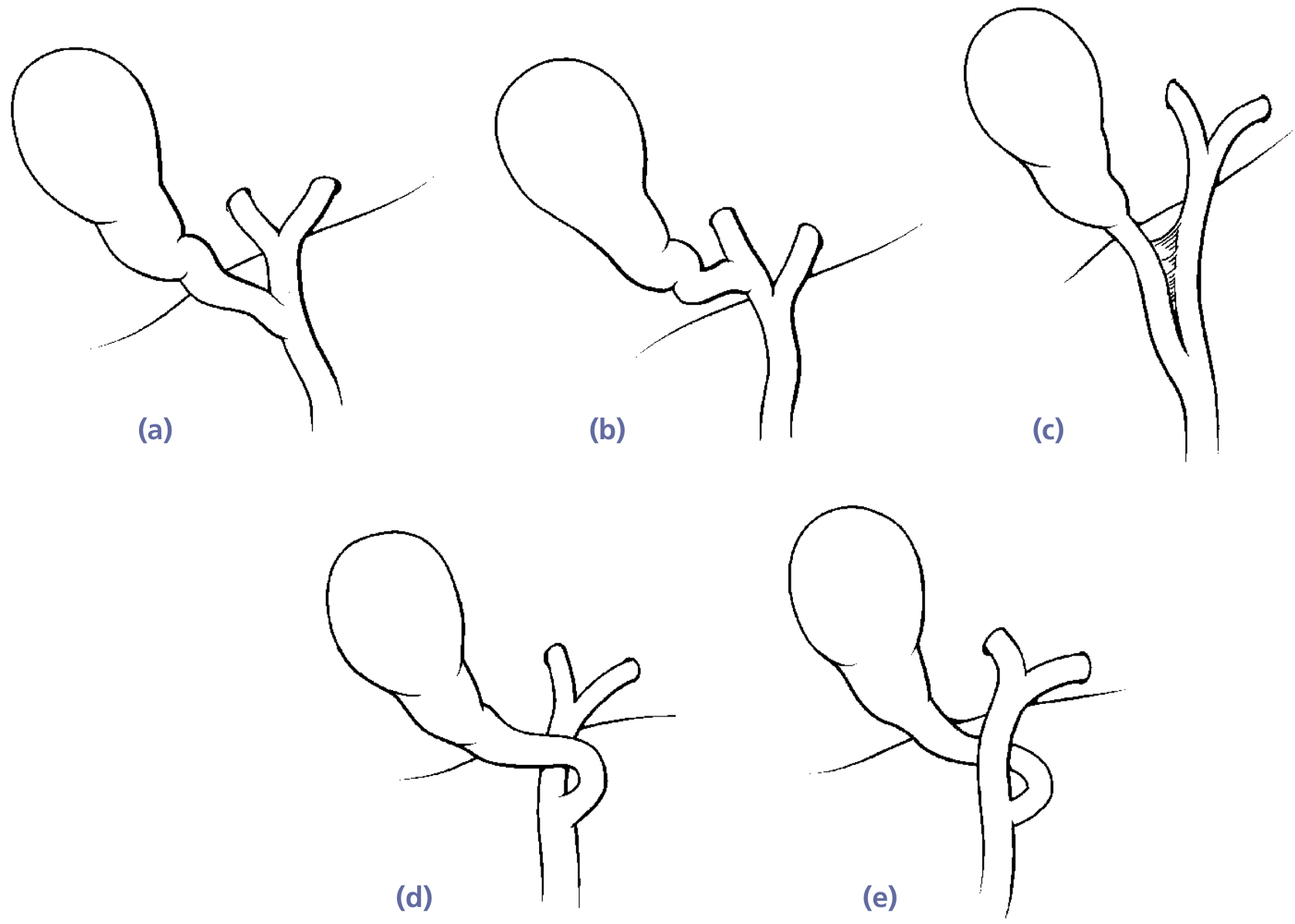
Fig: Variations in cystic duct anatomy - Yamada's Textbook of Gastroenterology
Common variations include: joining the common hepatic duct directly (most common), joining the right hepatic duct, a low junction, anterior spiral, or posterior spiral before union.
3d. Common Bile Duct (Ductus Choledochus)
The common bile duct (CBD) is formed by the union of the cystic duct and common hepatic duct. It is approximately 7.5 cm long with a mean diameter of ~6 mm (may dilate significantly with distal obstruction).
The CBD is divided into four anatomic segments:
| Segment | Location | Length | Key Relations |
|---|---|---|---|
| Supraduodenal | Right border of hepatoduodenal ligament | ~2.5 cm | Anterior to portal vein, right of hepatic artery; site of Pringle maneuver |
| Retroduodenal | Posterior to first part of duodenum | 2.5-4 cm | Moves right to left; lies just right of gastroduodenal artery; close to duodenal bulb (risk in posterior peptic ulcer) |
| Pancreatic | Lower border of duodenum to posteromedial wall of 2nd duodenum | Variable | May lie retropancreatic or within pancreatic head parenchyma; commonly obstructed by pancreatic head cancer |
| Intraduodenal | Traverses duodenal wall obliquely with pancreatic duct | ~2 cm | Travels with main pancreatic duct; narrows here (common site for stone impaction) |
The supraduodenal segment is critically important surgically - it lies within the hepatoduodenal ligament in a consistent relationship with the portal vein (posteriorly) and hepatic artery (medially). Compression of the hepatoduodenal ligament between the thumb and index finger passed through the epiploic foramen (foramen of Winslow) is the Pringle maneuver, used to control hepatic hemorrhage intraoperatively.
- Yamada's Textbook of Gastroenterology, p. 229
4. The Ampulla of Vater
The union of the common bile duct and the main pancreatic duct (of Wirsung) forms the hepatopancreatic ampulla (ampulla of Vater). This opens on the major duodenal papilla on the posteromedial wall of the second (descending) part of the duodenum, typically 7-10 cm from the pylorus. From the duodenal lumen, it appears as a small nipple-like protrusion marked by a longitudinal fold.
Key anatomical facts:
-
The ampulla is longer than 2 mm in 46% of cases (range 3-14 mm), less than 2 mm in 32%, and absent (separate ductal openings) in 29% of cases
-
When no junction between the two ducts exists, there is technically no true ampulla of Vater
-
The common bile duct narrows significantly as it passes through the duodenal wall; these narrowings are the most frequent sites for gallstones to lodge, causing biliary or pancreatic obstruction
-
Yamada's Textbook of Gastroenterology, p. 230
5. The Sphincter of Oddi
The intraduodenal segment of the CBD and the ampulla is surrounded by a sheath of smooth muscle collectively called the sphincter of Oddi. This is a unique group of muscle fibers arising from the bile duct wall that act independently of the surrounding duodenal musculature - verified by manometric studies.
Its components include:
- Sphincter choledochus (sphincter of Boyden) - circular muscle sheath investing the preampullary portion of the CBD
- Sphincter pancreaticus - a short sphincter around the distal pancreatic duct (when present); may intertwine with the sphincter choledochus in a figure-of-eight pattern
- Sphincter of the ampulla - smooth muscle surrounding the ampulla itself
Physiology:
- Resting pressure: approximately 13 mmHg above duodenal pressure
- Relaxation is triggered by CCK and facilitated by parasympathetic stimulation - allows bile flow into the duodenum after eating
- Increased tone is produced by sympathetic stimulation
- This sphincter is the primary regulator of bile flow
Clinical relevance: During endoscopic sphincterotomy (EST), the sphincter of Oddi is divided using electrocautery to relieve CBD obstruction from stones or stricture.
- Yamada's Textbook of Gastroenterology, p. 230
6. Blood Supply of the Extrahepatic Bile Ducts
The arterial supply to the extrahepatic bile ducts is segmental in nature, and this has major surgical implications:
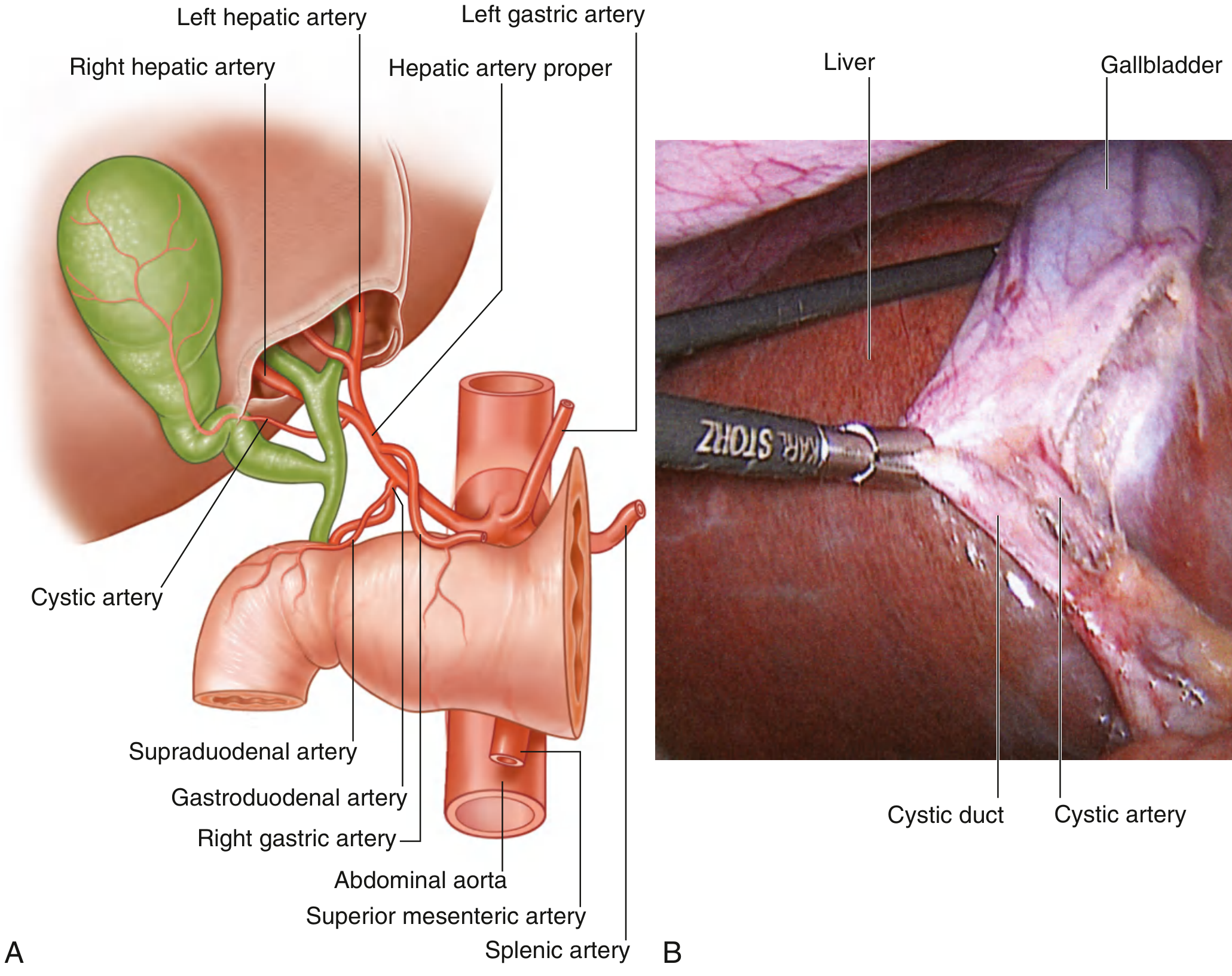
Fig: Arterial Supply to the Liver and Gallbladder (Gray's Anatomy for Students)
- Hepatic ducts and supraduodenal CBD: nourished by small branches from the cystic artery
- Retroduodenal CBD: supplied by the retroduodenal artery and the posterior superior pancreaticoduodenal artery
- Pancreatic segment: branches of the posterior superior pancreaticoduodenal artery
Because the blood supply is segmental and limited, extensive mobilization of the extrahepatic bile ducts during surgery can lead to ischemic injury, predisposing to postoperative biliary strictures. This principle underlies careful surgical technique in biliary reconstruction procedures.
- Yamada's Textbook of Gastroenterology, p. 230
7. Anatomical Relationships and the Hepatoduodenal Ligament
The extrahepatic bile ducts travel within the hepatoduodenal ligament (the free right edge of the lesser omentum, also called the portal triad). This ligament contains three critical structures in a consistent arrangement:
- Bile duct - rightmost, anterior
- Hepatic artery proper - leftmost, anterior
- Portal vein - posterior
This arrangement is the basis of the Pringle maneuver described above and is the key surgical landmark during cholecystectomy and biliary surgery.
8. Calot's Triangle (Cystohepatic Triangle)
Calot's triangle is a surgically critical anatomical space bounded by:
- Medially: common hepatic duct
- Laterally: cystic duct
- Superiorly: inferior surface of the liver
Within this triangle runs the cystic artery (typically a branch of the right hepatic artery). Safe identification and ligation of the cystic duct and cystic artery within Calot's triangle is the essential step in laparoscopic cholecystectomy. Failure to correctly identify these structures is the most common cause of bile duct injury during surgery.
9. Congenital Anomalies
Extrahepatic Ducts
- Accessory bile ducts: aberrant ducts draining liver segments directly into the gallbladder, cystic duct, or hepatic ducts; must be identified on cholangiography to avoid injury
- Biliary atresia: progressive obliterative cholangiopathy affecting extrahepatic ducts; the most common cause of neonatal cholestasis requiring surgery
- Complete bile duct duplication: rare; separate ducts drain right and left lobes
- Choledochal cysts: congenital dilations of the biliary tree (Types I-V by Todani classification)
Gallbladder
-
Agenesis (0.04-0.13% at autopsy): isolated or associated with other malformations
-
Double gallbladder (1-5 per 10,000): may share one cystic duct (Y-shaped) or each have a separate cystic duct
-
Phrygian cap deformity: folding of the fundus over the body
-
Intrahepatic gallbladder: embedded within liver parenchyma
-
Floating gallbladder: complete peritoneal covering with a mesentery, predisposing to torsion
-
Diverticula and septations: promote bile stasis and stone formation
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1169
10. Summary of Key Dimensions
| Structure | Length | Diameter |
|---|---|---|
| Common hepatic duct | ~2-3 cm | ~4-5 mm |
| Cystic duct | ~4 cm | ~3 mm |
| Common bile duct (total) | ~7.5 cm | ~6 mm |
| Supraduodenal CBD | ~2.5 cm | - |
| Retroduodenal CBD | 2.5-4 cm | - |
| Intraduodenal CBD | ~2 cm | - |
| Gallbladder | ~7 cm long, ~3 cm wide | - |
| Gallbladder capacity | - | 30-50 mL |
| Major papilla distance from pylorus | - | 7-10 cm |
Sources:
- Gray's Anatomy for Students, p. 393-394
- Yamada's Textbook of Gastroenterology 7th ed., p. 228-230
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 1168-1169
- The Developing Human: Clinically Oriented Embryology, p. 620-621
This is a shared conversation. Sign in to Orris to start your own chat.