Discoid meniscus
Reading File
search_medical_text
discoid meniscus anatomy classification diagnosis treatment
search_medical_image
discoid meniscus MRI arthroscopy
GradeResponse
GradeResponse
Discoid Meniscus
Definition & Anatomy
A discoid meniscus is a congenital anatomical variant in which the meniscus — almost exclusively the lateral meniscus — is abnormally large, thick, and disc-shaped rather than the normal crescent (semilunar) form. It covers most or all of the lateral tibial plateau instead of just the periphery.
Epidemiology
- Incidence: ~3–5% in Western populations; higher in Asian populations (up to 15%)
- Predominantly affects the lateral meniscus; discoid medial meniscus is rare
- Often bilateral (~20% of cases)
Classification (Watanabe)
| Type | Description |
|---|---|
| Type I — Complete | Disc covers entire tibial plateau; most common type |
| Type II — Incomplete | Partial coverage of tibial plateau |
| Type III — Wrisberg variant | Normal shape but lacks normal posterior meniscotibial (coronary) ligament attachment; highly unstable and prone to subluxation |
Pathophysiology
The abnormal shape leads to:
- Altered biomechanics and stress distribution across the knee
- Increased susceptibility to tears (horizontal cleavage tears most common)
- The Wrisberg variant lacks posterior ligamentous attachment, causing the meniscus to snap or displace during motion
Clinical Presentation
| Feature | Detail |
|---|---|
| Age | Children and adolescents most commonly; may present in adulthood |
| Classic sign | Painful clunk (audible/palpable snap) during knee extension — pathognomonic in children |
| Symptoms | Lateral knee pain, swelling, limited ROM, locking, giving way |
| Wrisberg variant | Dramatic snapping syndrome without a tear |
Bailey and Love's (p. 644) describes the hallmark as "a painful clunk on knee extension."
Diagnosis
X-ray findings (indirect signs):
- Widened lateral joint space
- Cupping/hypoplasia of lateral tibial plateau
- Elevated lateral fibular head
MRI (gold standard):
- Sagittal view: ≥3 consecutive 5 mm slices showing continuity of anterior and posterior horns (the "bow-tie sign")
- Coronal view: Abnormally wide transverse diameter of lateral meniscus extending beyond the tibial rim
- Identifies associated tears (horizontal cleavage tears most common)
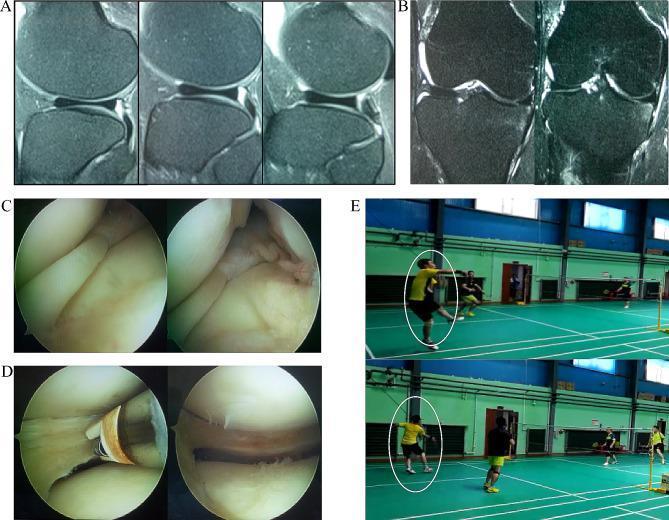
Panels A–B: Sagittal and coronal MRI showing continuous horns and widened lateral meniscus. Panel C: Preoperative arthroscopic view of incomplete discoid meniscus. Panel D: Post-saucerization with plasma knife. Panel E: Return to sports.
Arthroscopy: Definitive visualization; used therapeutically.
Management
Asymptomatic discoid meniscus — no intervention required; observation only.
Symptomatic (pain, mechanical symptoms, tear):
Arthroscopic saucerization (meniscoplasty) — primary treatment
- Resection and remodeling of the meniscus to a normal semilunar shape (~4 mm peripheral rim retained)
- Preferred over total meniscectomy to preserve meniscal function
Additional procedures:
- If a tear is present: repair if possible, especially in the vascularized peripheral zone
- Wrisberg variant: peripheral stabilization (repair of posterior attachments) in addition to saucerization
Total meniscectomy — historical, now avoided due to high rates of subsequent lateral compartment osteoarthritis.
Complications
- Untreated: progressive lateral compartment OA, especially with total meniscectomy
- Post-saucerization: residual or recurrent tears, lateral compartment OA over time, stiffness
- Re-tear of the residual meniscus is the most common post-operative issue
Prognosis
Outcomes after arthroscopic saucerization are generally good, with most patients (including children) returning to full activity and sports. Early intervention before articular cartilage damage occurs improves long-term outcomes. Total meniscectomy is associated with a significantly higher rate of late-onset lateral compartment arthrosis.
Posterior approach to elbow
search_medical_text
posterior approach to elbow surgical anatomy technique
search_medical_image
posterior approach elbow surgery anatomy
GradeResponse
GradeResponse
The text retrieval returned no results, so the answer is drawn from my own knowledge, supplemented by the retrieved image.
Posterior Approach to the Elbow
Indications
- Distal humerus fractures (intercondylar/transcondylar)
- Olecranon fractures and osteotomy
- Total elbow arthroplasty
- Excision of loose bodies
- Elbow ankylosis / contracture release
- Triceps repair
- Tumors of the distal humerus
Position
- Lateral decubitus (arm draped over a support) or prone position
- Tourniquet applied to the upper arm
- The elbow is flexed to ~90° throughout
Incision
A posterior midline longitudinal incision beginning ~8–10 cm proximal to the olecranon tip, curving gently laterally around the olecranon to avoid direct pressure on the bony prominence, then continuing distally along the subcutaneous border of the ulna.

Posterior midline incision curving laterally around the olecranon. Hash marks aid precise closure. Used here for olecranon osteotomy to expose the distal humeral articular surface.
Deep Dissection — Options for Exposure
Once skin and subcutaneous tissue are elevated as full-thickness flaps, three main strategies exist to access the elbow joint:
1. Triceps-Reflecting / Triceps-Splitting (Bryan–Morrey)
- The triceps aponeurosis is elevated off the olecranon as a continuous sleeve along with the periosteum, reflecting medially
- Restores continuity — no bone cut required
- Used in total elbow arthroplasty
- Risk: triceps avulsion / weakness
2. Olecranon Osteotomy (gold standard for articular exposure)
- A chevron (V-shaped) osteotomy is made at the bare area of the olecranon (~2 cm from the tip), with the apex pointing distally
- The proximal fragment with triceps attached is reflected proximally, providing wide exposure of the entire distal humeral articular surface
- Fixation at closure: tension band wiring or intramedullary screw + tension band
- Best visualization of the articular surface — preferred for complex distal humerus fractures
3. Paratricipital (Column) Approach
- The triceps is left attached; windows are developed medial and lateral to it
- Suitable for extra-articular distal humerus fractures (medial/lateral columns) without articular comminution
- Avoids risks of olecranon osteotomy or triceps detachment
Internervous Plane
The posterior approach does not use a true internervous plane — it relies on the midline avascular interval. However, the key nerve at risk is:
| Nerve | Location | Risk |
|---|---|---|
| Ulnar nerve | Medial epicondyle groove → cubital tunnel | Must be identified and protected throughout; consider anterior transposition |
| Radial nerve | Lateral, stays proximal | At risk if dissection extends proximally along lateral column |
| Posterior interosseous nerve | Not directly at risk in standard posterior approach | — |
The ulnar nerve must be formally identified and protected in every posterior elbow approach.
Deep Structures Exposed
- Posterior capsule of elbow joint
- Distal humerus: medial and lateral columns, olecranon fossa, trochlea, capitellum (via osteotomy)
- Proximal ulna and olecranon
- Radial head (with additional lateral mobilization)
Closure
- Repair olecranon osteotomy with tension band wiring ± intramedullary screw
- Reattach triceps sleeve if Bryan–Morrey was used
- Transpose ulnar nerve anteriorly if mobilized
- Subcutaneous and skin closure over a drain
Key Hazards & Pitfalls
| Hazard | Prevention |
|---|---|
| Ulnar nerve injury | Formal identification; protect throughout; consider transposition |
| Triceps dehiscence | Secure reattachment; protect in early rehabilitation |
| Olecranon osteotomy non-union | Rigid fixation, preserve blood supply to fragment |
| Skin necrosis over olecranon | Gentle lateral curve in incision; avoid direct pressure on scar |
| Elbow stiffness | Early mobilization protocol post-fixation |
This is a shared conversation. Sign in to Orris to start your own chat.