First seminar for department of Medicine, topic Evolving landscape for stroke management 2026,
stroke management 2024 2025 guidelines thrombolysis thrombectomy
acute ischemic stroke treatment tenecteplase extended window neuroprotection
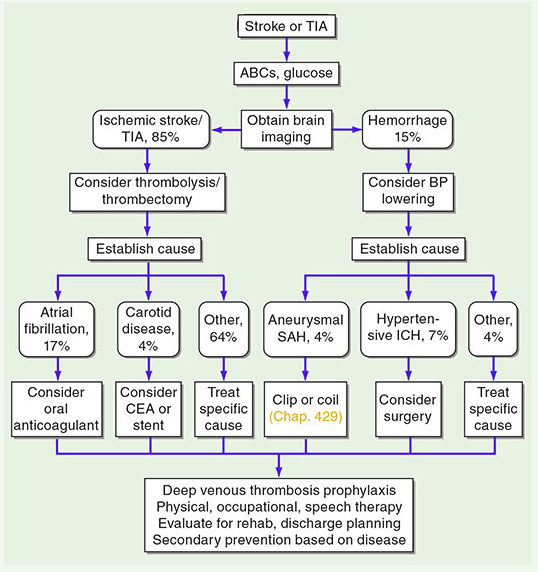
stroke management algorithm ischemic hemorrhagic pathway
Professional medical seminar announcement poster for "Evolving Landscape for Stroke Management 2026" - Department of Medicine First Seminar. Features brain/neurovascular imagery, modern medical design with bold title, seminar badge, and clean academic layout.
429 RESOURCE_EXHAUSTED. {'error': {'code': 429, 'message': 'Resource exhausted. Please try again later. Please refer to https://cloud.google.com/vertex-ai/generative-ai/docs/error-code-429 for more details.', 'status': 'RESOURCE_EXHAUSTED'}}
We encountered an error while processing your request. Please try again or reach out to us for help.
seminar for department of Medicine, topic Evolving landscape for stroke management 2026,
stroke management 2024 2025 guidelines thrombolysis thrombectomy acute ischemic stroke
stroke secondary prevention anticoagulation antiplatelet hemorrhagic stroke management
stroke management algorithm ischemic hemorrhagic pathway
Professional medical seminar announcement poster titled "Evolving Landscape for Stroke Management 2026" for the Department of Medicine. Include a brain with neurovascular/cerebral blood vessel illustration, modern clean academic design, "1st Seminar" badge, bold typography, and a medical conference aesthetic.
🧠 Evolving Landscape for Stroke Management 2026
Overview
SESSION OUTLINE
1. Stroke Epidemiology & Burden in 2026
- Global incidence: ~13.7 million strokes/year
- 85% ischemic | 15% hemorrhagic
- Rising stroke in young adults (<50 years)
- Low- and middle-income countries carry 70% of the burden
2. Acute Ischemic Stroke — Reperfusion Therapy Updates
A. Intravenous Thrombolysis
| Agent | Dose | Window | Notes |
|---|---|---|---|
| Alteplase | 0.9 mg/kg (max 90 mg) | ≤4.5 hrs | Still widely used; standard of care |
| Tenecteplase | 0.25 mg/kg (max 25 mg) | ≤4.5 hrs | Single IV bolus; non-inferior or superior recanalization; preferred in many updated protocols |
- Tenecteplase offers higher fibrin specificity, longer half-life, and ease of bolus administration — major advantage in prehospital and drip-and-ship models (Tenecteplase for Acute Ischaemic Stroke, p. 47)
- Wake-up stroke and unknown onset: MRI DWI-FLAIR mismatch guides eligibility
- Pre-treatment BP target: < 185/110 mmHg; maintain < 180/105 mmHg for 24 h post-thrombolysis (Management of Elevated Blood Pressure and Hypertension, p. 73)
B. Mechanical Thrombectomy (MT)
- Extended window: up to 24 hours in selected patients (DAWN & DEFUSE-3 criteria — penumbral imaging mismatch)
- Now the standard of care for large vessel occlusion (LVO)
- Combined IV thrombolysis + MT: ongoing debate ("drip and ship" vs. "mothership")
- Medium vessel occlusions (MeVO): emerging evidence supporting MT in M2/M3, basilar perforators
C. Imaging-Guided Selection (2026 Paradigm)
- CT perfusion / MRI perfusion: RAPID automated software widely deployed
- Collateral grading on CTA increasingly guides triage
- AI-driven LVO detection at CT triage (ambient intelligence in stroke workflows)
3. Blood Pressure Management in Acute Stroke
| Scenario | Target |
|---|---|
| Ischemic stroke, no reperfusion therapy | Permissive hypertension ≤220/120 mmHg in first 72 h; avoid aggressive lowering |
| Pre-thrombolysis | < 185/110 mmHg |
| Post-thrombolysis / post-MT (24 h) | < 180/105 mmHg |
| Hemorrhagic stroke (ICH) | Rapid lowering to < 140 mmHg systolic (INTERACT2, ATACH-2) |
- Intensive BP lowering in ischemic stroke post-thrombolysis is associated with increased mortality (OR 1.52, 95% CI 1.09–2.13) (Treatment of ICAD, p. 13)
- Induced hypertension for hemodynamic compromise (ICAD) remains a rescue-only strategy per ESO guidelines
4. Stroke Diagnostic Pathway
5. Hemorrhagic Stroke — Updates
Intracerebral Hemorrhage (ICH)
- Hematoma expansion (within 24 h) is the key modifiable target
- Tranexamic acid: not beneficial in unselected ICH (TICH-2)
- Factor Xa inhibitor reversal: Andexanet alfa — now guideline-recommended
- Dabigatran reversal: Idarucizumab
- Minimally invasive surgery (MIS) for ICH: MISTIE III, ENRICH trial — selected supratentorial ICH benefit
- Avoid steroids in ICH (harmful)
Subarachnoid Hemorrhage (SAH)
- Nimodipine 60 mg q4h for 21 days — vasospasm prevention
- Endovascular coiling preferred over surgical clipping for most aneurysms (ISAT)
- Surveillance imaging for unruptured aneurysms: updated risk stratification tools
6. Secondary Prevention — The 2026 Framework
Cardioembolic Stroke (Atrial Fibrillation)
- DOACs over warfarin for non-valvular AF (superior efficacy + safety)
- Apixaban non-inferior to LMWH in cancer-associated stroke
- Left Atrial Appendage Occlusion (LAAO / Watchman): for AF patients unable to tolerate anticoagulation
- Early anticoagulation debate: 1-3-6-12 rule (minor/moderate/severe/hemorrhagic transformation timing)
Non-Cardioembolic Stroke / TIA
- Dual antiplatelet therapy (aspirin + clopidogrel): 21 days then single agent (POINT, CHANCE trials)
- Ticagrelor + aspirin (THALES): modest benefit, higher bleeding
- Warfarin NOT superior to aspirin for non-cardioembolic stroke (Harrison's 21st Ed., p. 12165)
- Colchicine (CONVINCE trial): emerging role in inflammatory atherosclerotic stroke
Intracranial Atherosclerotic Disease (ICAD)
- Stenting (SAMMPRIS) showed higher risk than aggressive medical management
- Aggressive medical Rx: aspirin + clopidogrel 90 days, high-intensity statin, BP control
- Newer trials exploring drug-coated balloons in ICAD
Carotid Artery Disease
- CEA vs. CAS: CEA preferred for symptomatic stenosis >70% in good surgical candidates
- TCAR (Transcarotid Artery Revascularization): growing evidence
7. Emerging & Horizon Therapies in 2026
| Area | Development |
|---|---|
| Neuroprotection | No agent has yet translated to clinical benefit; NMDA antagonists, free radical scavengers under trial |
| Sonothrombolysis | Ultrasound-enhanced thrombolysis (CLOTBUST) — ongoing trials |
| Glymphatic system | Sleep-dependent brain waste clearance — implications for stroke recovery |
| Stem cell therapy | Phase II trials (SB623, MultiStem) — modest but promising functional recovery signals |
| AI & Predictive Analytics | AI-stroke code activation, outcome prediction, AF detection via wearables |
| Remote ischemic conditioning | RICAMIS trial positive in China — further validation needed |
8. Stroke Unit Care & Rehabilitation
- Stroke unit admission reduces mortality by 20–25% regardless of treatment
- Early mobilization (within 24 h — AVERT trial caveats: very early very intensive mobilization harmful)
- Dysphagia screening before any oral intake
- Post-stroke depression: screening with PHQ-9; SSRI (fluoxetine — FOCUS trial: no functional benefit but mood benefit)
- Constraint-induced movement therapy, robot-assisted rehabilitation — expanding evidence
9. Special Populations
- Cryptogenic stroke / ESUS: PFO closure in age <60 with high-risk features (RoPE score)
- Pregnancy-related stroke: heparin preferred; thrombolysis considered case-by-case
- Young stroke (<50 yrs): screen for thrombophilia, vasculitis, dissection, CADASIL, drug-related causes
- Posterior circulation stroke: high early recurrence risk after TIA — urgent workup essential
10. Key Takeaways
- Tenecteplase is replacing alteplase as the preferred IV thrombolytic in many centers
- Thrombectomy window has expanded to 24 hours with appropriate imaging selection
- BP management is nuanced — permissive in early ischemic stroke, aggressive in ICH
- DOACs are the cornerstone of AF-related stroke prevention
- Dual antiplatelet for 21 days after minor stroke/TIA is evidence-based
- Stroke unit care and multidisciplinary rehabilitation remain irreplaceable pillars
- AI, wearables, and minimally invasive neurosurgery are reshaping the 2026 landscape
References: Harrison's Principles of Internal Medicine, 21st Ed. | AHA/ASA Stroke Guidelines 2024 | ESO Guidelines 2023 | Tenecteplase for Acute Ischaemic Stroke (Orris Medical Database) | Management of Elevated BP and Hypertension (Orris Medical Database) | Treatment of Intracranial Atherosclerotic Disease (Orris Medical Database)