common cardiac diseases with ecg changes
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full, detailed answer.
Common Cardiac Diseases and Their ECG Changes
Here is a systematic, textbook-based reference covering the major cardiac conditions and their characteristic ECG findings.
1. Acute Myocardial Infarction (AMI) / Ischemic Heart Disease
This is the most ECG-rich area in cardiology. The ECG changes depend on the territory, depth (transmural vs. subendocardial), and phase of ischemia.
Pathophysiology of ECG Changes
Severe acute ischemia lowers the resting membrane potential and shortens action potential duration, creating a voltage gradient between normal and ischemic zones. These "currents of injury" appear as ST-segment deviations on the surface ECG.
(Harrison's Principles of Internal Medicine 22E)
ST-Elevation MI (STEMI)
| Lead Group | Territory | Culprit Vessel |
|---|---|---|
| V1-V4 | Anterior wall | LAD (proximal) |
| I, aVL, V5-V6 | Lateral wall | LCx or diagonal |
| II, III, aVF | Inferior wall | RCA (most common) or LCx |
| V1-V3 (reciprocal ST depression) | Posterior wall | RCA/LCx |
| V3R-V4R (right-sided leads) | Right ventricle | Proximal RCA |
Sequence of ECG changes (STEMI evolution):
- Hyperacute T waves - tall, broad, positive T waves (earliest sign, minutes)
- ST elevation - upward convex or straight, in the territory of ischemia
- Q wave formation - pathological Q waves (>1mm wide, >1/4 R height) indicating necrosis
- T wave inversion - develops over hours to days
- ST normalization, Q waves may persist
From Harrison's: "When ischemic ST elevations occur as the earliest sign of acute infarction, they typically are followed within hours to days by evolving T-wave inversions and often by Q waves in the same lead distribution."
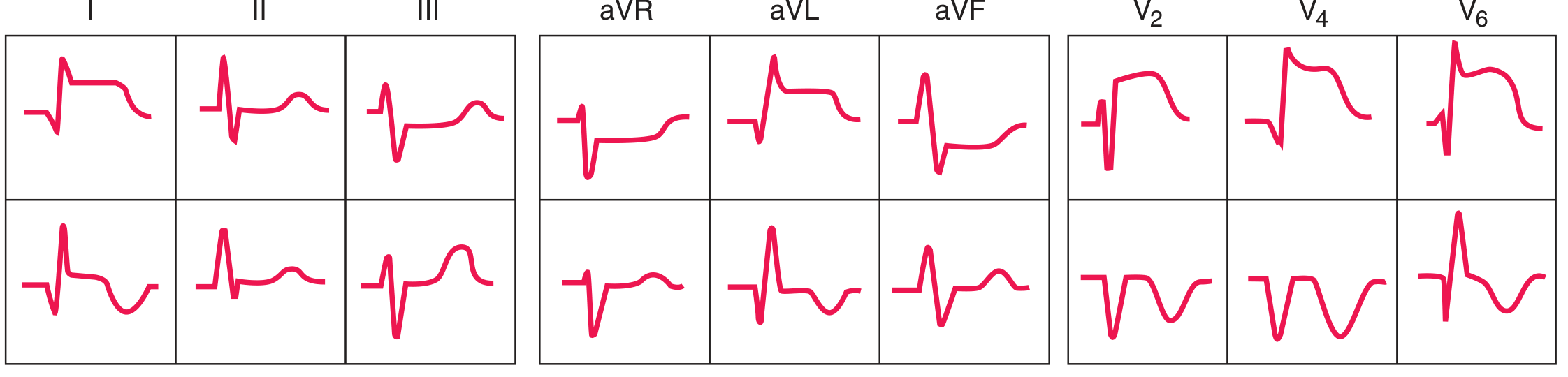
The image below from Harrison's shows the classic anterior (top row) and inferior (bottom row) STEMI ECG sequences:
Special STEMI Localization Points
- Inferior STEMI (RCA): ST elevation greater in III than II, plus ST depression in I and aVL (reciprocal); if ST elevation also in V1, suspect right ventricular involvement - confirm with right-sided leads (V3R-V4R)
- Posterior STEMI: Tall R wave + ST depression in V1-V3 (mirror image); use posterior leads V7-V9
- Wellens' Syndrome: Deeply inverted or biphasic T waves in V2-V3 (sometimes V1-V4) when pain-free - indicates critical LAD stenosis, high risk for anterior STEMI. Present in ~75% as deep inversion, ~25% as biphasic pattern (Tintinalli's Emergency Medicine)
NSTEMI / Unstable Angina
- ST depression (horizontal or downsloping) - more common in subendocardial ischemia
- T-wave inversion without Q waves
- Normal ECG - does not exclude NSTEMI (biomarkers required)
- When subendocardial ischemia is diffuse: ST depression in multiple leads + ST elevation in aVR
2. Acute Pericarditis
Four-stage ECG evolution (Braunwald's Heart Disease):
| Stage | ECG Changes | Timing |
|---|---|---|
| Stage I | Diffuse ST elevation (saddle-shaped/concave-up) + PR depression in I, II, III, aVF, V3-V6; reciprocal ST depression + PR elevation in aVR, V1 | Early hours to days |
| Stage II | ST returns to baseline, PR normalizes | Days |
| Stage III | T-wave inversions develop (diffuse) | Weeks |
| Stage IV | ECG normalizes | Weeks to months |
Key differentiating features from STEMI:
- ST elevation is diffuse (not territory-specific)
- ST elevation is concave upward ("saddle-shaped"), not convex
- PR depression is highly characteristic (absent in STEMI)
- No reciprocal ST changes (unlike STEMI, except aVR/V1)
- No Q waves
- Spodick's sign: downward-sloping TP segment (sensitive but not specific)
(Symptom to Diagnosis; Fuster and Hurst's The Heart; Rosen's Emergency Medicine)
3. Heart Failure / Cardiomyopathy
Dilated Cardiomyopathy (DCM)
- Sinus tachycardia (compensatory)
- Left bundle branch block (LBBB) - common; broad QRS >120ms, notched R in I/V5-V6, QS in V1
- Left ventricular hypertrophy (LVH) - Sokolow-Lyon criteria: S in V1 + R in V5/V6 >35mm; or Cornell criteria
- Atrial fibrillation (from atrial dilation)
- Non-specific ST-T changes
- Poor R-wave progression in precordial leads
- Interventricular conduction delay
Hypertrophic Cardiomyopathy (HCM)
- LVH pattern (often striking voltage)
- Deep, narrow Q waves (septal hypertrophy) - especially in inferolateral leads (II, III, aVF, V5-V6) - "dagger-like" Q waves
- T-wave inversions (especially lateral leads)
- ST depression in lateral leads
- Left axis deviation
- Apical HCM variant: giant negative T waves in precordial leads V4-V6 (Yamaguchi pattern)
- ECG Q waves or inferolateral changes help differentiate from athlete's heart (Goldman-Cecil Medicine)
Restrictive Cardiomyopathy / Cardiac Amyloidosis
- Low voltage (small QRS complexes despite thick walls on echo - a striking mismatch)
- Pseudo-infarction Q waves (without actual infarction)
- Conduction abnormalities (AV block, bundle branch blocks)
- Atrial fibrillation
4. Conduction System Diseases / Arrhythmias
Bundle Branch Blocks
| Finding | LBBB | RBBB |
|---|---|---|
| QRS duration | ≥120ms | ≥120ms |
| V1 | QS or rS pattern | RSR' ("rabbit ears") |
| V5-V6, I, aVL | Broad monophasic R (notched) | Wide S wave |
| Axis | Normal or left | Normal or right |
- Left anterior fascicular block (LAFB): Left axis deviation < -45°, no other cause
- Left posterior fascicular block (LPFB): Right axis deviation >+110°, rare as isolated finding (Harrison's Principles of Internal Medicine)
Wolff-Parkinson-White (WPW) Syndrome
- Short PR interval (<120ms)
- Delta wave (slurred upstroke of QRS)
- Wide QRS (>120ms, due to preexcitation)
- Can mimic LBBB, RBBB, or MI (pseudo-infarct Q waves)
- Associated with SVT (AVRT) or AF with rapid ventricular response
Atrial Fibrillation
- Irregularly irregular RR intervals
- Absence of distinct P waves (replaced by fibrillatory f waves, best seen in V1)
- Ventricular rate varies
Atrial Flutter
- Sawtooth flutter waves (F waves) at ~300 bpm, best in II, III, aVF
- Ventricular rate typically 150 bpm (2:1 block)
Complete AV Block (3rd Degree)
- P waves and QRS complexes completely dissociated
- P rate faster than QRS rate
- Narrow escape (junctional) or wide escape (ventricular) QRS
5. Infective Endocarditis (IE)
- Usually nonspecific findings
- New AV block (1st, 2nd, or 3rd degree) or bundle branch block - signals perivalvular extension, especially from aortic valve IE extending to the AV node/His bundle (10-20% incidence with perivalvular extension)
- New conduction abnormality is a multivariate predictor of death in IE (Braunwald's Heart Disease)
6. Pulmonary Embolism (PE)
- Sinus tachycardia (most common finding)
- S1Q3T3 pattern: S wave in lead I, Q wave and T-wave inversion in lead III (classic but insensitive)
- Right heart strain: Right axis deviation, right bundle branch block (complete or incomplete), ST depression + T-wave inversions in V1-V4
- T-wave inversions in V1-V4 (right ventricular strain)
- New atrial fibrillation
- Sinus tachycardia is the most sensitive but least specific finding
7. Electrolyte Abnormalities (Cardiac-relevant)
Hyperkalemia
Progressive ECG changes (Miller's Anesthesia):
- Peaked, symmetric ("tent-shaped") T waves (earliest)
- Prolonged PR interval and widened QRS
- Loss of P waves
- Sine wave pattern (severe, precedes cardiac arrest)
- Ventricular fibrillation / asystole
Hypokalemia
- Flattened or inverted T waves
- Prominent U waves (best seen V2-V3)
- QU prolongation (can trigger TdP)
- ST depression
Hypercalcemia
- Short QT interval (shortened ST segment)
Hypocalcemia
- Prolonged QT interval (prolonged ST segment specifically)
8. Long QT Syndrome (LQTS) & Brugada Syndrome
Long QT Syndrome
- Prolonged QTc (>440ms men, >460ms women)
- Risk of polymorphic VT (Torsades de Pointes - TdP)
- TdP on ECG: twisting of QRS axis around baseline, "spindle-fuseau" pattern
Brugada Syndrome
- Coved ST elevation (≥2mm) in V1-V2, followed by negative T wave (Type 1 - diagnostic)
- Right bundle branch block morphology
- Associated with sudden cardiac death, especially at rest/sleep
9. Aortic Stenosis / Valvular Disease
- LVH (pressure overload - concentric hypertrophy)
- Left axis deviation
- ST-T strain pattern ("LV strain"): ST depression and T-wave inversion in lateral leads (I, aVL, V5-V6) - the "strain pattern" suggests significant hypertrophy
10. Mitral Valve Prolapse (MVP)
- May be normal or show non-specific changes
- T-wave inversions in inferior (II, III, aVF) and lateral leads
- ST-segment changes that can mimic ischemia
- Associated with ventricular ectopy (PVCs) (Grainger & Allison's Diagnostic Radiology)
ECG Localization Quick Reference
| Leads with Changes | Cardiac Territory | Typical Vessel |
|---|---|---|
| V1-V4 | Anterior | LAD |
| I, aVL, V5-V6 | Lateral | LCx / Diagonal |
| II, III, aVF | Inferior | RCA (dominant) |
| V1-V3 (reciprocal depression) | Posterior | RCA / LCx |
| V3R-V4R | Right ventricle | Proximal RCA |
| Diffuse (all leads) | Pericarditis | - |
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Braunwald's Heart Disease | Goldman-Cecil Medicine | Tintinalli's Emergency Medicine | Rosen's Emergency Medicine | Fuster and Hurst's The Heart 15E | Miller's Anesthesia | Symptom to Diagnosis
Create a quick ECG interpretation reference poster or PDF
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.