Anti viral drugs from KD Tripathi
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have everything needed to deliver a comprehensive, well-structured answer on antiviral drugs as covered by KD Tripathi (using Katzung as the equivalent standard pharmacology reference in the library). Here is the full response:
Antiviral Drugs - KD Tripathi Style
Note: KD Tripathi's Essentials of Medical Pharmacology is not directly in this library, but the content below is sourced from Katzung's Basic and Clinical Pharmacology (16th ed.) - the international equivalent - which covers exactly the same syllabus as Tripathi. The classification and drug details align closely with Tripathi's presentation.
Key Concept
Antiviral drugs are virustatic - they are active only against replicating virus; they do not eliminate latent virus. They must either block viral entry/exit from the cell or be active inside the host cell (since viruses are obligate intracellular parasites).
Sites of Antiviral Drug Action
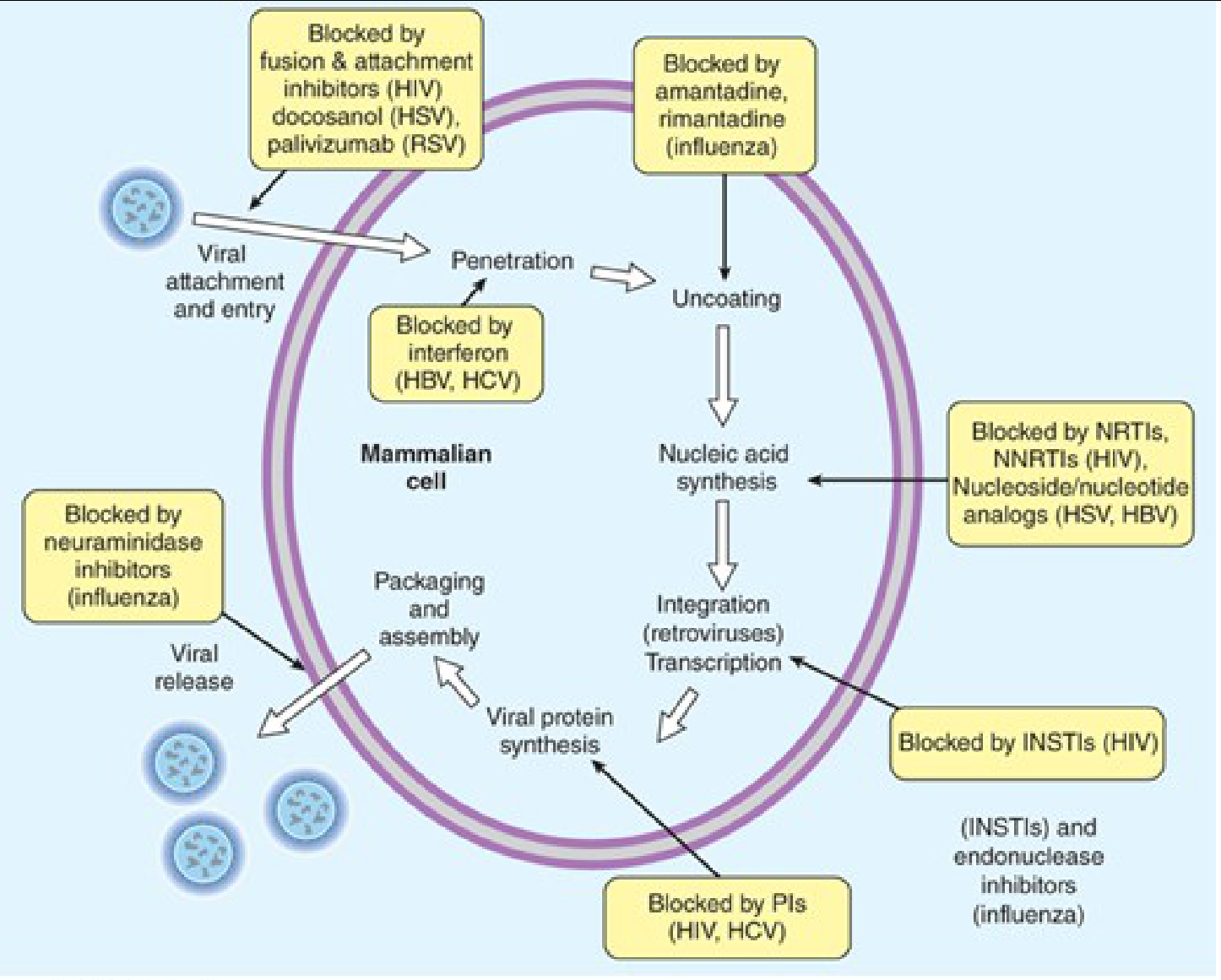
| Step in Viral Lifecycle | Drugs That Block It |
|---|---|
| Attachment & Entry | Fusion inhibitors (enfuvirtide), Attachment inhibitors (fostemsavir), Palivizumab (RSV), Docosanol (HSV) |
| Uncoating | Amantadine, Rimantadine (Influenza) |
| Nucleic Acid Synthesis | NRTIs, NNRTIs (HIV); Nucleoside analogs - acyclovir, ganciclovir (HSV/CMV); Sofosbuvir (HCV); Tenofovir (HBV) |
| Integration | INSTIs (raltegravir, dolutegravir, bictegravir) |
| Viral Protein Synthesis | Interferons (HBV, HCV) |
| Assembly & Maturation | Protease inhibitors - PIs (HIV, HCV) |
| Viral Release | Neuraminidase inhibitors - oseltamivir, zanamivir (Influenza) |
Classification of Antiviral Drugs
1. Anti-Herpesvirus Drugs (HSV, VZV, CMV)
Acyclovir (Prototype)
- Mechanism: Acyclovir is a guanosine analog. It is selectively phosphorylated by viral thymidine kinase (TK) to acyclovir monophosphate, then by host cell kinases to the triphosphate form, which inhibits viral DNA polymerase and causes chain termination.
- Selectivity: ~3,000 times more active against viral DNA polymerase than host polymerase
- Spectrum: HSV-1, HSV-2, VZV, EBV (less active against CMV)
- Uses: Genital herpes, herpes labialis, herpes encephalitis (IV: 10 mg/kg q8h x 14-21 days), neonatal HSV (IV: 20 mg/kg q8h), VZV (shingles), chickenpox
- ADRs: Crystalluria/nephrotoxicity (IV - maintain hydration), neurotoxicity at high doses; generally well-tolerated orally
- Resistance: Mutation in viral TK (most common) or DNA polymerase
Valacyclovir
- L-valyl ester prodrug of acyclovir; converted to acyclovir after intestinal/hepatic metabolism
- Higher oral bioavailability (~55% vs 15-30% for acyclovir)
- Dosed less frequently (bid vs 5 times/day)
Famciclovir
- Prodrug of penciclovir; similar mechanism to acyclovir
- Longer intracellular half-life than acyclovir
Ganciclovir
- Guanosine analog; phosphorylated by CMV UL97 protein kinase
- Spectrum: CMV (cytomegalovirus) - the key drug here
- Uses: CMV retinitis, CMV colitis, CMV pneumonitis in immunocompromised
- ADRs: Myelosuppression (neutropenia, thrombocytopenia) - major dose-limiting toxicity; also nephrotoxic, teratogenic, gonadotoxic
- Valganciclovir: Oral prodrug with improved bioavailability
Foscarnet
- Pyrophosphate analog; directly inhibits viral DNA polymerase WITHOUT requiring phosphorylation by viral kinase
- Use: CMV retinitis (alternative to ganciclovir); acyclovir-resistant HSV/VZV
- ADRs: Nephrotoxicity (major), electrolyte imbalances (hypocalcemia, hypomagnesemia, hypophosphatemia), seizures, penile ulceration
Cidofovir
- Nucleotide analog (already phosphorylated once); active against CMV, HSV, adenovirus, poxvirus
- ADR: Severe nephrotoxicity (requires co-administration with probenecid + IV saline prehydration)
2. Anti-Influenza Drugs
Neuraminidase Inhibitors (Preferred)
| Drug | Route | Notes |
|---|---|---|
| Oseltamivir (Tamiflu) | Oral | Most widely used; given within 48h of symptom onset; prophylaxis dose: 75 mg OD |
| Zanamivir (Relenza) | Inhaled | Bronchospasm risk in asthmatic patients |
| Peramivir | IV | Single-dose; for hospitalized patients |
| Baloxavir marboxil | Oral | Newer; inhibits cap-dependent endonuclease (PA subunit of polymerase complex); single oral dose |
- Mechanism of neuraminidase inhibitors: Neuraminidase cleaves sialic acid residues, allowing newly formed virions to be released from the host cell surface. Inhibiting it traps virions on the cell surface, limiting spread.
- Active against: Influenza A and B
Adamantanes (Older, largely obsolete due to resistance)
| Drug | Notes |
|---|---|
| Amantadine | Blocks M2 ion channel of Influenza A; prevents viral uncoating; also used in Parkinsonism |
| Rimantadine | Same mechanism; fewer CNS side effects; NOT effective against Influenza B |
- ADRs of Amantadine: Insomnia, nervousness, lightheadedness, anticholinergic effects; teratogenic
- Note: >90% of circulating Influenza A strains are now resistant to adamantanes; no longer recommended for routine influenza treatment
3. Antiretroviral Drugs (HIV)
HIV treatment requires combination antiretroviral therapy (cART) - typically 2 NRTIs + 1 INSTI (preferred) or PI or NNRTI.
a) NRTIs - Nucleoside/Nucleotide Reverse Transcriptase Inhibitors
Mechanism: Converted intracellularly to triphosphate forms that competitively inhibit HIV reverse transcriptase and cause chain termination (lack 3'-OH group).
| Drug | Notes |
|---|---|
| Zidovudine (AZT, ZDV) | First antiretroviral; thymidine analog; ADRs: macrocytic anemia, neutropenia, myopathy, lactic acidosis with hepatic steatosis |
| Lamivudine (3TC) | Well-tolerated; also active against HBV |
| Emtricitabine (FTC) | Similar to 3TC; also active against HBV; long intracellular half-life (39h) |
| Tenofovir Disoproxil Fumarate (TDF) | Nucleotide analog; also used in HBV; ADRs: nephrotoxicity, Fanconi syndrome, decreased bone density |
| Tenofovir Alafenamide (TAF) | Newer prodrug; less nephrotoxic and bone toxicity than TDF |
| Abacavir (ABC) | ADR: Hypersensitivity reaction (HLA-B*5701 allele carriers); screen with HLA testing before use |
| Stavudine (d4T) | Largely phased out; peripheral neuropathy, lipoatrophy |
| Didanosine (ddI) | Pancreatitis, peripheral neuropathy |
- Class ADRs: Lactic acidosis with hepatic steatosis (mitochondrial toxicity)
b) NNRTIs - Non-Nucleoside Reverse Transcriptase Inhibitors
Mechanism: Bind directly to the hydrophobic pocket near the catalytic site of reverse transcriptase (non-competitive inhibition); do NOT require phosphorylation.
| Drug | Notes |
|---|---|
| Efavirenz | Standard of care; CNS side effects (dizziness, nightmares, depression); teratogenic (avoid in 1st trimester); CYP3A4 inducer AND inhibitor |
| Nevirapine | Hepatotoxicity (especially in women with CD4 >250); severe rash/Stevens-Johnson syndrome |
| Rilpivirine | Take with meal (absorption increased 40%); avoid PPIs; lower CNS effects |
| Doravirine | Newer; minimal CNS effects; no food restriction |
| Etravirine | Active against K103N/Y181C mutants; diarylpyrimidine |
- Class ADRs: Rash, hepatotoxicity; high genetic barrier to resistance with etravirine; low barrier with efavirenz/nevirapine (single mutation - K103N)
c) Protease Inhibitors (PIs)
Mechanism: Inhibit HIV aspartyl protease, preventing cleavage of the Gag-Pol polyprotein, resulting in immature, non-infectious viral particles.
| Drug | Notes |
|---|---|
| Atazanavir (ATV) | Once-daily; indirect hyperbilirubinemia (jaundice, no liver damage) |
| Darunavir (DRV) | High genetic barrier to resistance; preferred PI; requires ritonavir/cobicistat boosting |
| Lopinavir/Ritonavir (LPV/r) | Fixed-dose combination; ritonavir used as pharmacokinetic booster |
| Ritonavir | Now used only as a booster (inhibits CYP3A4); at full dose causes GI intolerance, lipid abnormalities |
- Class ADRs: Metabolic syndrome (hyperlipidemia, insulin resistance, lipodystrophy), GI intolerance, nephrolithiasis (atazanavir)
- Boosting: Ritonavir or cobicistat inhibit CYP3A4, increasing plasma levels of co-administered PIs
d) INSTIs - Integrase Strand Transfer Inhibitors (Preferred first-line)
Mechanism: Inhibit HIV integrase, preventing insertion of viral DNA into host genome.
| Drug | Notes |
|---|---|
| Raltegravir | First INSTI; twice daily; generally well-tolerated; CK elevation, myopathy |
| Elvitegravir | Requires cobicistat boosting; once daily |
| Dolutegravir | High genetic barrier; once daily; preferred in guidelines; neural tube defect risk in early pregnancy |
| Bictegravir | Latest; highest genetic barrier; only available as fixed-dose combination (Biktarvy = BIC/TAF/FTC) |
| Cabotegravir | Long-acting injectable (monthly or every 2 months) with rilpivirine |
e) Entry/Fusion Inhibitors
| Drug | Class | Mechanism | Notes |
|---|---|---|---|
| Enfuvirtide (T-20) | Fusion inhibitor | Binds gp41, prevents membrane fusion | SC injection only; injection site reactions; reserved for resistant HIV |
| Maraviroc | CCR5 antagonist | Blocks CCR5 co-receptor on host cell | Only for CCR5-tropic virus (tropism testing required before use); hepatotoxicity |
| Fostemsavir | Attachment inhibitor | Binds gp120, blocks CD4 binding | For multi-drug resistant HIV |
| Ibalizumab | CD4 post-attachment inhibitor | Blocks post-attachment step | IV infusion; multi-drug resistant HIV |
| Lenacapavir | Capsid inhibitor | Blocks capsid protein function at multiple stages | Long-acting (6-monthly SC); most potent and newest class |
4. Anti-Hepatitis Drugs
HBV (Hepatitis B)
- Interferon alfa-2b / Peginterferon alfa-2a: Immunomodulatory; 48-week course; 30-40% response; ADRs: flu-like syndrome, depression, cytopenias, thyroid dysfunction
- Tenofovir (TDF/TAF): Preferred; potent; low resistance
- Entecavir: Guanosine analog; highly potent; low resistance; avoid in lamivudine-resistant HBV
- Lamivudine: High resistance rates (70% at 5 years); now second-line
- Adefovir: Nephrotoxic at higher doses; used for lamivudine-resistant HBV
- Telbivudine: Moderate potency; peripheral neuropathy; higher resistance
HCV (Hepatitis C) - Direct Acting Antivirals (DAAs)
Three major targets:
NS3/4A Protease Inhibitors ("-previr" drugs):
- Glecaprevir, Grazoprevir, Voxilaprevir - pangenotypic; potent; avoid in severe hepatic impairment
NS5B Polymerase Inhibitors ("-buvir" drugs):
- Sofosbuvir - nucleotide analog; pangenotypic; backbone of most regimens; renal dose adjustment required; avoid with amiodarone
NS5A Inhibitors ("-asvir" drugs):
- Ledipasvir, Velpatasvir, Pibrentasvir, Elbasvir - reduce viral replication and assembly; NS5A resistance variants (RAVs) can limit efficacy
Common DAA Combinations:
| Regimen | Genotype Coverage | Duration |
|---|---|---|
| Sofosbuvir/Ledipasvir | GT 1, 4, 5, 6 | 8-12 weeks |
| Glecaprevir/Pibrentasvir (Mavyret) | Pangenotypic | 8-16 weeks |
| Sofosbuvir/Velpatasvir (Epclusa) | Pangenotypic | 12 weeks |
| Elbasvir/Grazoprevir (Zepatier) | GT 1, 4 | 12-16 weeks |
5. Anti-RSV Drugs
| Drug | Type | Notes |
|---|---|---|
| Palivizumab | Monoclonal antibody (anti-F protein) | Monthly prophylaxis for high-risk infants (premature, congenital heart disease) |
| Nirsevimab | Long-acting monoclonal antibody | Single-dose prophylaxis; newer; longer duration |
| Ribavirin | Nucleoside analog (guanosine) | Inhaled for RSV bronchiolitis/pneumonia in infants; also used in HCV (with interferon); teratogenic; hemolytic anemia |
6. Drugs for COVID-19
| Drug | Class | Notes |
|---|---|---|
| Nirmatrelvir/Ritonavir (Paxlovid) | 3CL protease inhibitor + booster | Oral; mild-moderate COVID in high-risk patients; within 5 days of symptoms |
| Remdesivir | Nucleoside analog (RNA-dependent RNA polymerase inhibitor) | IV; hospitalized patients; 5-day course |
| Molnupiravir | Nucleoside analog | Oral; increases viral mutation rate (mutagenesis); teratogenic risk |
| Baricitinib | JAK inhibitor (immunomodulator) | Hospitalized on O2/ventilation; JAK1/JAK2 inhibitor |
| Tocilizumab | IL-6 receptor antagonist | Hospitalized on corticosteroids + O2/ventilation; single IV dose |
7. Miscellaneous Antivirals
| Drug | Use | Mechanism/Notes |
|---|---|---|
| Ribavirin | RSV, HCV (with interferon), Lassa fever, Crimean-Congo HF | Guanosine analog; broad-spectrum; teratogenic; hemolytic anemia |
| Interferons (alfa, beta) | HBV, HCV, hairy cell leukemia, MS (beta) | Induces antiviral state; immunomodulatory; ADRs: flu-like, cytopenias, depression, thyroid dysfunction |
| Imiquimod | Genital warts (HPV) | Topical immune response modifier; induces interferon and cytokines |
| Cidofovir | CMV retinitis, adenovirus, poxvirus | Must use with probenecid to prevent nephrotoxicity |
| Trifluridine (Trifluorothymidine) | Herpes keratitis (topical) | DNA synthesis inhibitor; too toxic for systemic use |
| Docosanol | Herpes labialis (topical) | Inhibits viral attachment/entry |
Quick Mnemonics (Tripathi Style)
- NRTIs remember: "AZT eats the LATTES" → Zidovudine, emtricitabine, lamivudine, abacavir, tenofovir, stavudine
- Neuraminidase inhibitors end in "-navir" group → Oseltamivir, Zanamivir, Peramivir
- Protease inhibitors end in "-navir" → Ritonavir, Atazanavir, Darunavir, Lopinavir
- INSTIs end in "-gravir" → Raltegravir, Dolutegravir, Bictegravir, Elvitegravir, Cabotegravir
- NS5B (HCV) drugs end in "-buvir" → Sofosbuvir
- NS3/4A (HCV) drugs end in "-previr" → Glecaprevir, Grazoprevir
- NS5A (HCV) drugs end in "-asvir" → Ledipasvir, Velpatasvir, Pibrentasvir
- Katzung's Basic and Clinical Pharmacology 16th Ed., Chapter 49 (Antiviral Agents)
This is a shared conversation. Sign in to Orris to start your own chat.