Pre-op management and post-op management of a patient with a bronchial asthma, posted for laparoscopic cholecystectomy. Give me an exam ready answer for MD anesthesia exam with the possible table questions.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have excellent textbook content from Morgan & Mikhail, Miller's Anesthesia, and Barash. Let me compile the comprehensive exam-ready answer.
Bronchial Asthma in a Patient Posted for Laparoscopic Cholecystectomy
Pre-operative and Post-operative Anesthetic Management
(MD Anesthesia Exam-Ready Answer)
PATHOPHYSIOLOGIC CONTEXT
Asthma is a chronic airway disease characterized by reversible airflow obstruction, airway inflammation, and bronchial hyperreactivity. Perioperatively:
- Bronchospasm develops in approximately 9% of asthmatics in the perioperative period
- 25% of asthmatics may present with wheezing after induction of anesthesia
- The most critical time is during instrumentation of the airway
- Even 50% of patients with non-allergic bronchospasm have no prior history of asthma (ASA Closed Claims Project)
Added complexity of laparoscopic cholecystectomy:
| Pneumoperitoneum Effect | Mechanism | Relevance to Asthmatic |
|---|---|---|
| ↑ Peak airway pressure | Cephalad diaphragm displacement, ↓ FRC | Worsens airway obstruction |
| ↓ Respiratory compliance | Abdominal insufflation | May precipitate air trapping |
| Hypercapnia/respiratory acidosis | CO2 absorption across peritoneum | Masks hypoventilation |
| V/Q mismatch | Atelectasis, ↓ FRC | Hypoxemia |
| Trendelenburg position | Reduces FRC further | Worsens work of breathing |
PRE-OPERATIVE MANAGEMENT
1. History and Severity Assessment
Establish asthma severity and control:
| Parameter | What to Assess |
|---|---|
| Symptom control | Dyspnea, cough, wheeze at rest vs. exertion |
| Exacerbations | Frequency, severity, hospitalizations in last 6-12 months |
| ICU admissions / prior intubation | Identifies high-risk patients |
| Current medications | SABA, LABA, ICS dose, oral steroids, leukotriene antagonists |
| Triggers | Allergens, ASA/NSAIDs (important - will be needed post-op!), cold air, exercise |
| Last exacerbation | Should be at least 4-6 weeks symptom-free before elective surgery |
Decision rule: Elective surgery should be postponed 4-6 weeks if the patient has active bronchospasm or a recent exacerbation. Well-controlled asthma is NOT a risk factor for perioperative complications - Morgan & Mikhail, 7e.
2. Physical Examination
- Auscultate chest for wheeze, rhonchi, prolonged expiration
- Assess for features of severe disease: pulsus paradoxus, accessory muscle use, central cyanosis
- Document baseline SpO2 on room air
3. Investigations
| Investigation | Purpose |
|---|---|
| Spirometry (FEV1, FEV1/FVC, FEF 25-75%, PEFR) | Assess severity; reversibility post-bronchodilator |
| Chest X-ray | Air trapping (flattened diaphragm, hyperlucent fields, small heart) |
| ABG (if FEV1 <50% or active distress) | Hypercapnia = severe disease, impending respiratory failure |
| CBC | Eosinophilia, polycythemia if chronic hypoxia |
| Serum electrolytes | Hypokalemia with beta-agonist use |
| ECG | Right heart strain in severe chronic asthma |
Note: Routine spirometry outside cardiothoracic procedures has limited value in predicting postoperative pulmonary complications; its role is in confirming and quantifying obstructive disease - Berek & Novak / Morgan & Mikhail.
4. Pre-operative Optimization
Pharmacological optimization:
| Step | Intervention |
|---|---|
| Continue all bronchodilators up to the day of surgery | Do NOT withhold SABA/LABA/ICS |
| Add short-acting beta-2 agonist (salbutamol 2 puffs) | Give 15-20 min before induction |
| For suboptimal control: oral prednisolone 40 mg/day x 5 days pre-op | Combined ICS + SABA x 5 days pre-op reduces perioperative bronchospasm risk |
| Ipratropium bromide (if copious secretions) | Add-on; do not use as monotherapy |
| Avoid H2 blockers (ranitidine, famotidine) for premedication | H2 blockade leaves H1 unopposed - worsens bronchoconstriction if histamine release occurs |
Steroid supplementation (stress dose):
| Indication | Regimen |
|---|---|
| Oral steroids >5 mg prednisolone/day or within 6 months | Hydrocortisone 100 mg IV at induction + q8h for 24h, then taper to baseline in 1-2 days |
| Large dose ICS | Consider perioperative stress dosing |
Non-pharmacological:
- Smoking cessation (minimum 8 weeks for pulmonary benefit; even 12-24 hours reduces CO, improves oxygenation)
- Chest physiotherapy if secretions are significant
- Patient education and anxiety reduction (emotional stress triggers bronchospasm)
Premedication:
- Anxiolytic: benzodiazepine (midazolam 1-2 mg IV) - reduces sympathetic stress without respiratory depression at usual doses
- Anti-sialagogue: glycopyrrolate preferred over atropine (less tachycardia); use if ketamine is induction agent
- Avoid morphine/meperidine for premedication (histamine releasers)
- Aspiration prophylaxis: pantoprazole 40 mg oral the night before + morning of surgery (note: avoid H2 blockers)
INTRA-OPERATIVE MANAGEMENT
5. Anesthetic Technique
Regional vs. General Anesthesia:
- Laparoscopic cholecystectomy requires general anesthesia with endotracheal intubation (pneumoperitoneum, Trendelenburg, muscle relaxation required)
- Spinal/epidural not suitable for laparoscopic surgery; also, high thoracic epidural (T1-T4 block) could block sympathetic bronchodilator tone and worsen bronchoconstriction
6. Induction
Preferred induction agents:
| Agent | Reason for Preference |
|---|---|
| Propofol (1.5-2 mg/kg) | Bronchodilation, attenuates airway reflexes, smooth induction - FIRST CHOICE |
| Ketamine (1-2 mg/kg) | Bronchodilation (sympathomimetic + direct smooth muscle relaxation); preferred if hemodynamically unstable |
| Etomidate (0.3 mg/kg) | Cardiovascularly neutral; no bronchodilation, but acceptable |
| AVOID: Thiopentone | Precipitates histamine release, bronchospasm |
Airway management:
- LMA (supraglottic airway) is preferred IF adequate muscle relaxation and low risk of aspiration are ensured - avoids tracheal stimulation
- If ETT required: use smaller size (7.0 in women, 7.5 in men), use armored tube for long laparoscopy
- Pretreat before intubation: IV/intratracheal lidocaine 1-2 mg/kg or additional induction agent bolus or volatile agent at 2-3 MAC for 5 min to blunt reflex bronchospasm
- Ensure deep anesthesia before intubating - light anesthesia is the most dangerous trigger
Muscle relaxants:
| Agent | Recommendation |
|---|---|
| Vecuronium / Rocuronium | Preferred - no histamine release |
| Cisatracurium | Acceptable (no histamine at standard doses unlike atracurium) |
| Avoid Atracurium | Histamine release - precipitates bronchospasm |
| Succinylcholine | Generally safe; rarely causes histamine release; acceptable for RSI |
7. Maintenance
| Component | Choice | Rationale |
|---|---|---|
| Volatile agent | Sevoflurane (preferred) | Most potent bronchodilator among volatiles; smooth; no airway irritation |
| Isoflurane (alternative) | Bronchodilates; more pungent - avoid for inhalation induction | |
| Avoid Desflurane | Potent airway irritant; increases airway resistance - especially in asthmatics and children | |
| TIVA | Propofol infusion | Excellent if volatiles not suitable; reduced airway irritability |
| Opioids | Fentanyl, remifentanil | Minimal histamine release; avoid morphine/meperidine |
| N2O | Avoid (or minimize) | Increases bowel gas, distension; contraindicated in laparoscopy |
Ventilation strategy:
- Use warmed, humidified gases
- Tidal volume: 6 mL/kg (low tidal volume)
- Prolonged expiratory time (I:E ratio 1:3 or 1:4) to prevent air trapping and auto-PEEP
- Moderate PEEP (3-5 cmH2O) to maintain FRC, counter pneumoperitoneum-induced atelectasis
- Monitor capnography - upward sloping (shark fin) end-tidal CO2 trace = expiratory obstruction
- Keep insufflation pressure <12-15 mmHg - higher pressures worsen airway pressures and AKI risk
- Accept permissive hypercapnia if no cardiovascular or neurologic contraindication
- Adjust ventilator rate to maintain ETCO2 35-45 mmHg (CO2 absorption from pneumoperitoneum will increase ETCO2; increase minute ventilation by ~15-25%)
Monitoring:
- Standard ASA + invasive arterial line if severe disease
- SpO2, ETCO2, airway pressure (peak and plateau), tidal volume
- Neuromuscular blockade monitor (TOF)
- Temperature (use warm humidified gases)
8. Intraoperative Bronchospasm - Recognition and Treatment
Recognition:
| Sign | Mechanism |
|---|---|
| Bilateral wheeze | Airflow obstruction |
| ↑ Peak airway pressure (plateau unchanged) | Increased airway resistance |
| ↓ Exhaled tidal volumes | Air trapping |
| Slowly rising ETCO2 / shark-fin capnograph | Expiratory obstruction |
| SpO2 desaturation | V/Q mismatch |
Differential diagnosis of intraoperative bronchospasm (exam favourite!):
| Cause | Clue |
|---|---|
| True bronchospasm | Bilateral wheeze, ↑ peak, plateau unchanged |
| Endobronchial intubation | Unilateral breath sounds, tube too deep |
| Kinked/obstructed ETT | No air movement, obstruction at tube |
| Overinflated ETT cuff | Tube position issue |
| Pulmonary edema | Pink frothy sputum, bilateral crepitations |
| Pulmonary embolism | Sudden ETCO2 drop, hemodynamic instability |
| Pneumothorax | Unilateral, tracheal deviation, ↑ airway pressure |
| Patient straining/light anesthesia | Clinical context |
Treatment of intraoperative bronchospasm (stepwise):
| Step | Intervention |
|---|---|
| 1. Eliminate triggers | Deepen anesthesia (↑ volatile concentration), check tube position, remove offending drug |
| 2. 100% FiO2 | Immediately |
| 3. Inhaled SABA | Salbutamol (albuterol) 2-4 puffs via ETT adaptor - FIRST-LINE |
| 4. IV Hydrocortisone | 100-200 mg IV (especially steroid-dependent patients) |
| 5. IV/Inhaled Ipratropium | Anticholinergic bronchodilation |
| 6. IV Magnesium sulfate | 2 g over 20 min - smooth muscle relaxation |
| 7. IV Epinephrine | 0.1-0.3 mcg/kg/min infusion - for refractory bronchospasm; life-saving |
| 8. IV Aminophylline | 5 mg/kg loading over 30 min (narrow therapeutic window; use if others fail) |
| 9. IV Ketamine | Bolus 0.5-1 mg/kg if depth of anesthesia inadequate |
9. Reversal and Extubation
| Approach | Rationale |
|---|---|
| Deep extubation (preferred) | Remove ETT before return of airway reflexes; eliminates extubation-triggered bronchospasm |
| Ensure no wheeze before extubation | Must be bronchospasm-free at end of surgery |
| Neuromuscular reversal: Sugammadex (preferred) | Avoids neostigmine-induced ↑ACh + anticholinergic side effects; no bronchospasm trigger |
| If neostigmine must be used | Always preceded by appropriate atropine or glycopyrrolate |
| IV lidocaine 1-2 mg/kg at extubation | Blunts airway reflexes |
| Avoid suctioning at light planes | Major bronchospasm trigger |
POST-OPERATIVE MANAGEMENT
10. Immediate Post-operative (PACU)
| Priority | Action |
|---|---|
| Supplemental O2 | Continue 28-40% O2 via facemask for 4-6 hours post-op |
| Continue bronchodilators | Resume all pre-op inhalers immediately post-op |
| SpO2 monitoring | Target SpO2 >95%; continuous for 30-60 min |
| Chest auscultation | Rule out wheeze, atelectasis, pneumothorax |
| Avoid cold dry oxygen | Use humidified, warmed oxygen |
| CPAP/BiPAP | Consider if SpO2 <92% or significant atelectasis |
| Adequate analgesia | Critical - see below |
11. Post-operative Analgesia (Critical Consideration)
Why it matters: Inadequate analgesia → splinting → atelectasis → V/Q mismatch → hypoxemia. But over-sedation → respiratory depression.
Analgesic strategy (Multimodal, Opioid-sparing):
| Analgesic | Dose | Note |
|---|---|---|
| Paracetamol (acetaminophen) | 1 g IV/oral q6h | Safe, no bronchospasm |
| Ketorolac (NSAID) | USE WITH CAUTION | Aspirin-sensitive asthma: absolute contraindication to all NSAIDs (5-10% of asthmatics have NSAID-exacerbated respiratory disease) |
| Celecoxib (COX-2 selective) | Generally safer alternative to non-selective NSAIDs | Less risk in non-ASA-sensitive asthmatics |
| IV Fentanyl (titrated) | Small boluses in PACU | Minimal histamine; preferred opioid |
| TAP block (Transversus Abdominis Plane) | Reduces opioid requirement | Excellent for laparoscopic ports |
| Port-site local anesthetic infiltration | Bupivacaine 0.25% | Simple, effective |
| Shoulder tip pain | Due to diaphragmatic irritation from residual CO2 | Nurse in semi-recumbent; diclofenac if not aspirin-sensitive |
EXAM TABLE: NSAIDs and Asthma
| Drug | Safety in Asthma |
|---|---|
| Non-selective NSAIDs (ketorolac, diclofenac, ibuprofen) | Contraindicated in aspirin-sensitive asthma (Samter's triad: asthma + nasal polyps + NSAID sensitivity) |
| COX-2 inhibitors (celecoxib) | Generally safe in non-NSAID-sensitive asthmatics |
| Paracetamol | Safe (very rarely implicated) |
| Tramadol | Avoid - histamine release |
| Morphine | Avoid if possible - histamine release |
12. Post-operative Respiratory Physiotherapy
- Deep breathing exercises
- Incentive spirometry (target >70% of predicted)
- Early ambulation (within 4-6 hours for laparoscopic cholecystectomy - day surgery)
- Positioning: semi-recumbent (30-45°) to maximize FRC and diaphragmatic excursion
- Humidification
- Continue nebulized salbutamol q4-6h for 24 hours in moderate-severe asthmatic
13. Steroid Management Post-operative
- If stress doses given intra-op: taper hydrocortisone to baseline regimen within 24-48 hours
- Monitor blood glucose (steroids cause hyperglycemia)
- Do not abruptly stop long-term oral steroids
14. Discharge Criteria (Day Surgery)
- No wheeze on auscultation
- SpO2 ≥95% on room air
- Pain controlled on oral analgesics
- Tolerating oral fluids
- Passed urine
- Stable vital signs
- Written asthma action plan if exacerbation occurs at home
- Early follow-up (24-48 hours post-discharge)
EXAM-READY TABLES
Table 1: Drugs to Avoid vs. Prefer in Asthmatic Patients
| Category | Prefer | Avoid |
|---|---|---|
| Induction agents | Propofol, Ketamine, Etomidate | Thiopentone |
| Muscle relaxants | Vecuronium, Rocuronium, Cisatracurium, Succinylcholine | Atracurium, Mivacurium |
| Volatile agents | Sevoflurane, Isoflurane | Desflurane |
| Opioids | Fentanyl, Remifentanil, Alfentanil | Morphine, Meperidine (pethidine), Tramadol |
| Reversal | Sugammadex | Neostigmine alone (use with anticholinergic if must use) |
| Antibiotics | Cephalosporins | Penicillins/cephalosporins if known allergic |
| NSAIDs post-op | Celecoxib (COX-2), Paracetamol | Non-selective NSAIDs in NSAID-sensitive asthma |
| Premedication | Midazolam, Glycopyrrolate | H2 blockers (ranitidine, famotidine) |
| Colloids/plasma expanders | Albumin, crystalloids | Dextran, Gelatin (histamine release) |
Table 2: Severity-Based Pre-op Management Strategy
| Asthma Severity | Pre-op Strategy |
|---|---|
| Mild intermittent (well-controlled, PEFR >80%) | Salbutamol inhaler 15-20 min pre-op; proceed with surgery |
| Mild persistent | Add ICS optimization; SABA pre-op; proceed if well-controlled |
| Moderate persistent | ICS + LABA; consider 5-day oral prednisolone pre-op; confirm reversibility on spirometry |
| Severe/poorly controlled | Postpone 4-6 weeks; aggressive optimization; IV steroids + nebulization; PFT; may need ICU post-op |
| Acute exacerbation (emergency surgery) | Nebulized salbutamol + IV hydrocortisone + O2 for few hours then proceed; ABG monitoring |
Table 3: Physiological Effects of CO2 Pneumoperitoneum Relevant to Asthma
| System | Effect | Clinical Implication for Asthmatic |
|---|---|---|
| Respiratory | ↓ FRC, ↓ compliance, ↑ airway pressure | Worsens airflow obstruction |
| Gas exchange | CO2 absorption → hypercapnia, acidosis | Masked by air trapping |
| Airway | ↑ Peak inspiratory pressure | Difficult to distinguish from bronchospasm |
| Cardiovascular | ↑ PVR, ↑ catecholamines | May worsen bronchospasm |
| Position (Trendelenburg) | Cephalad visceral displacement, ↓ FRC | Compounded atelectasis |
Table 4: Ventilation Strategy Comparison (Normal vs. Asthmatic with Pneumoperitoneum)
| Parameter | Normal Patient | Asthmatic + Laparoscopy |
|---|---|---|
| Tidal volume | 7-8 mL/kg | 6 mL/kg (low VT) |
| I:E ratio | 1:2 | 1:3 to 1:4 (prolonged expiration) |
| PEEP | 5 cmH2O | 3-5 cmH2O (titrate; auto-PEEP risk) |
| FiO2 | 0.4-0.5 | 0.5-1.0 titrate to SpO2 |
| ETCO2 target | 35-40 mmHg | Accept 45-55 (permissive hypercapnia if no ICP ↑) |
| Respiratory rate | 12-14/min | Increase rate to compensate for CO2 absorption |
Table 5: Intraoperative Bronchospasm - Step-wise Treatment
| Step | Drug | Dose | Notes |
|---|---|---|---|
| 1 | Deepen anesthesia | ↑ Sevoflurane | Remove trigger |
| 2 | Salbutamol MDI via ETT | 4-6 puffs | First-line bronchodilator |
| 3 | IV Hydrocortisone | 200 mg IV | Steroid-dependent patients |
| 4 | IV MgSO4 | 2 g over 20 min | Smooth muscle relaxation |
| 5 | IV/inhaled Ipratropium | 0.5 mg neb | Anticholinergic bronchodilator |
| 6 | IV Ketamine | 0.5-1 mg/kg | Bronchodilation + deepens anesthesia |
| 7 | IV Epinephrine | 0.1 mcg/kg/min | Refractory bronchospasm |
| 8 | IV Aminophylline | 5 mg/kg over 30 min | Last resort (narrow TI) |
Table 6: Extubation Strategy in Asthmatic
| Approach | Indication | Technique |
|---|---|---|
| Deep extubation (preferred) | Mild-moderate asthma, easy airway, no aspiration risk | Remove ETT at plane 2-3 anesthesia |
| Awake extubation | Difficult airway, full stomach, high aspiration risk | Pretreat with IV lidocaine 1.5 mg/kg; IV salbutamol 250 mcg if wheeze present |
| LMA substitution | If ETT used throughout, swap to LMA at end, then awake removal | Reduces extubation bronchospasm |
Table 7: Post-operative Complications to Watch for
| Complication | Cause | Management |
|---|---|---|
| Bronchospasm | Residual airway irritability, secretions | Nebulized salbutamol; O2; IV hydrocortisone |
| Atelectasis | ↓ FRC post-laparoscopy, pain splinting | Incentive spirometry, physiotherapy, analgesia |
| Pneumonia | Aspiration, atelectasis, secretion retention | Antibiotics, physiotherapy |
| Hypoxemia | V/Q mismatch, atelectasis | O2 supplementation, CPAP if severe |
| Shoulder tip pain | Residual CO2 under diaphragm | Semi-recumbent positioning, paracetamol, COX-2 inhibitor |
| Subcutaneous emphysema | CO2 extravasation | Usually self-limiting; monitor airway |
| Post-op nausea/vomiting | Laparoscopy, opioids | Ondansetron, dexamethasone (also helps bronchodilation) |
SPECIAL EXAM POINTS
-
H2 blockers are CONTRAINDICATED as premedication in asthmatics - they leave H1 stimulation unopposed when histamine is released, worsening bronchoconstriction. Use PPIs instead.
-
Aspirin-sensitive asthma (Samter's Triad) = asthma + nasal polyps + NSAID intolerance. These patients must receive paracetamol and COX-2 inhibitors only for post-op analgesia.
-
Desflurane must be avoided in all asthmatics - it is a potent airway irritant and increases airway resistance.
-
Sevoflurane is the volatile of choice - most potent bronchodilator, least pungent, smooth inhalation.
-
Deep extubation vs. awake extubation - always justify your choice based on airway difficulty and aspiration risk.
-
Permissive hypercapnia is acceptable in asthmatics under laparoscopy - do not aggressively hyperventilate (worsens auto-PEEP, air trapping, barotrauma).
-
Sugammadex is preferred over neostigmine for reversal - avoids the cholinergic surge and its bronchospastic potential.
-
CO2 pneumoperitoneum will increase ETCO2 by ~15-25%; increase minute ventilation pre-emptively before insufflation.
-
The capnograph "shark fin" or sawtooth pattern (slow upslope on expiration) is the earliest sensitive sign of airway obstruction intraoperatively.
-
Dexamethasone (given for PONV prophylaxis in laparoscopy) has the added benefit of reducing airway inflammation - use 8 mg IV at induction.
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e | Miller's Anesthesia, 10e | Barash's Clinical Anesthesia, 9e | Berek & Novak's Gynecology (Perioperative Asthma Management)
Pre-op management and post-op management of a patient with a bronchial asthma, posted for laparoscopic cholecystectomy. Give me an exam ready answer for MD anesthesia exam with the possible table questions.
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Here is a complete, structured MD Anesthesia exam-ready answer.
Bronchial Asthma in a Patient Posted for Laparoscopic Cholecystectomy
Perioperative Anesthetic Management - MD Anesthesia Exam
INTRODUCTION / CLINICAL SIGNIFICANCE
Bronchial asthma is a chronic inflammatory airway disorder characterized by reversible airflow obstruction, bronchial hyperreactivity, and mucus hypersecretion. Its perioperative significance:
- Bronchospasm occurs in ~9% of asthmatics in the perioperative period
- 25% of asthmatics may wheeze after induction of anesthesia
- 1.7% sustain a poor respiratory outcome
- ASA Closed Claims Project: 40 bronchospasm-related claims - 88% resulted in brain damage or death; only half had pre-existing asthma/COPD
- Key principle: Well-controlled asthma is NOT a risk factor for perioperative complications. Poorly controlled asthma is. (Morgan & Mikhail, 7e)
Laparoscopic cholecystectomy adds unique physiologic challenges through CO2 pneumoperitoneum and Trendelenburg positioning, which directly worsen respiratory mechanics in an asthmatic patient.
PART I: PRE-OPERATIVE MANAGEMENT
A. Pre-anaesthetic Assessment
1. History - Severity Stratification
| Parameter | What to Assess |
|---|---|
| Symptom burden | Dyspnea, wheeze, cough - at rest, nocturnal, or exertional only |
| Frequency of attacks | Number of exacerbations in past 12 months |
| Severity markers | Emergency visits, hospitalizations, ICU admissions, prior intubations |
| Current medications | SABA, LABA, ICS dose, oral corticosteroids, leukotriene antagonists, theophylline |
| Last attack | Should be symptom-free for minimum 4-6 weeks before elective surgery |
| Triggers | Allergens, cold air, exercise, ASA/NSAIDs (critical for post-op analgesia planning), beta-blockers |
| URTI history | Recent URTI within 2-4 weeks = 2-10x increased bronchospasm risk; consider postponement |
Decision Point: Elective surgery should be postponed 4-6 weeks if the patient has active bronchospasm, recent exacerbation, or current wheeze at the time of assessment.
2. Physical Examination
- Auscultate chest: wheeze, prolonged expiration, reduced air entry
- Signs of severe disease: accessory muscle use, pulsus paradoxus >10 mmHg, central cyanosis, inability to speak full sentences
- Baseline SpO2 on room air
- Signs of steroid side effects (moon face, central obesity, proximal myopathy, skin fragility - alert to adrenal suppression)
3. Investigations
| Investigation | Finding | Significance |
|---|---|---|
| Spirometry | FEV1, FEV1/FVC, FEF 25-75%, PEFR | Assess severity and reversibility post-bronchodilator. PEFR >70% predicted = well-controlled |
| Chest X-ray | Hyperinflation, flattened diaphragm, hyperlucent fields, small heart | Air trapping; rule out pneumothorax, infection, consolidation |
| ABG | PaO2, PaCO2, pH | Reserved for FEV1 <50% or active distress. Even mild hypercapnia = severe disease, impending failure |
| CBC | Eosinophilia, polycythemia | Allergy, chronic hypoxia |
| Serum electrolytes | Hypokalemia | From beta-agonist therapy |
| ECG | Right heart strain, P pulmonale | Chronic severe asthma |
| Serum theophylline | Therapeutic range 10-20 mcg/mL | Toxicity risk if using aminophylline perioperatively |
Exam point: Spirometry has limited value in predicting postoperative pulmonary complications outside cardiothoracic surgery. Its perioperative role is to confirm and quantify obstruction and measure reversibility. (Berek & Novak / Morgan & Mikhail)
B. Pre-operative Optimization
The 3 AAAAI Recommended Interventions (American Academy of Allergy, Asthma and Immunology):
- Review asthmatic control, including need for oral steroids
- Optimize symptomatic control with long-acting pharmacotherapy, including oral steroids if needed
- For patients on oral steroids within 6 months, or large-dose ICS users - consider perioperative stress-dose steroids
Pharmacological Optimization:
| Drug Class | Action | Perioperative Use |
|---|---|---|
| SABA (Salbutamol/albuterol) | Bronchodilation | Continue; give 2-4 puffs 15-20 min before induction on morning of surgery |
| LABA (Salmeterol, formoterol) | Sustained bronchodilation | Continue up to the day of surgery |
| ICS (Budesonide, fluticasone) | Anti-inflammatory | Continue; do NOT stop |
| Oral corticosteroids | Anti-inflammatory | Continue; add stress-dosing if applicable |
| LTRA (Montelukast) | Anti-inflammatory, anti-leukotriene | Continue |
| Theophylline/aminophylline | Bronchodilation | Continue; check levels |
| ICS + SABA x 5 days pre-op | Reduce airway inflammation | Combined 5-day regimen shown to decrease perioperative bronchospasm risk (Berek & Novak) |
Stress-Dose Steroids:
| Indication | Regimen |
|---|---|
| Oral steroids >5 mg prednisolone/day currently or within past 6 months | Hydrocortisone 100 mg IV at induction, then 50-100 mg q8h for 24 h, taper to baseline in 1-2 days |
| Large dose ICS users | Consider same regimen |
| Minor day-surgery procedure + well-controlled on ICS only | Usually not required |
Pre-medication:
| Drug | Use | Note |
|---|---|---|
| Midazolam 1-2 mg IV/oral | Anxiolysis - reduces emotional trigger | Preferred |
| Glycopyrrolate 0.2 mg IM/IV | Anti-sialagogue if ketamine planned | Less tachycardia than atropine |
| Salbutamol nebulization | Pre-induction bronchodilation | In moderate-severe asthma |
| Pantoprazole 40 mg oral (night before + morning) | Aspiration prophylaxis | Avoid H2 blockers - see below |
| Dexamethasone 8 mg IV at induction | Anti-emetic + airway anti-inflammatory | Dual benefit in laparoscopy |
Critical Exam Point - H2 Blockers: Ranitidine, famotidine, and cimetidine are contraindicated as premedication in asthmatics. H2 receptor activation normally produces bronchodilation. Blocking H2 while leaving H1 unopposed means any histamine release will cause unmitigated bronchoconstriction via H1. Use PPI instead. (Morgan & Mikhail, 7e)
Non-pharmacological:
- Smoking cessation: minimum 12-24 hours improves CO levels and oxygenation; 8 weeks for significant pulmonary benefit; 2 months reduces post-op pulmonary complication risk
- Chest physiotherapy and breathing exercises if secretions present
- Treat active respiratory infection before surgery
- Patient counselling and anxiety reduction (emotional stress triggers bronchospasm)
PART II: INTRA-OPERATIVE MANAGEMENT
Understanding the Added Challenge: CO2 Pneumoperitoneum
Laparoscopic cholecystectomy mandates general anaesthesia with endotracheal intubation. The CO2 pneumoperitoneum imposes significant respiratory changes that are particularly hazardous in the asthmatic.
Table: Pulmonary Changes During Laparoscopy (Barash, 9e)
| Anatomic Displacement | V/Q Mismatch | Altered Lung Mechanics |
|---|---|---|
| Cephalad diaphragm displacement | Lung volume reduction / uneven gas distribution | ↓ Lung compliance |
| Diaphragm elevation | ↑ Alveolar-arterial O2 gradient | ↑ Lung resistance |
| Risk of endobronchial intubation (tube migration with head-down tilt) | ↑ Airway pressure | ↑ Pleural pressure |
- Peak airway pressure increases by 50%, plateau pressure by 81% during CO2 pneumoperitoneum
- Bronchopulmonary compliance decreases by 47% (Maingot's Abdominal Operations)
- CO2 absorbed across peritoneum → hypercapnia/respiratory acidosis
- Trendelenburg position further reduces FRC, worsens atelectasis and V/Q mismatch
- These effects are compounded on top of pre-existing airway obstruction in an asthmatic
A. Choice of Anaesthetic Technique
Regional anaesthesia alone is not suitable for laparoscopic cholecystectomy - it requires pneumoperitoneum, Trendelenburg positioning, and muscle relaxation, all of which mandate GETA.
Note: High spinal/epidural (T1-T4) can block sympathetic bronchodilator tone, allowing unopposed parasympathetic bronchoconstriction. Therefore, regional anaesthesia is not a preferred approach for this case. (Morgan & Mikhail, 7e)
Plan: General Anaesthesia with Endotracheal Intubation
B. Induction
Preferred Induction Agents:
| Agent | Dose | Properties | Recommendation |
|---|---|---|---|
| Propofol | 1.5-2.5 mg/kg | Bronchodilation, attenuates airway reflexes, smooth induction | FIRST CHOICE |
| Ketamine | 1-2 mg/kg | Sympathomimetic bronchodilation + direct smooth muscle relaxation; also provides analgesia | Preferred if hemodynamically unstable |
| Etomidate | 0.3 mg/kg | Cardiovascularly neutral; no histamine release; no bronchodilation | Acceptable if cardiovascular compromise |
| AVOID - Thiopentone | - | Histamine release; precipitates bronchospasm | Contraindicated |
Pre-intubation bronchospasm prevention:
- Additional bolus of induction agent before laryngoscopy
- OR ventilate with 2-3 MAC sevoflurane for 5 min before intubation
- IV or intratracheal lidocaine 1-2 mg/kg to blunt laryngeal reflexes
- Caution: Intratracheal lidocaine itself can trigger bronchospasm if anaesthesia is too light
- Ensure adequate depth of anaesthesia before any airway instrumentation - this is the single most important preventive measure
Airway Device:
- LMA (Proseal/Supreme) can be considered if airway is easy and aspiration risk is low - avoids tracheal stimulation entirely
- Endotracheal tube if RSI required (full stomach), obese, or surgical factors demand full relaxation and airway control
- If ETT: use appropriate size; confirm bilateral equal air entry immediately after intubation and after each position change (risk of tube migration in Trendelenburg)
C. Muscle Relaxants
| Agent | Histamine Release | Recommendation |
|---|---|---|
| Vecuronium | None | Preferred |
| Rocuronium | None | Preferred; enables RSI with sugammadex reversal |
| Cisatracurium | Minimal (unlike atracurium) | Acceptable |
| Succinylcholine | Minimal; rarely causes histamine release | Generally safe; acceptable for RSI |
| Atracurium | Significant | Avoid in asthmatics |
| Mivacurium | Significant | Avoid |
D. Maintenance
| Component | Drug of Choice | Rationale |
|---|---|---|
| Volatile agent | Sevoflurane | Most potent bronchodilator of all volatiles; smooth, non-pungent; ideal for asthmatics |
| Alternative volatile | Isoflurane | Bronchodilates; more pungent - do not use for inhalation induction |
| AVOID | Desflurane | Potent airway irritant; increases airway resistance; contraindicated in asthmatics |
| TIVA alternative | Propofol infusion | Excellent when volatiles unsuitable; maintains airway quiescence |
| Opioids | Fentanyl, remifentanil | Minimal/no histamine release; preferred |
| AVOID opioids | Morphine, meperidine (pethidine) | Significant histamine release |
| N2O | Avoid | Expands bowel gas, worsens surgical field in laparoscopy; no benefit |
E. Ventilation Strategy
| Parameter | Standard | Asthmatic + Pneumoperitoneum |
|---|---|---|
| Tidal volume | 7-8 mL/kg IBW | 6 mL/kg IBW (lung-protective) |
| I:E ratio | 1:2 | 1:3 to 1:4 (prolonged expiration to prevent air trapping) |
| PEEP | 5 cmH2O | 3-5 cmH2O (titrate; beware auto-PEEP) |
| RR | 12-14/min | Increase by ~15-25% to compensate for CO2 absorption from pneumoperitoneum |
| FiO2 | 0.4-0.5 | 0.5-1.0, titrate to SpO2 >95% |
| ETCO2 target | 35-40 mmHg | Accept 45-55 mmHg (permissive hypercapnia); aggressive hyperventilation worsens auto-PEEP |
| Insufflation pressure | < 15 mmHg | Keep < 12-15 mmHg; higher pressures worsen airway pressure and risk AKI |
| Gas humidification | Preferred | Mandatory - warm humidified gases throughout |
- Pre-emptively increase minute ventilation by ~15-25% before insufflation to compensate for CO2 absorption
- Use alveolar recruitment maneuvers at safe intervals to counter atelectasis
- Monitor for auto-PEEP (incomplete expiration): increase expiratory time, reduce RR, reduce tidal volume
F. Monitoring
- Standard ASA monitors (SpO2, ETCO2, ECG, NIBP, temperature)
- Capnography waveform - earliest indicator of expiratory obstruction
- Airway pressures: peak AND plateau pressure (plateau unchanged in bronchospasm = pure resistance problem)
- Neuromuscular blockade monitoring (TOF) - essential; adequate relaxation reduces insufflation pressure needed
- Arterial line if severe asthma, significant co-morbidities, or arterial blood gas monitoring required
G. Intraoperative Bronchospasm - Recognition and Management
Capnograph of Expiratory Obstruction:
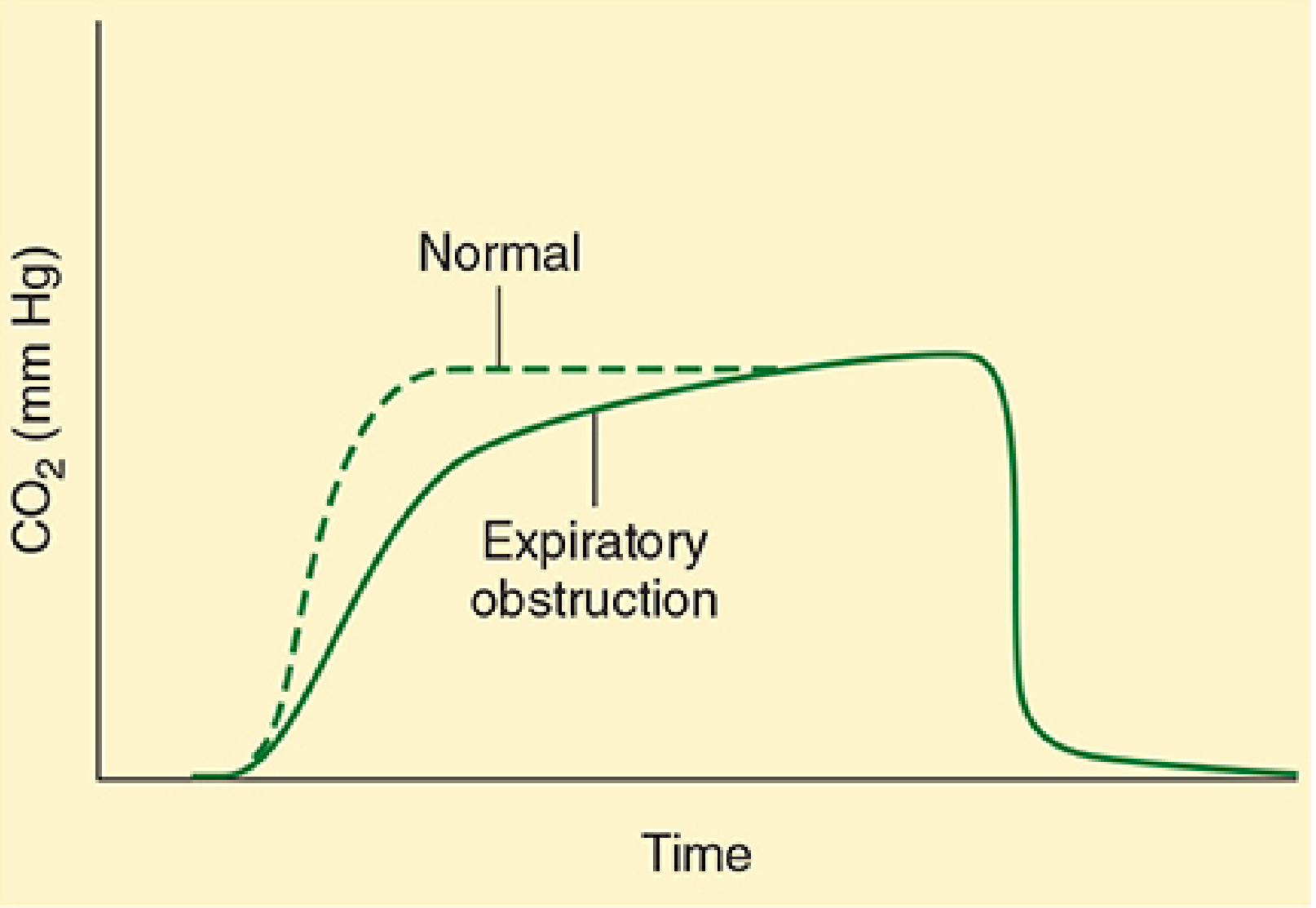
The solid line (expiratory obstruction) shows a slowly rising "shark fin" ETCO2 waveform vs. the dashed normal square waveform. This is the EARLIEST sign of airway obstruction. (Morgan & Mikhail, 7e, Fig. 24-2)
Recognition of Intraoperative Bronchospasm:
| Feature | Finding |
|---|---|
| Auscultation | Bilateral expiratory wheeze |
| Airway pressures | ↑ Peak inspiratory pressure; plateau pressure unchanged (pure resistance) |
| Tidal volumes | ↓ Exhaled tidal volumes |
| Capnography | Slowly rising "shark fin" or sawtooth ETCO2 trace |
| SpO2 | Progressive desaturation |
| Chest movement | Incomplete expiration, hyperinflation |
Differential Diagnosis of Intraoperative "Wheeze / High Airway Pressure" (MUST know for exam)
| Cause | Distinguishing Feature |
|---|---|
| True bronchospasm | Bilateral wheeze; ↑ peak, plateau unchanged; no tube issue |
| Endobronchial intubation | Unilateral breath sounds; tube too deep (common in Trendelenburg) |
| Kinked / obstructed ETT | Pass suction catheter; no air movement at tube end |
| Overinflated ETT cuff | Cuff pressure check |
| Light anaesthesia / straining | Clinical context; patient moving |
| Pulmonary oedema | Pink frothy secretions; crepitations; ↑ plateau pressure |
| Pulmonary embolism | Sudden ETCO2 drop; haemodynamic collapse |
| Tension pneumothorax | Unilateral; tracheal deviation; haemodynamic instability; ↑ both peak AND plateau |
| Anaphylaxis | Rash; haemodynamic collapse; concurrent bronchospasm |
Stepwise Treatment of Intraoperative Bronchospasm:
| Step | Intervention | Dose | Notes |
|---|---|---|---|
| 1 | FiO2 = 1.0 immediately | 100% O2 | While identifying and treating cause |
| 2 | Deepen anaesthesia | ↑ Sevoflurane concentration | Eliminate trigger; remove offending drug; check tube position |
| 3 | Inhaled SABA via ETT | Salbutamol 4-8 puffs via MDI adaptor | First-line bronchodilator |
| 4 | IV Hydrocortisone | 100-200 mg IV bolus | Especially in steroid-dependent patients; onset 4-6 hours |
| 5 | IV Magnesium sulphate | 2 g IV over 20 min | Smooth muscle relaxation; effective adjunct |
| 6 | IV/Nebulized Ipratropium | 0.5 mg nebulized | Anticholinergic bronchodilation; add-on |
| 7 | IV Ketamine | 0.5-1 mg/kg bolus | Bronchodilation + deepens anaesthesia |
| 8 | IV Aminophylline | 5 mg/kg over 30 min (loading) | Narrow therapeutic index; last resort if others fail; monitor ECG |
| 9 | IV Epinephrine (adrenaline) | 0.1-0.3 mcg/kg/min infusion | Life-saving for refractory bronchospasm |
H. Reversal and Extubation
Neuromuscular Reversal:
| Agent | Recommendation | Rationale |
|---|---|---|
| Sugammadex (if rocuronium/vecuronium) | Preferred | Directly encapsulates relaxant; avoids neostigmine-induced ↑ACh and potential bronchospasm |
| Neostigmine + glycopyrrolate | Acceptable if sugammadex unavailable | Glycopyrrolate must precede neostigmine; reduces muscarinic side effects |
| Neostigmine alone | Avoid | Unopposed muscarinic stimulation → bronchoconstriction |
Extubation Strategy:
| Approach | Indication | Technique |
|---|---|---|
| Deep extubation (preferred) | Easy airway, no aspiration risk, no full stomach | Remove ETT at Guedel plane 2-3 (before return of airway reflexes); eliminates extubation-triggered bronchospasm |
| Awake extubation | Difficult airway, obesity, full stomach, GERD | Pre-treat with IV lidocaine 1.5-2 mg/kg at emergence; ensure no wheeze before extubating |
| LMA exchange | If ETT used, well-tolerated LMA exchange possible | Remove ETT while deeply anaesthetised, insert LMA, then awake removal |
- Ensure patient is wheeze-free before extubation
- Ensure complete neuromuscular reversal (TOF ratio ≥ 0.9)
- IV Lidocaine 1.5-2 mg/kg 90 seconds before extubation blunts airway reflexes on emergence (Morgan & Mikhail, 7e)
- Avoid deep suctioning at light planes - potent bronchospasm trigger
PART III: POST-OPERATIVE MANAGEMENT
A. Immediate Post-Operative (Recovery Room / PACU)
| Priority | Intervention |
|---|---|
| O2 supplementation | 28-40% via facemask for minimum 4-6 hours; use humidified O2 |
| SpO2 monitoring | Continuous; target ≥95% |
| Resume all bronchodilators | Immediately post-extubation - SABA + ICS |
| Salbutamol nebulization | 2.5-5 mg q4-6h for at least 24 hours in moderate-severe asthma |
| Chest auscultation | Rule out wheeze, atelectasis, pneumothorax |
| Position | Semi-recumbent (30-45°) - maximizes FRC, reduces atelectasis |
| CPAP/BiPAP | Consider if SpO2 <92% despite O2, or significant atelectasis |
| Temperature | Keep patient warm - cold dry air is a bronchospasm trigger |
B. Post-operative Analgesia - Critical Consideration
Inadequate analgesia → pain splinting → atelectasis → hypoxemia. But respiratory-depressant drugs add risk. Multimodal, opioid-sparing analgesia is the gold standard.
| Analgesic | Dose | Safety in Asthma | Notes |
|---|---|---|---|
| Paracetamol (acetaminophen) | 1 g IV/oral q6h | Safe | First-line; no bronchospasm risk |
| Fentanyl (IV PCA or titrated) | 25-50 mcg boluses | Safe - minimal histamine | Preferred opioid if needed |
| TAP block (Transversus Abdominis Plane) | Bupivacaine 0.25% | Safe | Excellent opioid-sparing for laparoscopic ports |
| Port-site local anaesthetic | Bupivacaine 0.25% | Safe | Simple, effective |
| COX-2 inhibitors (Celecoxib, Etoricoxib) | Per guidelines | Generally safe | Safer than non-selective NSAIDs in non-NSAID-sensitive asthmatics |
| Tramadol | 50-100 mg oral/IV | Use with caution | Histamine release; avoid |
| Morphine / Meperidine | - | Avoid | Histamine release → bronchospasm |
NSAID Warning - Aspirin/NSAID-Exacerbated Respiratory Disease (AERD / Samter's Triad):
| Feature | Detail |
|---|---|
| Definition | Asthma + Nasal polyps + NSAID/Aspirin sensitivity |
| Prevalence | ~5-10% of all asthmatics |
| Mechanism | COX-1 inhibition → ↓ PGE2 (bronchodilatory) → ↑ Leukotrienes → bronchoconstriction |
| Contraindicated drugs | All non-selective NSAIDs (ketorolac, diclofenac, ibuprofen, naproxen, aspirin) |
| Safe alternatives | Paracetamol, COX-2 inhibitors (celecoxib), opioids (fentanyl) |
| Exam critical | Always ask about NSAID/aspirin tolerance BEFORE prescribing post-op analgesia |
C. Post-operative Respiratory Care
| Intervention | Detail |
|---|---|
| Deep breathing exercises | Start in PACU; 10 deep breaths every hour |
| Incentive spirometry | Target ≥70% predicted; commence as soon as alert |
| Early ambulation | Within 4-6 hours for laparoscopic cholecystectomy (day-surgery procedure) |
| Chest physiotherapy | If secretions are increased or atelectasis present |
| Humidified O2 | Continue until tolerating room air with SpO2 ≥95% |
| Postural drainage | If mucus plugging present |
D. Shoulder Tip Pain (Unique to Laparoscopy)
- Caused by residual CO2 accumulating under the diaphragm, irritating the phrenic nerve (referred to C3-C5 dermatome = shoulder)
- Ensure adequate CO2 desufflation at end of surgery
- Treatment: Semi-recumbent positioning, paracetamol, COX-2 inhibitors (if not NSAID-sensitive), warm packs
E. Steroid Management Post-operative
| Scenario | Action |
|---|---|
| Stress-dose steroids given intraoperatively | Taper hydrocortisone to baseline regimen within 24-48 hours |
| Patient on chronic oral prednisolone | Do NOT abruptly stop; continue maintenance dose |
| Monitoring | Blood glucose q6h (steroid-induced hyperglycemia); fluid balance |
F. Discharge Criteria (Day Surgery - Laparoscopic Cholecystectomy)
- No wheeze on auscultation
- SpO2 ≥ 95% on room air for ≥30 min
- Pain controlled on oral analgesics
- Tolerating oral fluids; passed urine
- Vital signs stable
- Written discharge instructions including asthma action plan if worsening wheeze/dyspnoea at home
- Review appointment within 24-48 hours
EXAM-CRITICAL TABLES (HIGH-YIELD)
Table 1: Drugs to PREFER vs. AVOID in Asthma - Comprehensive
| Drug Category | Prefer | Avoid |
|---|---|---|
| Induction agents | Propofol, Ketamine, Etomidate | Thiopentone (histamine release) |
| Muscle relaxants | Vecuronium, Rocuronium, Cisatracurium, Succinylcholine | Atracurium, Mivacurium (histamine) |
| Volatile agents | Sevoflurane (1st choice), Isoflurane | Desflurane (airway irritant) |
| Opioids | Fentanyl, Remifentanil, Alfentanil | Morphine, Meperidine, Tramadol (histamine) |
| NMB reversal | Sugammadex (preferred) | Neostigmine alone |
| Analgesics | Paracetamol, Fentanyl, COX-2 inhibitors, TAP block | NSAIDs (if NSAID-sensitive asthma) |
| Antiemetics | Ondansetron, Dexamethasone | - |
| Aspiration prophylaxis | Proton pump inhibitors (pantoprazole, omeprazole) | H2 blockers (ranitidine, famotidine) - contraindicated |
| Plasma expanders | Crystalloids, Albumin | Dextran, Gelatin (histamine) |
| Antibiotics | Cephalosporins, fluoroquinolones | Penicillins if penicillin-allergic; vancomycin (histamine) |
| Beta-blockers | Avoid all if possible | Non-selective beta-blockers (propranolol, atenolol) - absolute contraindication; cause bronchoconstriction |
Table 2: Severity-Based Pre-operative Strategy
| GINA Severity | Characteristics | Pre-op Action |
|---|---|---|
| Intermittent (Step 1) | Symptoms <2x/week, PEFR >80% | SABA 2 puffs 20 min pre-induction; proceed |
| Mild persistent (Step 2) | Symptoms >2x/week, PEFR 80% | Add low-dose ICS; SABA pre-op; well-controlled = proceed |
| Moderate persistent (Step 3) | Daily symptoms, PEFR 60-80% | Low-medium ICS + LABA; 5-day oral prednisolone pre-op; spirometry; proceed only if well-controlled |
| Severe persistent (Step 4-5) | Continuous symptoms, PEFR <60% | Postpone 4-6 weeks; aggressive optimization; IV steroids; ICU post-op planning |
| Emergency surgery with active bronchospasm | Active wheeze, hypoxia | Nebulized salbutamol + IV hydrocortisone 200 mg + O2 for 2-4 hours → proceed; ABG monitoring; ICU post-op |
Table 3: Physiological Effects of CO2 Pneumoperitoneum in the Asthmatic
| System | Effect | Implication for Asthmatic |
|---|---|---|
| Respiratory compliance | ↓ by 47% during insufflation | Worsens air trapping; ↑ work of breathing |
| Peak airway pressure | ↑ by 50% | May be confused with bronchospasm; increases barotrauma risk |
| FRC / Vital Capacity | ↓ (diaphragm pushed up) | Atelectasis; V/Q mismatch |
| CO2 absorption | Hypercapnia, respiratory acidosis | Masks hypoventilation; need ↑ MV by 15-25% |
| Catecholamine release | Peritoneal stretch → sympathetic stimulation | May partially bronchodilate, but also increases myocardial O2 demand |
| Trendelenburg position | Further ↓ FRC; risk of tube migration | Compound respiratory compromise |
Table 4: Intraoperative Bronchospasm - Stepwise Drug Treatment
| Step | Drug | Dose | Mechanism |
|---|---|---|---|
| 1 | 100% O2 | FiO2 1.0 | Oxygenation while treating |
| 2 | Sevoflurane ↑ | 2-3 MAC | Bronchodilation + deepens anaesthesia |
| 3 | Salbutamol MDI via ETT | 4-8 puffs | Beta-2 agonist bronchodilation - first-line |
| 4 | IV Hydrocortisone | 200 mg IV | Anti-inflammatory; onset 4-6 h |
| 5 | IV MgSO4 | 2 g over 20 min | Ca2+ antagonism → smooth muscle relaxation |
| 6 | Ipratropium nebulized | 0.5 mg | Anticholinergic bronchodilation |
| 7 | IV Ketamine | 0.5-1 mg/kg | Sympathomimetic bronchodilation |
| 8 | IV Aminophylline | 5 mg/kg load over 30 min | PDE inhibition → ↑ cAMP → bronchodilation |
| 9 | IV Epinephrine | 0.1-0.3 mcg/kg/min | Refractory bronchospasm - life-saving |
Table 5: Extubation Decision in the Asthmatic
| Factor | Deep Extubation | Awake Extubation |
|---|---|---|
| Airway | Easy airway confirmed | Difficult airway - cannot risk losing control |
| Aspiration risk | Low - fasted, no GERD | Full stomach, morbid obesity, GERD |
| Bronchospasm risk | High - active asthmatic | High - but safety of airway control outweighs benefit |
| Technique | Remove ETT at plane 2-3; LMA exchange | IV lidocaine 1.5 mg/kg; ensure wheeze-free |
| Advantage | Eliminates extubation-triggered bronchospasm | Maintains airway protection |
Table 6: Post-operative Pulmonary Complications and Management
| Complication | Cause | Prevention | Treatment |
|---|---|---|---|
| Bronchospasm | Residual airway irritability, secretions, cold air | Resume bronchodilators early; humidified O2 | Nebulized salbutamol; IV hydrocortisone; O2 |
| Atelectasis | ↓ FRC post-laparoscopy, pain splinting, secretions | Incentive spirometry; early ambulation; adequate analgesia | Chest PT, deep breathing, CPAP |
| Hypoxaemia | V/Q mismatch, atelectasis, opioid sedation | O2 supplementation; opioid-sparing analgesia | Supplemental O2; CPAP/NIV |
| Pneumonia | Aspiration, atelectasis, secretion retention | Early mobilization; aspiration precautions | Antibiotics; physiotherapy |
| Shoulder tip pain | Residual subdiaphragmatic CO2 | Complete desufflation | Semi-recumbent; paracetamol; COX-2 |
| Subcutaneous emphysema | CO2 extravasation at port sites | Recognize early; check airway | Usually self-limiting; monitor airway |
| PONV | Laparoscopy, opioids | Dexamethasone + ondansetron at induction | Ondansetron, metoclopramide |
KEY EXAM POINTS TO REMEMBER
-
The single most important preventive measure for perioperative bronchospasm is ensuring adequate depth of anaesthesia before airway instrumentation.
-
H2 blockers are contraindicated as premedication - they leave H1 unopposed and worsen histamine-triggered bronchoconstriction.
-
Desflurane is absolutely avoided in asthmatics - it is the most pungent volatile agent and increases airway resistance.
-
Sevoflurane is the volatile agent of choice - most potent bronchodilator, smooth, non-irritant.
-
Deep extubation is preferred over awake extubation in asthmatics with an easy airway and no aspiration risk.
-
Sugammadex is preferred over neostigmine for NMB reversal - avoids cholinergic surge and its bronchospastic potential.
-
The "shark fin" capnograph (slowly rising ETCO2 on expiration) is the earliest and most sensitive indicator of expiratory obstruction intraoperatively.
-
Permissive hypercapnia is acceptable during laparoscopy in asthmatics - aggressive hyperventilation worsens auto-PEEP and barotrauma.
-
Always ask about NSAID/aspirin tolerance before prescribing any post-operative analgesia - Samter's triad (asthma + nasal polyps + NSAID sensitivity) affects ~5-10% of asthmatics.
-
CO2 pneumoperitoneum increases ETCO2 by 15-25% above baseline - pre-emptively increase minute ventilation before insufflation.
-
ETCO2 and peak airway pressure both rise during pneumoperitoneum - do not confuse this physiologic increase with bronchospasm. The key differentiator: bronchospasm shows rising PEAK with UNCHANGED PLATEAU; pneumoperitoneum raises both.
-
Dexamethasone 8 mg at induction serves double duty in laparoscopy - PONV prophylaxis AND airway anti-inflammatory effect.
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e | Miller's Anesthesia, 10e | Barash's Clinical Anesthesia, 9e | Berek & Novak's Gynecology | Maingot's Abdominal Operations
This is a shared conversation. Sign in to Orris to start your own chat.