X-ray basics to read
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Searching Images
normal chest X-ray anatomy labelled PA view
Finding Sources
Finding Sources
Reading File
Searching Images
chest X-ray pneumonia consolidation opacity
Searching Images
pleural effusion chest X-ray blunting costophrenic angle
Searching Images
pneumothorax chest X-ray absent lung markings
Now I have enough material from Grainger & Allison's Diagnostic Radiology and the medical image library. Let me compile a comprehensive, well-illustrated guide.
X-Ray Basics: How to Read a Chest Radiograph
1. Technical Assessment — Before You Read Any Pathology
Always assess film quality first. A poor-quality film produces false findings.
Rotation: The medial ends of both clavicles should be equidistant from the spinous process of the thoracic vertebra at the same level. Rotation causes one hemithorax to appear denser than the other.
Inspiration: Count posterior ribs. On adequate inspiration, the right hemidiaphragm should be visible at or below the 6th anterior rib / 10th posterior rib. Poor inspiration makes the heart look enlarged and the lung bases look congested.
Exposure:
- Underexposed → film too white; pulmonary vessels obscured
- Overexposed → film too dark; lesions missed
- Optimal: thoracic vertebral bodies just visible through the cardiac shadow
Projection:
- PA (posteroanterior): standard upright; patient stands facing the detector. Heart is not magnified. Preferred view.
- AP (anteroposterior): portable/supine; heart appears magnified (up to 20% larger); scapulae overlap lung fields. Do not call cardiomegaly on AP films.
2. A Systematic Approach — Use a Mnemonic Every Time
A consistent order prevents errors. A common approach: ABCDE
| Letter | Structures to assess |
|---|---|
| A — Airways | Trachea (midline?), carina angle (<70°), main bronchi |
| B — Bones & soft tissue | Ribs, clavicles, scapulae, vertebrae, soft tissues of neck/chest wall |
| C — Cardiac | Cardiac silhouette, cardiothoracic ratio, cardiac borders |
| D — Diaphragm | Domes, costophrenic angles, subdiaphragmatic air |
| E — Everything else | Lung fields, hila, mediastinum, devices/lines |
3. Normal Anatomy on a PA Chest X-Ray
Trachea: midline, slight rightward deviation at the carina is normal. Bifurcates at T4–T5 (angle of Louis).
Heart:
- Cardiothoracic (CT) ratio < 0.5 on PA film is normal (heart width / widest thoracic width)
- Right heart border = right atrium
- Left heart border (top-down) = aortic knob → pulmonary trunk → left atrial appendage → left ventricle
Hila: left hilum normally 0.5–1.5 cm higher than right. Hila are formed by pulmonary arteries and veins. Enlarged hila = lymphadenopathy, vascular engorgement, or mass.
Diaphragm: right dome is 1.5–2.5 cm higher than left (liver below). Both costophrenic angles should be sharp and acute.
Lung zones:
- Lungs are described in upper, middle, and lower zones (not lobes, on CXR)
- Pulmonary vessels visible radiating from hila; upper lobe vessels are smaller than lower lobe on erect film (if equal/larger = upper lobe diversion, a sign of pulmonary venous hypertension)
4. Key Signs and What They Mean
The Silhouette Sign
When a structure touches another of the same radiodensity, the border between them disappears. Loss of a border localises pathology:
- Loss of right heart border → right middle lobe consolidation/collapse
- Loss of left heart border → lingula disease
- Loss of hemidiaphragm outline → lower lobe consolidation
Air Bronchogram
Air-filled bronchi become visible within consolidated (fluid/pus-filled) lung. Indicates airspace consolidation (pneumonia, pulmonary oedema, infarction, neoplasm).
Kerley B Lines
Horizontal lines at the lung bases perpendicular to the pleura, 1–2 cm long. Represent fluid in interlobular septa. Classic sign of interstitial pulmonary oedema.
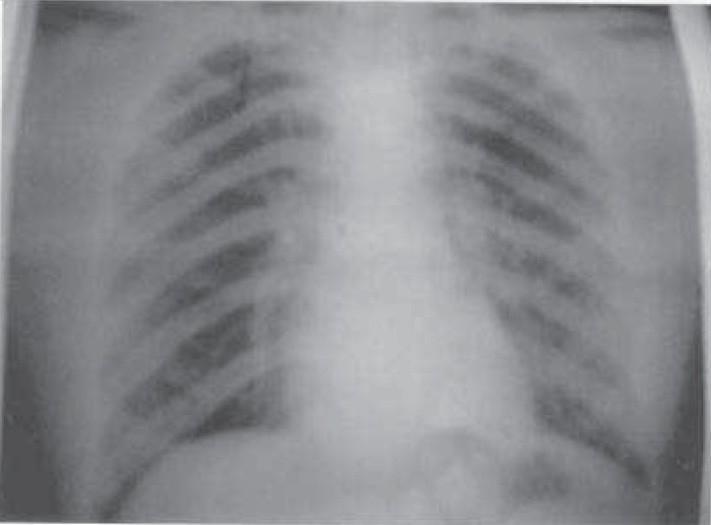
5. Common Pathologies
Consolidation (Pneumonia)

- Increased opacity with ill-defined borders
- Air bronchograms often present
- Loss of adjacent cardiac/diaphragmatic border (silhouette sign)
- Lobar distribution suggests bacterial pneumonia; patchy bilateral = atypical/viral
Pleural Effusion
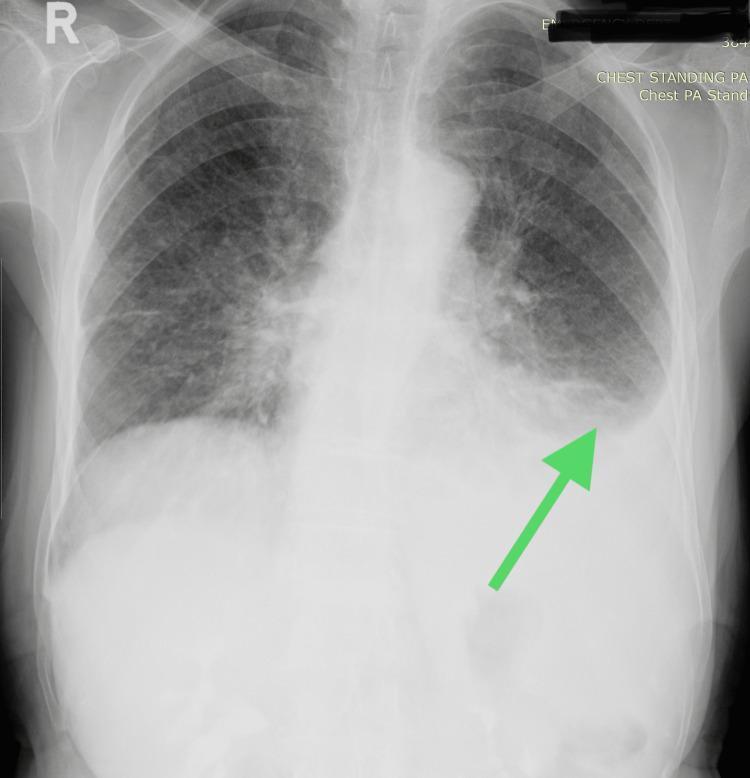
- Small effusion (200–500 mL): blunting of costophrenic angle
- Larger effusion: homogeneous opacity with concave upper border (meniscus sign) — higher laterally than medially
- Massive effusion: opacification of hemithorax with contralateral mediastinal shift
- Absent mediastinal shift with large effusion → suspect ipsilateral lung collapse or pleural malignancy (mesothelioma)
(Source: Grainger & Allison's Diagnostic Radiology)
Pneumothorax
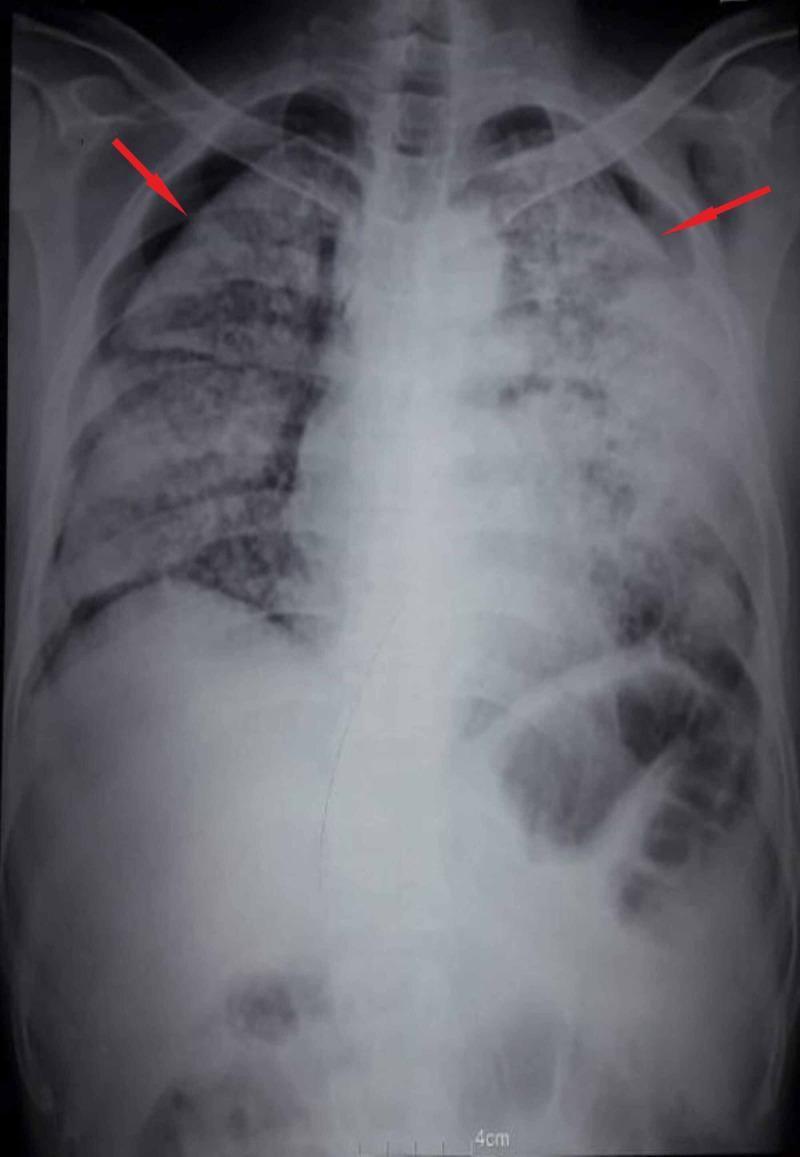
- Visible visceral pleural line with absent lung markings beyond it
- Peripheral hyper-lucency; no vascular markings in that zone
- Tension pneumothorax: tracheal deviation away from the affected side + contralateral mediastinal shift + ipsilateral hemidiaphragm depression → clinical emergency, do not wait for CXR if suspected
Cardiomegaly
- CT ratio > 0.5 on PA film
- Causes: left ventricular failure, dilated cardiomyopathy, pericardial effusion (globular "flask-shaped" heart)
Pulmonary Oedema
Radiological progression:
- Upper lobe blood diversion (PCWP ~18 mmHg)
- Kerley B lines, peribronchial cuffing (~20–25 mmHg)
- Bat-wing / butterfly pattern of alveolar oedema (>25 mmHg)
6. Approach to the Mediastinum
| Compartment | Contents | Causes of widening/mass |
|---|---|---|
| Anterior | Thymus, lymph nodes, fat | Thymoma, teratoma, thyroid, terrible lymphoma ("4 Ts") |
| Middle | Heart, great vessels, trachea, main bronchi | Aortic aneurysm, lymphadenopathy, pericardial cyst |
| Posterior | Oesophagus, descending aorta, paravertebral structures | Neurogenic tumour, oesophageal pathology |
Mediastinal widening >8 cm on PA = abnormal. On AP portable films, up to 8.5 cm can be normal due to magnification.
7. Diaphragm Assessment
- Sub-diaphragmatic free air (pneumoperitoneum): crescentic lucency under the diaphragm — surgical emergency
- Raised hemidiaphragm: phrenic nerve palsy, subphrenic abscess, basal collapse, hepatomegaly/splenomegaly
- Right hemidiaphragm normally higher by ~1.5 cm; if left is higher, suspect gastric/splenic pathology or left lower lobe collapse
8. Lines and Devices (ICU/Ward Films)
| Device | Correct position |
|---|---|
| Endotracheal tube | 2–4 cm above carina (at T4–T5) |
| Central venous catheter | Tip in SVC, at/just above right atrium |
| Nasogastric tube | Beyond the gastro-oesophageal junction; tip in stomach |
| Chest drain | Within pleural space; holes should all be inside thorax |
Summary: Quick-Reference Checklist
- ☐ Confirm patient ID and date
- ☐ Check projection (PA vs AP), rotation, inspiration, exposure
- ☐ Airways: trachea midline, carina angle
- ☐ Bones: rib fractures, lytic lesions, clavicles, spine
- ☐ Cardiac: CT ratio, borders, mediastinal width
- ☐ Diaphragm: domes, CP angles, sub-diaphragmatic air
- ☐ Lung fields: opacities, consolidation, pneumothorax, vascular pattern
- ☐ Hila: size, density, position
- ☐ Soft tissues: surgical emphysema, chest wall masses
- ☐ Lines/tubes: correct position
Sources: Grainger & Allison's Diagnostic Radiology (Nair, Barnett, Semple — Thoracic Imaging chapter); clinical image library.
This is a shared conversation. Sign in to Orris to start your own chat.