Tetanus definition
Reading File
Finding Sources
Reading File
Reading File
Tetanus - Definition
Tetanus is an acute infectious disease characterized by generalized rigidity and convulsive spasms of skeletal muscles, caused by a potent neurotoxin (tetanospasmin) produced by Clostridium tetani at the site of injury. It is also commonly called "lockjaw" due to the hallmark spasm of the jaw muscles (trismus).
The Organism
Clostridium tetani is a:
- Gram-positive, anaerobic, spore-forming bacillus
- Found naturally in soil and intestines of humans and animals
- Spores have a characteristic drumstick or tennis racket shape
- Enters the body through a wound, thriving in anaerobic (low-oxygen) conditions present in devitalized tissues
Mechanism (Pathobiology)
- C. tetani spores germinate in low-oxygen wounds and produce tetanospasmin (tetanus neurotoxin)
- The toxin is one of the most potent known microbial toxins - lethal at 2.5 ng/kg in humans
- It binds peripheral nerve terminals and is transported intra-axonally (~75-250 mm/day) to spinal neurons
- The light chain blocks release of neurotransmitters from inhibitory afferent motor neurons
- Loss of inhibition --> sustained, uncontrolled muscle contraction and tetanic spasms
- Toxin binding is irreversible - recovery depends on growth of new axon terminals
Key Clinical Features
- Incubation period: 3-21 days (mean 8 days); shorter = more severe disease
- Trismus (lockjaw) - initial complaint in ~75% of cases
- Risus sardonicus - spasm of facial muscles producing a characteristic grimace
- Opisthotonus - arching of the entire body due to paravertebral/extensor muscle spasm
- Reflex spasms triggered by even slight sensory stimuli (noise, touch)
- Laryngeal spasm leading to apnoea and potential respiratory arrest
- Autonomic involvement: labile BP, cardiac arrhythmias, diaphoresis, hyperthermia
- Patients typically remain lucid and afebrile unless complicated by secondary infection
Types
| Type | Frequency | Features |
|---|---|---|
| Generalized | 80-90% of US cases | Involves neck, jaw, all muscles |
| Local | Rare | Limited to muscle groups near wound |
| Neonatal | Common in low-income countries (~60,000 cases/year) | Via immature umbilical cord |
Sources: Goldman-Cecil Medicine International Edition; Bailey and Love's Short Practice of Surgery, 28th Ed.
Acute pancerititis
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Here is a comprehensive overview of Acute Pancreatitis:
Definition
Acute Pancreatitis (AP) is an acute inflammatory condition of the pancreas leading to enzymatic autodigestion and destruction of pancreatic tissue. It ranges from mild, self-limited disease to life-threatening sepsis and multiorgan failure. It is the most common pancreatic disease worldwide and one of the top reasons for hospitalization due to gastrointestinal disease in the United States.
Etiology (Causes)
| Category | Examples |
|---|---|
| Most common | Gallstones (40-70%), Chronic alcohol use (25-35%) |
| Toxic/Metabolic | Hypertriglyceridemia (>1000 mg/dL), hypercalcemia, uremia, drugs, scorpion venom |
| Mechanical/Obstructive | Biliary stones, post-ERCP, pancreas divisum, ampullary tumors, trauma |
| Infectious | Viral (mumps, coxsackievirus, HIV, CMV, EBV), bacterial (TB, Salmonella, Mycoplasma), parasitic (Ascaris) |
| Other | Autoimmune, vascular, idiopathic |
Smoking and diabetes are independent risk factors. Many "idiopathic" cases are thought to be due to occult microlithiasis.
Pathophysiology
Regardless of the trigger, the common pathway involves premature activation of digestive enzymes (especially trypsin) within the pancreas, leading to:
- Autodigestion of pancreatic parenchyma
- Local inflammatory response with release of cytokines
- Systemic inflammatory response (SIRS)
- In severe cases: distant organ injury (lungs, kidneys, cardiovascular system)
Classification (Atlanta Classification 2012)
By Type:
- Interstitial edematous pancreatitis - Most cases; diffuse inflammation + edema; usually resolves within the first week
- Necrotizing pancreatitis - ~5-10% of cases; involves pancreatic parenchyma ± surrounding tissue; necrosis may be sterile, liquefy, or become infected (infected = worse prognosis)
By Severity:
- Mild - No organ failure, no local or systemic complications
- Moderately severe - Transient organ failure (<48 hrs) and/or local complications
- Severe - Persistent organ failure (>48 hrs); mortality up to 30%
Clinical Features
Symptoms:
- Persistent epigastric or left upper quadrant pain, often radiating to the back, chest, or flanks
- Pain may be relieved by sitting up or bending forward
- Nausea, vomiting, anorexia
Signs:
- Fever, tachycardia (with inflammation)
- Hypotension and shock (severe cases)
- Jaundice (if obstructive cause)
- Cullen sign - bluish periumbilical discoloration (hemoperitoneum) - rare, poor prognosis
- Grey Turner sign - reddish-brown flank discoloration (retroperitoneal bleeding) - rare, poor prognosis
- Epigastric tenderness ± guarding
- Reduced/absent bowel sounds (ileus)
Diagnosis
Diagnosis requires at least 2 of the following 3 criteria:
- Abdominal pain characteristic of AP
- Serum lipase or amylase >3x the upper limit of normal
- Characteristic findings on abdominal imaging
Lab Tests:
- Lipase - preferred; more sensitive and specific than amylase; remains elevated ~1-2 weeks
- Amylase - less specific; elevated in many other conditions; may be falsely normal in alcohol/hypertriglyceridemia-induced AP
- ALT/AST/bilirubin - evaluate for biliary cause (ALT >3x normal has ~95% PPV for biliary pancreatitis)
- Serum calcium, triglycerides, CBC, BMP
Imaging:
- CT/MRI - not routine; indicated for diagnostic uncertainty, ruling out other pathology, or assessing complications (best after 48-72 hrs of failed therapy; necrosis best seen at 3-7 days)
- Ultrasound - first-line to identify gallstones
Severity Scoring
| System | Key Points |
|---|---|
| Ranson's criteria | Assessed at admission (5 criteria) and at 48 hours (6 criteria) |
| APACHE II | Applicable on admission |
| BISAP score | Bedside; 5 variables |
| CT Severity Index (CTSI) | Radiological grading |
Complications
Local:
- Acute peripancreatic fluid collections (<4 weeks)
- Pancreatic pseudocyst (>4 weeks, encapsulated, fluid only)
- Acute necrotic collection
- Walled-off necrosis (WON) (>4 weeks)
- Bowel necrosis, splenic/portal vein thrombosis, GI bleeding, gastric outlet obstruction
Systemic:
- SIRS, ARDS, pleural effusion (up to 50%; more often left-sided)
- Cardiovascular collapse, acute kidney injury
- Coagulopathy/DIC
- Hyperglycemia, hypocalcemia
Management Principles
- Fluid resuscitation - aggressive IV fluids (isotonic crystalloids preferred)
- Analgesia - adequate pain control
- Nutrition - early enteral feeding preferred over parenteral (nasogastric = nasojejunal in most cases)
- ERCP - reserved for concurrent cholangitis or biliary obstruction (not routine)
- Cholecystectomy - early (within 3 days) in mild biliary pancreatitis
- Antibiotics - only for confirmed infected necrosis (not prophylactic)
- ICU care - for organ failure and severe disease
Sources: Rosen's Emergency Medicine, 10th Ed.; Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Exg images
Finding Sources
Asking for Preferences
Acute pancerititissonographic images
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here are the sonographic (ultrasound) images of acute pancreatitis from Grainger & Allison's Diagnostic Radiology:
Sonographic Images of Acute Pancreatitis
Fig. 25.7 - Ultrasound in Oedematous (Interstitial) Pancreatitis
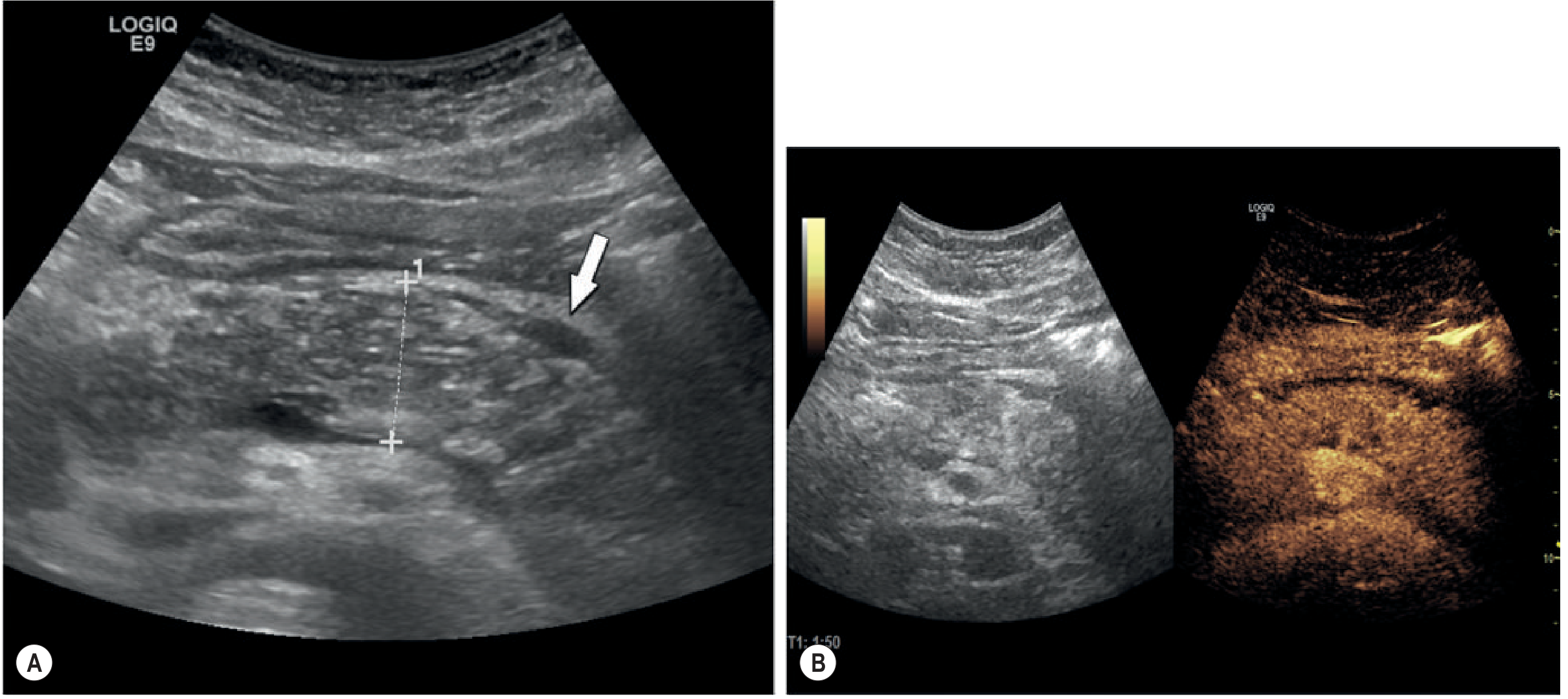
Panel A (B-mode ultrasound): Shows diffuse swelling of the pancreatic gland with heterogeneous echogenicity and a small rim of peripancreatic fluid (white arrow). The gland appears enlarged and the margins are ill-defined.
Panel B (Contrast-Enhanced Ultrasound - CEUS): Reveals homogeneous hyperenhancement nearly 2 minutes after contrast administration - characteristic of oedematous pancreatitis (viable, perfused tissue). This distinguishes it from necrotizing pancreatitis where areas of non-enhancement would be seen.
Normal Pancreas for Comparison (US panels D & E)
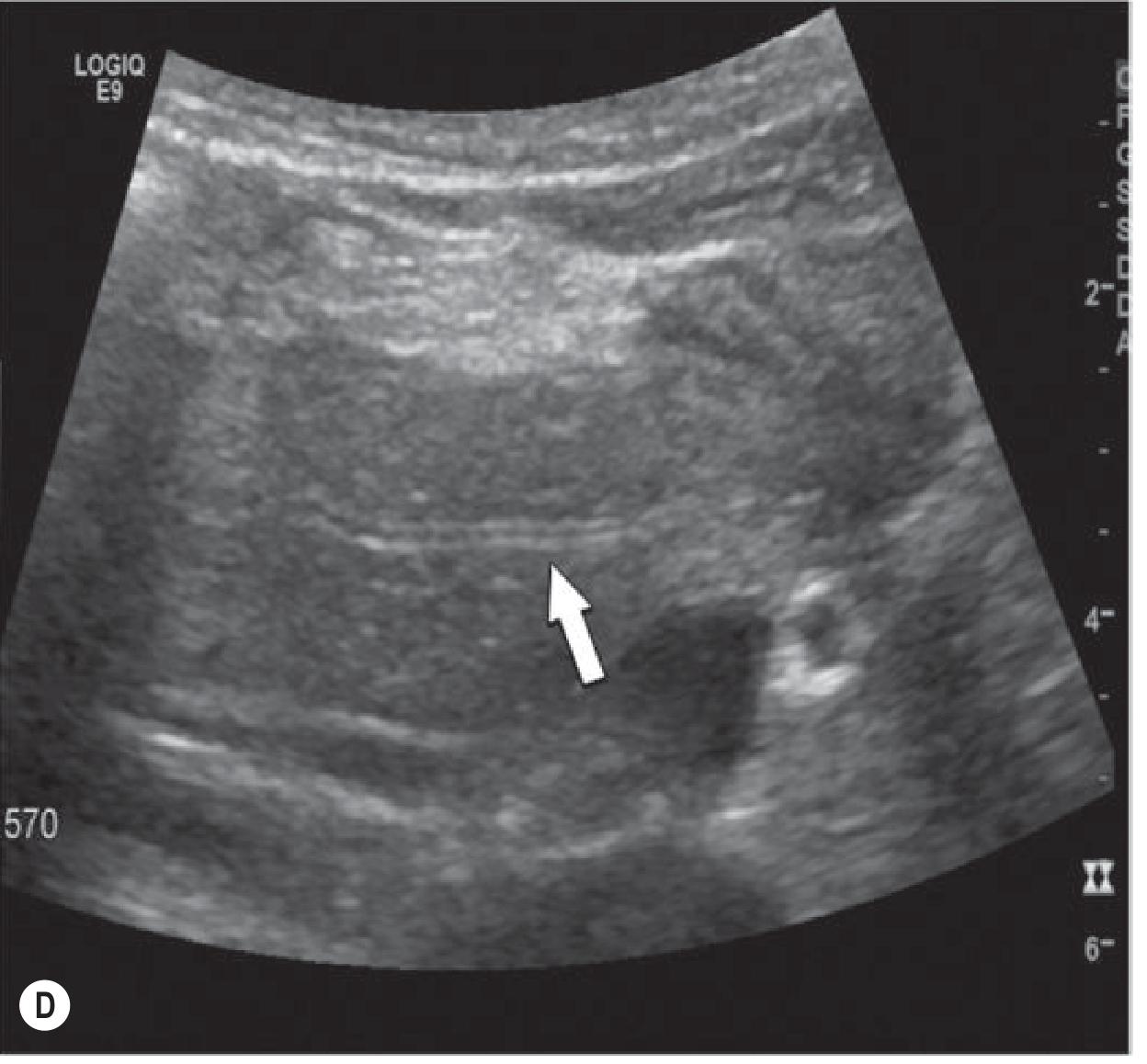
Panel D: Normal pancreatic head with homogeneous echogenicity. The arrow points to the normal-sized pancreatic duct, which is well visualised.
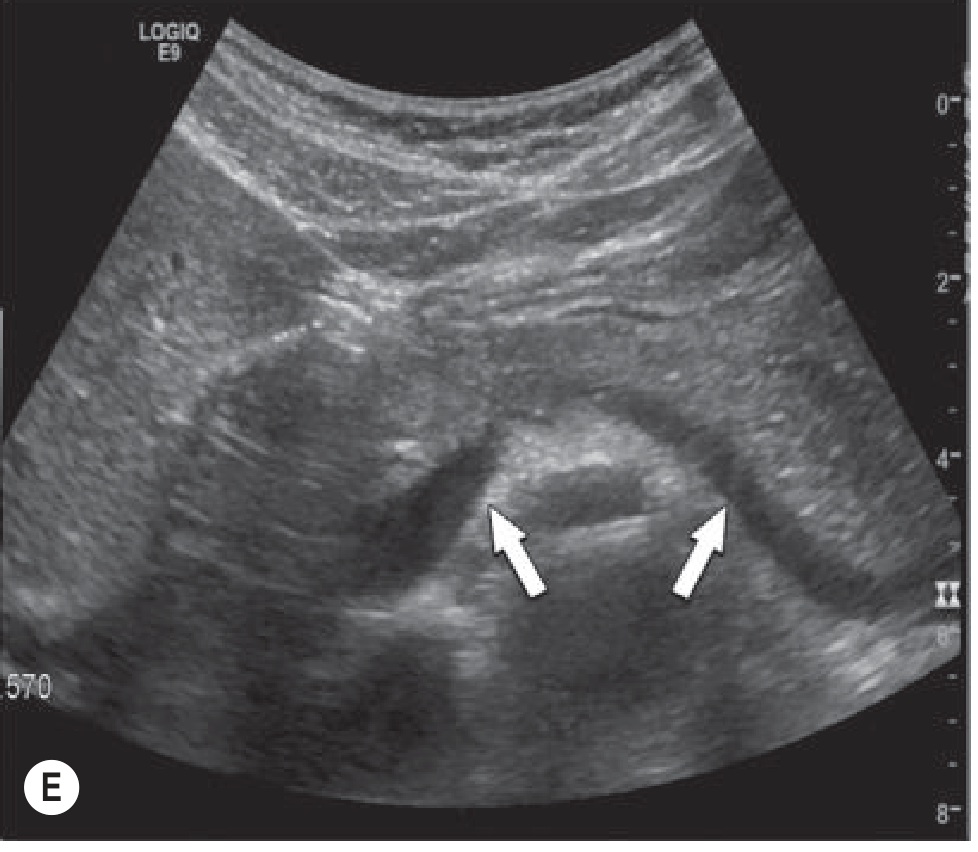
Panel E: Normal pancreatic body and part of the tail (arrows) seen anteriorly to the splenic vein. Normal smooth contour and uniform echogenicity - contrast this with the inflamed gland above.
Key Sonographic Features of Acute Pancreatitis
| Finding | Description |
|---|---|
| Gland size | Diffuse (or focal) enlargement |
| Echogenicity | Reduced (hypoechoic) due to oedema |
| Margins | Ill-defined, difficult to delineate |
| Peripancreatic fluid | Anechoic rim around the gland |
| Pancreatic duct | May be dilated if obstructed |
| CEUS | Homogeneous enhancement = oedematous; non-enhancing areas = necrosis |
Important note: US may appear entirely normal in up to 20-30% of mild acute pancreatitis cases. US cannot reliably detect pancreatic necrosis. Contrast-enhanced CT remains the gold standard for staging severity and detecting necrosis (best performed 48-72 hrs after onset).
Source: Grainger & Allison's Diagnostic Radiology, Chapter 25
Show CT imaging patterns in acute pancreatitis
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Here is a comprehensive visual tour of CT imaging patterns in acute pancreatitis, from mild to severe:
CT Imaging Patterns in Acute Pancreatitis
1. Timing of CT - Why It Matters
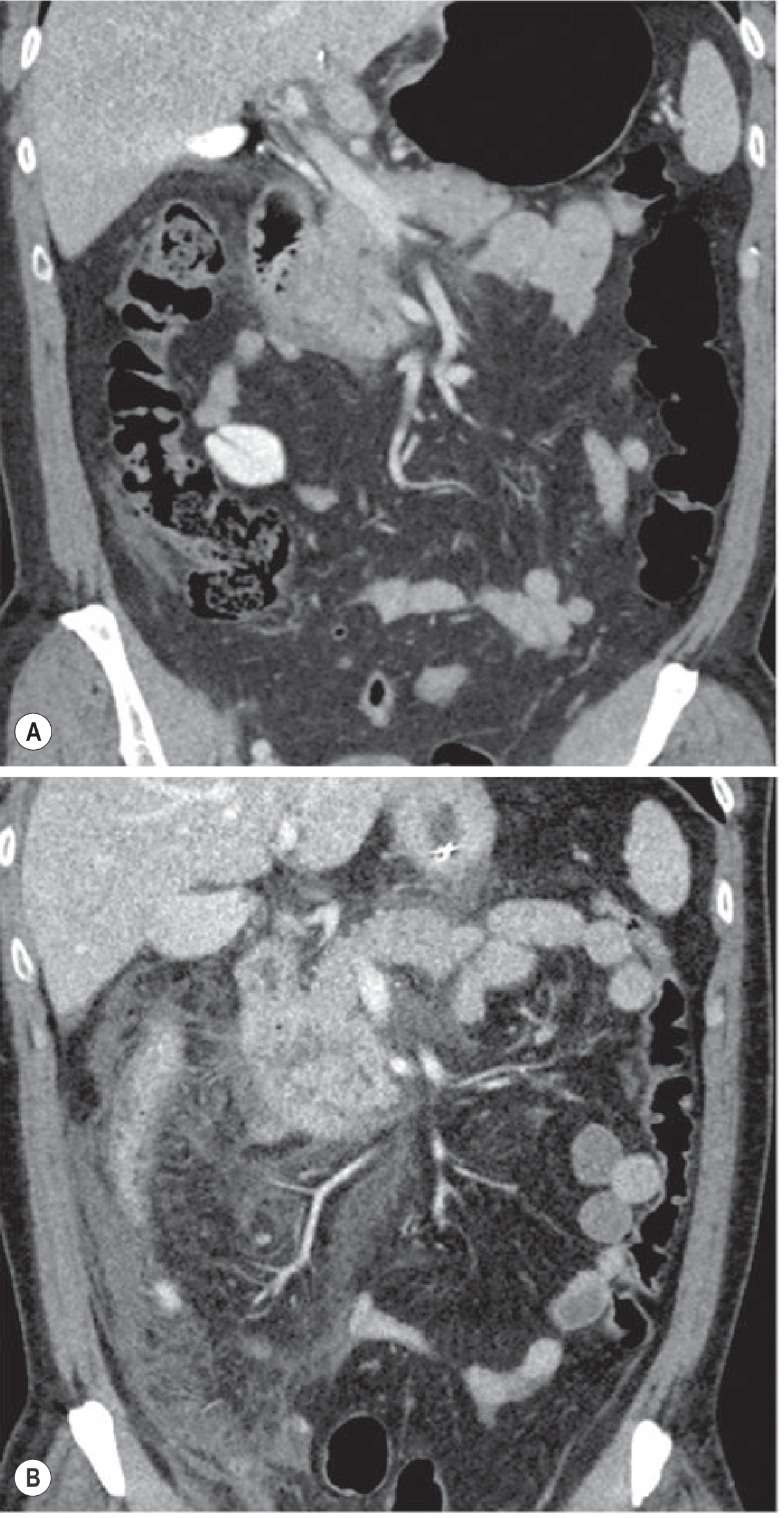
Fig. 25.8 - Appropriate Timing of CT Imaging
- Panel A (top): CT at 12 hours after onset - only minimal signs visible
- Panel B (bottom): Follow-up CT at Day 3 (due to clinical deterioration) - dramatically more severe inflammation is now apparent
Key teaching point: CT should NOT be done routinely in the first 24 hours. Necrosis takes 2-3 days to fully develop and may be underestimated early. Best performed at 48-72 hours in patients failing to improve.
2. Interstitial Oedematous Pancreatitis (Mild to Severe)
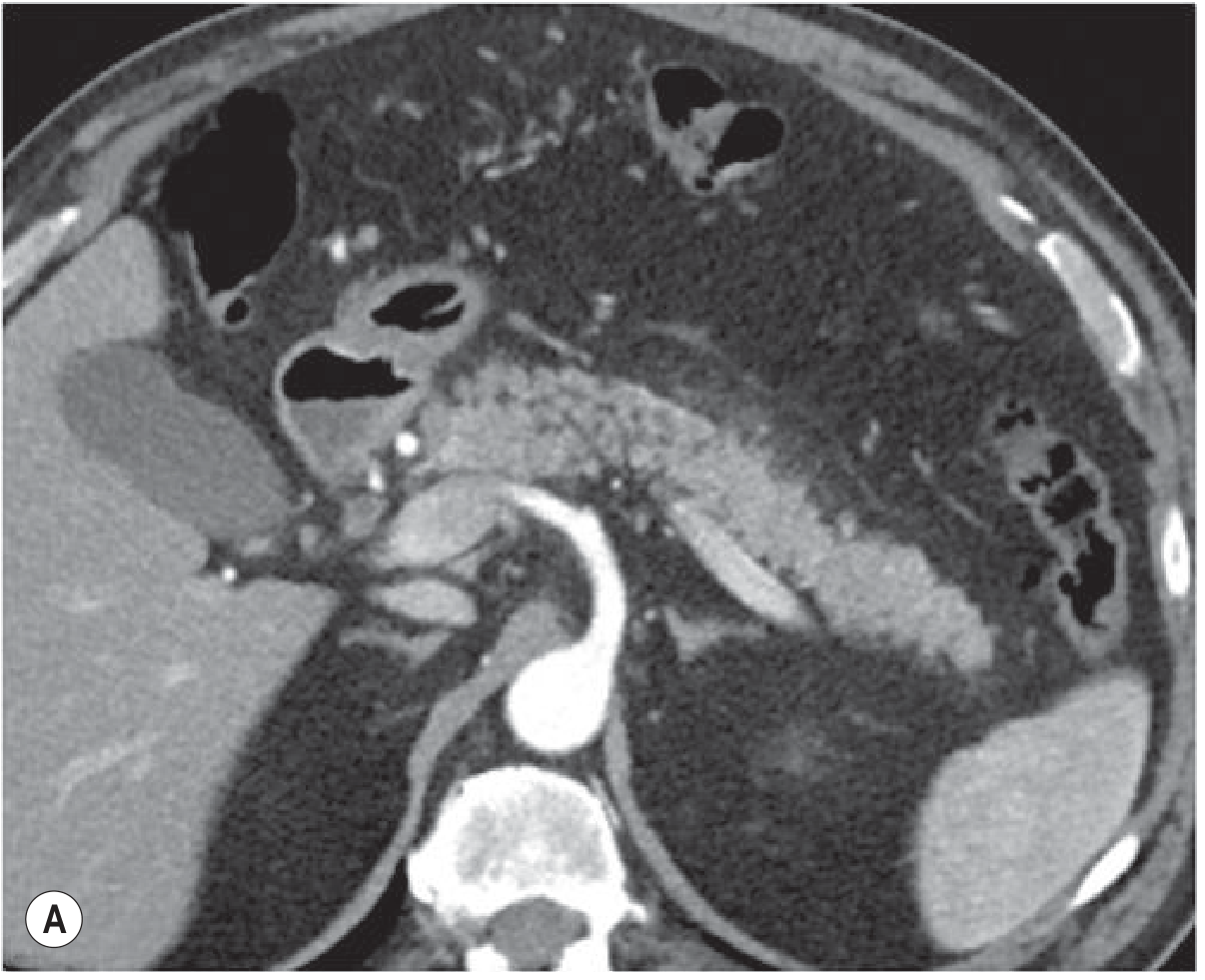
Fig. 25.11A - Mild Oedematous Pancreatitis: Gland swelling and minimal peripancreatic fat stranding ("mistiness" in peripancreatic fat). The pancreas still enhances uniformly, confirming viable tissue.
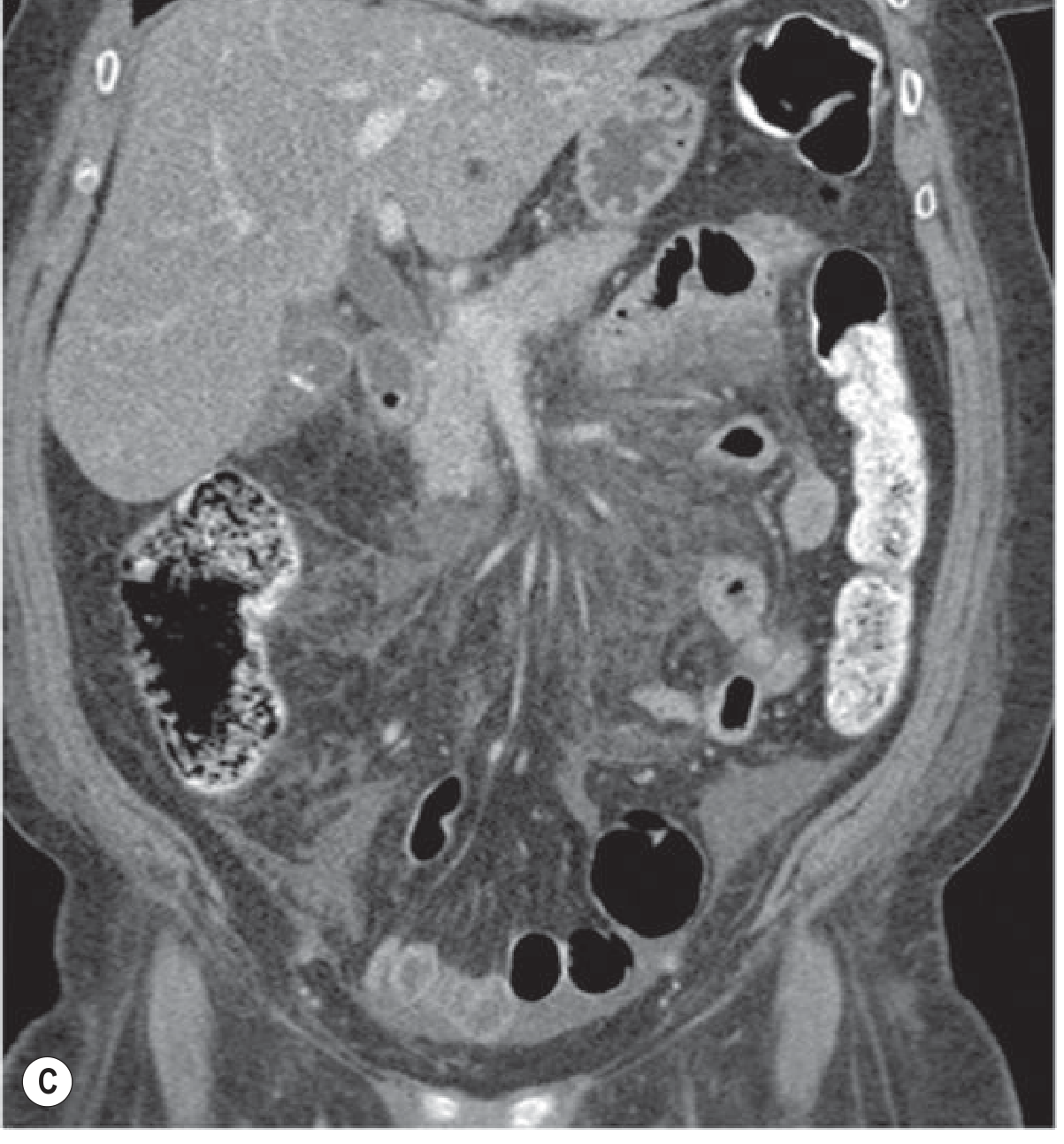
Fig. 25.11C - Severe Oedematous Pancreatitis: Extensive peripancreatic inflammation with fluid tracking into the paracolic gutter and pelvis - a poor prognostic sign. Fluid collections are called Acute Peripancreatic Fluid Collections (AFPC) at this stage - no wall, no solid debris.
3. Pseudocyst (Late Complication, >4 Weeks)
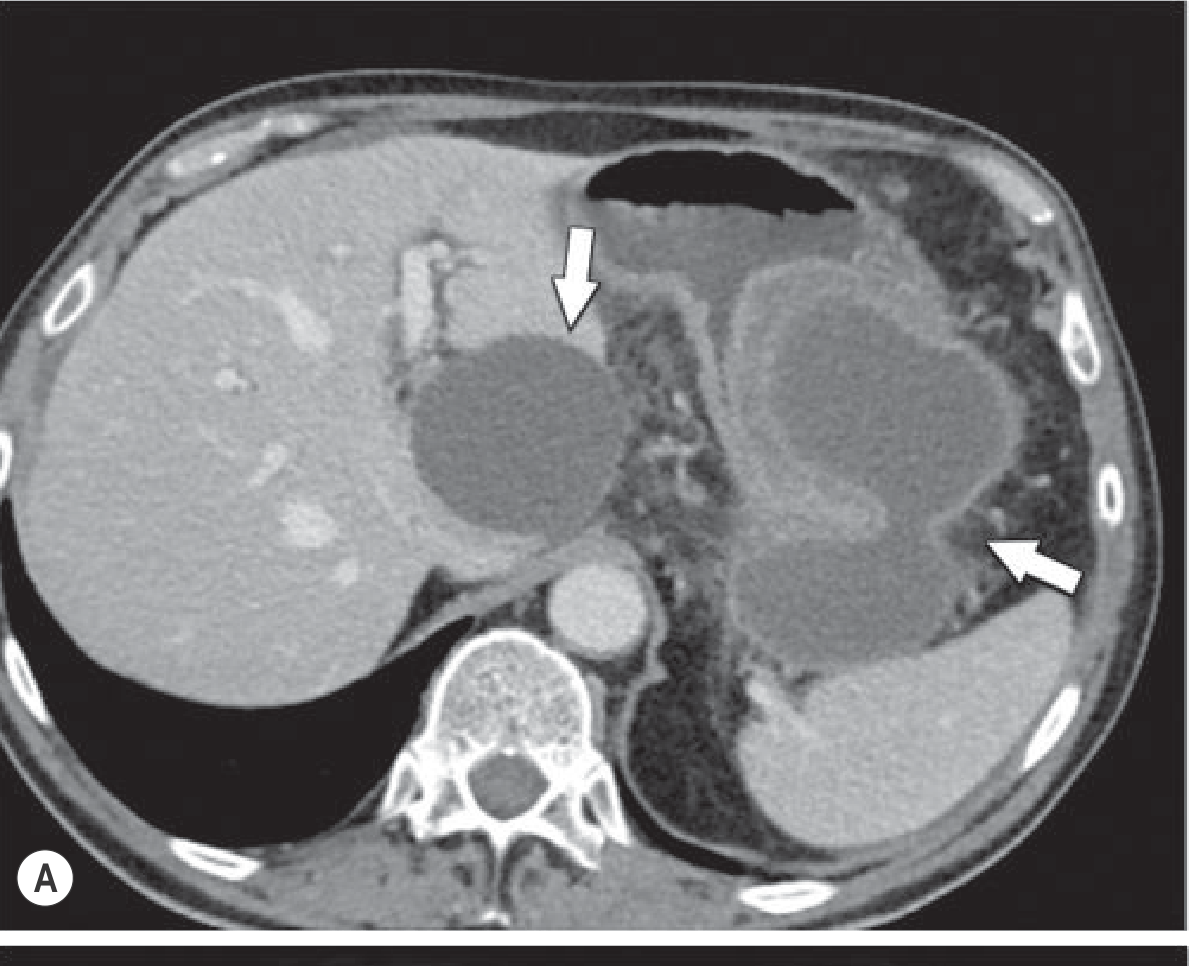
Fig. 25.12 - Pseudocyst After Oedematous Pancreatitis:
- Two unilocular fluid collections (arrows) - one extending into the fissure of the ligamentum venosum, the other in the omental bursa
- Characteristic features: homogeneous low-attenuation fluid, well-defined enhancing fibrous wall, no solid debris
-
70% resolve spontaneously
4. Necrotising Pancreatitis - Key CT Patterns
Fig. 25.14 - Acute Necrotising Pancreatitis - Morphological Types:
The hallmark is areas of non-enhancement of the pancreatic parenchyma (necrosis = no blood supply = no contrast uptake). Three types exist:
- (A) Combined intrapancreatic + extrapancreatic necrosis (most common, 75-80%)
- (B & C) Extrapancreatic fat necrosis alone (arrows) - appears as mass-like hypodense areas (unlike simple stranding in oedema)
- (D) Intrapancreatic hypoenhancing necrosis alone (arrow) - minimal peripancreatic involvement
- (E) Necrosis in the swollen tail only
5. Walled-Off Necrosis (WON) - Evolution Over 4 Weeks
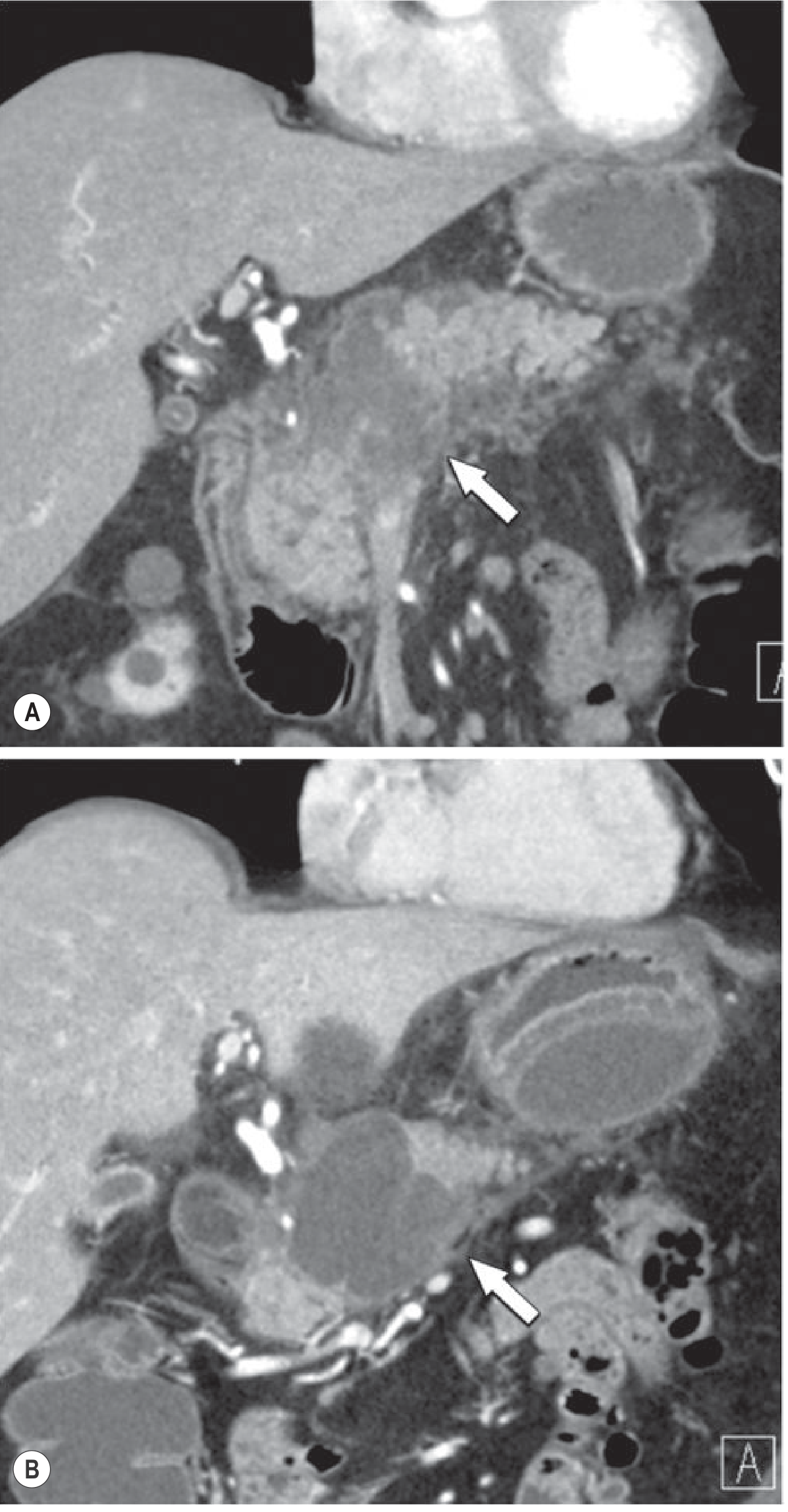
Fig. 25.15 - Development of Walled-Off Necrosis:
- Panel A: Early phase - Acute Necrotic Collection (ANC) involving pancreatic head and body (arrow) - heterogeneous, no wall
- Panel B: Follow-up at 4 weeks - evolution into a well-defined WON (arrow) containing fat-density debris inside. Note the thick wall that has now formed.
6. Infected WON - CT + Ultrasound Correlation
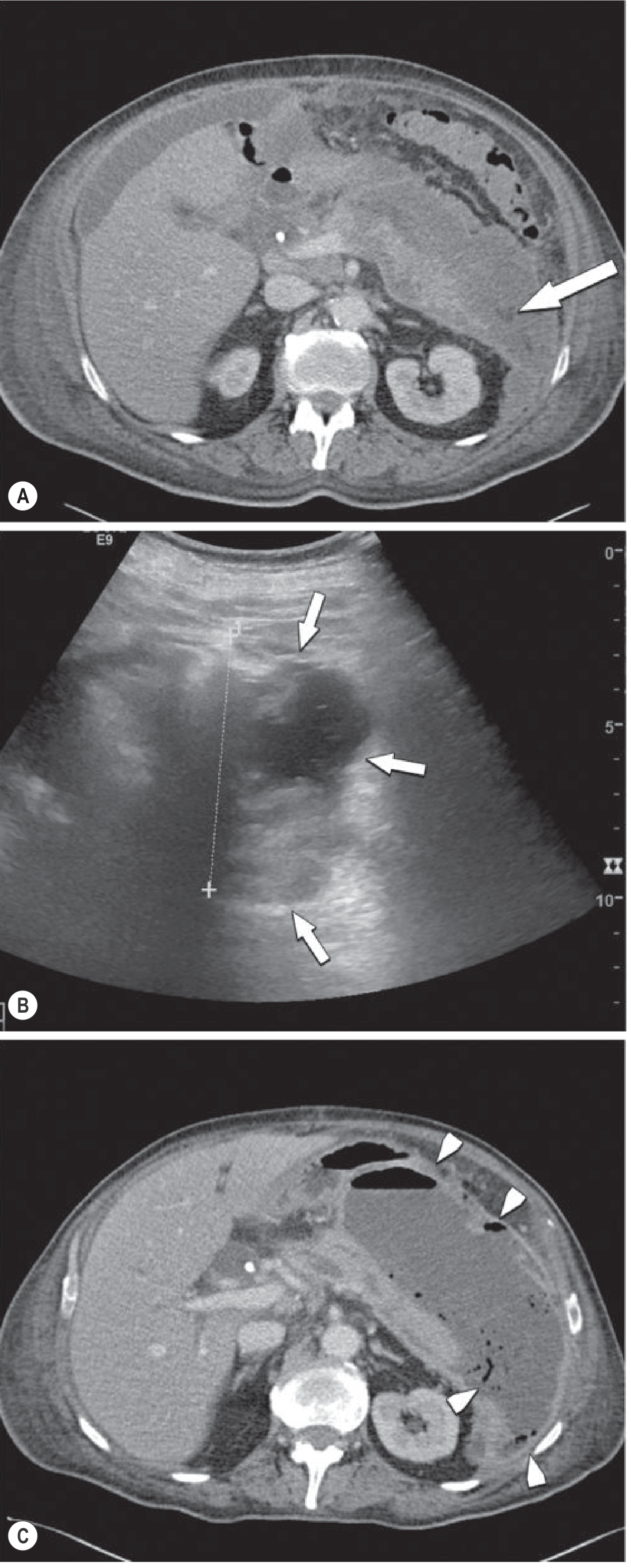
Fig. 25.16 - Infected Walled-Off Necrosis:
- Panel A (CT): Heterogeneous pancreatic parenchyma with hypoenhancing spotty necrosis + extrapancreatic ANC with fat necrosis chunks (arrow)
- Panel B (US): Collection with mixed fluid and solid material - cannot be mistaken for a simple pseudocyst (arrows)
- Panel C (follow-up CT at 6 weeks): Gas-fluid level (arrow) and gas bubbles (arrowheads) - pathognomonic of superinfection (infected necrosis). This carries ~80% of all mortality from acute pancreatitis.
Summary: CT Patterns at a Glance
| CT Finding | Diagnosis | Timing |
|---|---|---|
| Gland swelling + peripancreatic fat stranding | Mild oedematous AP | Early |
| AFPC (fluid collection, no wall) | Moderate-severe oedematous AP | <4 weeks |
| Pseudocyst (fluid + wall, no debris) | Complication of oedematous AP | >4 weeks |
| Non-enhancing parenchyma | Necrotising pancreatitis (ANC) | Early |
| Thick-walled collection + debris | Walled-off necrosis (WON) | >4 weeks |
| Gas bubbles/gas-fluid level in collection | Infected necrosis (surgical emergency) | Late |
CT Severity Index (CTSI): Scores 0-10 combining degree of pancreatic inflammation (0-4 pts), necrosis (0-4 pts), and extrapancreatic complications (2 pts). Scores 8-10 = severe disease with ~50% organ failure rate.
Source: Grainger & Allison's Diagnostic Radiology, Chapter 25 - Pancreatic Imaging
This is a shared conversation. Sign in to Orris to start your own chat.