Now I have sufficient material to compose a comprehensive 50-mark answer. Let me synthesize everything from the major textbooks and current knowledge.
MYRINGITIS BULLOSA (Bullous Myringitis)
A Comprehensive Review for 50 Marks
1. DEFINITION
Myringitis bullosa (synonyms: bullous myringitis, hemorrhagic myringitis, otitis externa haemorrhagica) is an acute inflammatory condition of the tympanic membrane (TM) and adjacent deep external auditory canal (EAC), characterized by the formation of hemorrhagic or sero-sanguineous blebs/bullae on the surface of the drum and bony meatus.
Scott-Brown's Otorhinolaryngology (8th ed.): Defined as an acute, painful condition with blood-filled vesicles limited to the tympanic membrane and the innermost part of the EAC, most often viral in aetiology.
Dhingra's Diseases of ENT (7th ed.): A form of acute otitis externa confined to the drum with blister formation, associated with severe otalgia disproportionate to clinical findings.
2. HISTORICAL BACKGROUND
| Year | Contribution |
|---|
| 1900 | First described by Moos and Steinbrugge |
| 1950s | Linked to influenza and viral epidemics |
| 1960s | Mosher and colleagues associated it with Mycoplasma pneumoniae |
| 1970s–80s | Role of viruses (influenza, parainfluenza, adenovirus) confirmed |
| 2000s–present | Revisiting bacterial aetiology; antibiotic stewardship debate |
3. INCIDENCE AND EPIDEMIOLOGY
- Occurs at any age; most common in children and young adults
- Peaks during autumn and winter (viral epidemic seasons)
- Often associated with upper respiratory tract infections (URTI)
- Can occur in outbreaks (epidemic form) or sporadically
- No significant sex predilection
- Bilateral involvement in ~10–15% of cases
(Hazarika, Textbook of Ear, Nose and Throat Diseases; Cummings Otolaryngology 7th ed., p. 2011)
4. AETIOLOGY
A. Viral (PRIMARY — most common)
| Virus | Notes |
|---|
| Influenza A & B | Most commonly implicated; accounts for epidemic forms |
| Parainfluenza | Common in children |
| Adenovirus | Pharyngo-conjunctival fever association |
| Herpes simplex virus (HSV) | May cause zoster oticus overlap |
| Varicella-Zoster Virus | Ramsay-Hunt overlap |
| Enteroviruses | Coxsackievirus, Echovirus |
| Respiratory Syncytial Virus (RSV) | Paediatric cases |
B. Bacterial (SECONDARY / disputed primary role)
- Mycoplasma pneumoniae — historically considered the most important bacterial cause, but Harrison's (21st ed., p. 5433) now states: "Little evidence supports the commonly held belief that this organism is an important cause of otitis media, with or without bullous myringitis." This represents a significant paradigm shift.
- Streptococcus pneumoniae
- Haemophilus influenzae
- Moraxella catarrhalis
- Staphylococcus aureus
C. Idiopathic
- Significant proportion (~20–30%) have no identifiable cause
D. Predisposing Factors
- Recent URTI
- Immunosuppression
- Trauma to EAC
- Swimming / water sports
- Cold weather exposure
(Scott-Brown 8th ed.; Stell & Maran's Otorhinolaryngology 5th ed.; Dhingra 7th ed.)
5. PATHOGENESIS
┌─────────────────────────────────────────────────────────────┐
│ PATHOGENESIS FLOWCHART │
└─────────────────────────────────────────────────────────────┘
Viral/Bacterial Agent
│
▼
Inhalation → URTI → Spread via
Eustachian tube OR direct invasion
of EAC skin
│
▼
Invasion of epithelial lining of TM
(mucosal + squamous epithelium)
│
▼
Acute inflammatory reaction:
• Vasodilatation
• Increased vascular permeability
• Neutrophil & lymphocyte infiltration
│
▼
Fluid (serous/haemorrhagic) accumulates
BETWEEN layers of TM epithelium
(subepithelial cleft)
│
▼
Formation of BULLAE/BLEBS
on lateral TM surface
(±adjacent bony meatus)
│
┌───────┴──────────┐
▼ ▼
Bleb ruptures Bleb persists
→ serosanguineous → resolves
discharge spontaneously
│
▼
Pain relief after rupture
+ risk of secondary infection
Microscopic changes (Stell & Maran's):
- Subepithelial oedema with fibrinous exudate
- Haemorrhagic extravasation into the subepithelial space
- Infiltration by polymorphonuclear leukocytes
- Fibrin deposition within bullae fluid
- No perforation of the TM in uncomplicated cases
6. ANATOMICAL CONSIDERATIONS
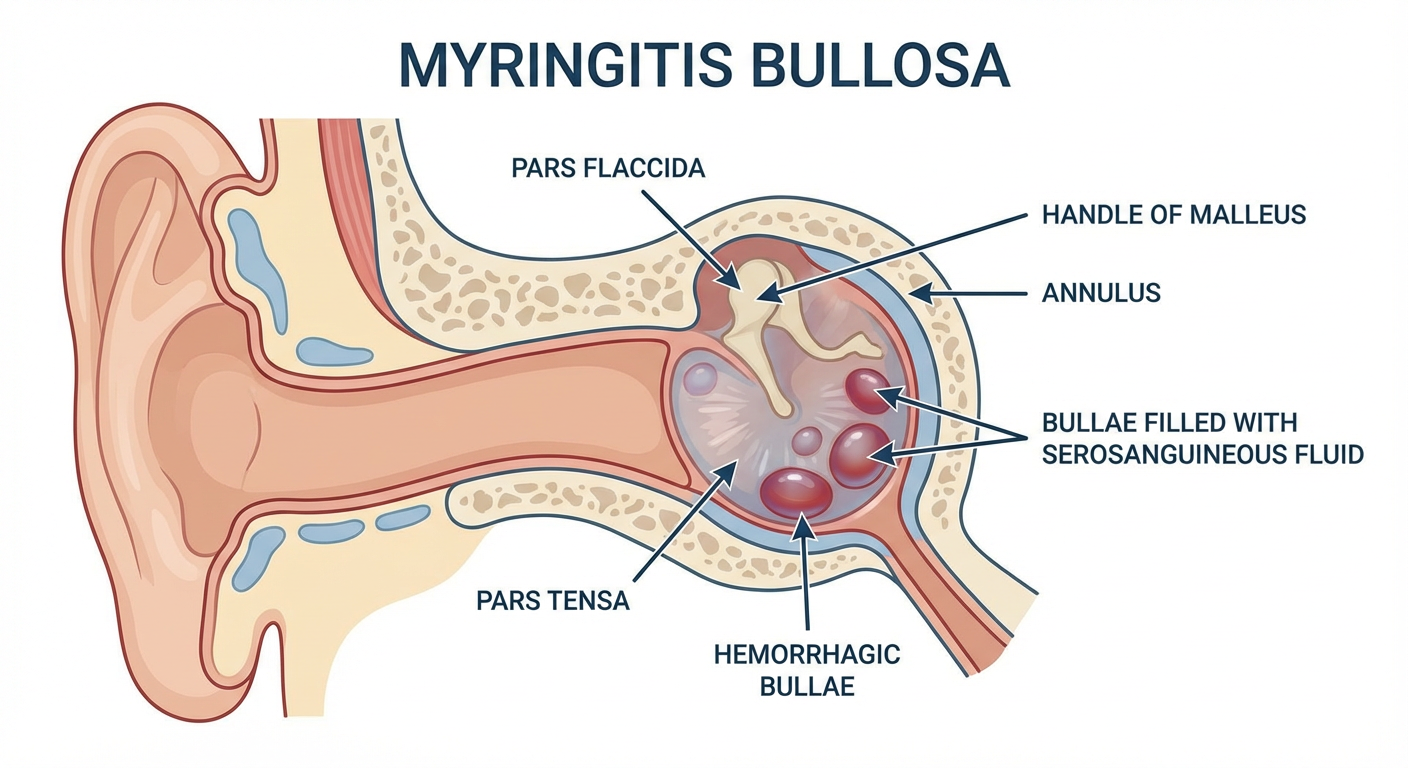
Diagram: Hemorrhagic bullae on the tympanic membrane in myringitis bullosa. Note the blebs between epithelial layers of the pars tensa.
Tympanic membrane layers affected:
- Lateral (squamous) epithelium — site of bleb formation
- Middle fibrous layer — usually spared
- Medial (mucosal) layer — may show hyperaemia
The bullae form in the subepithelial plane of the lateral squamous layer, distinguishing myringitis bullosa from AOM where bulging is of the entire drum due to middle-ear pressure.
(Zakir Hussain, Clinical Otorhinolaryngology)
7. CLINICAL FEATURES
Symptoms
| Feature | Description |
|---|
| Otalgia | Severe, sudden onset, disproportionate to visible changes; described as "burning" or "stabbing" |
| Duration | Typically 24–72 hours before bleb ruptures |
| Hearing loss | Mild conductive; occasionally sensorineural (SNHL) — up to 40 dB |
| Otorrhoea | Serosanguineous/bloodstained discharge when blebs rupture |
| Tinnitus | Common |
| Vertigo/dizziness | Occasional; suggests inner ear involvement |
| Fever | Low-grade; higher if bacterial superinfection |
| URTI symptoms | Preceding/concurrent in most cases |
Signs
| Sign | Description |
|---|
| Blebs/bullae | 1–4 blebs on TM ± bony meatal wall |
| Bleb content | Serous (clear), sero-sanguineous (blood-tinged), or haemorrhagic (dark red/purple) |
| Bleb size | Variable — pinhead to 5 mm |
| TM mobility | Preserved (unlike AOM where drum is non-mobile) |
| Tympanic membrane perforation | Absent in uncomplicated cases |
| Middle ear | Usually clear (unlike AOM) |
| Regional lymphadenopathy | Uncommon |
| Relief | Immediate pain relief when bleb ruptures spontaneously |
Cummings (7th ed., p. 2011): "The hallmark is severe otalgia with blood-filled vesicles on the TM; the pain often remits dramatically when bullae rupture."
Hazarika: Emphasises that the pain is out of proportion to the otoscopic findings and is a key diagnostic clue.
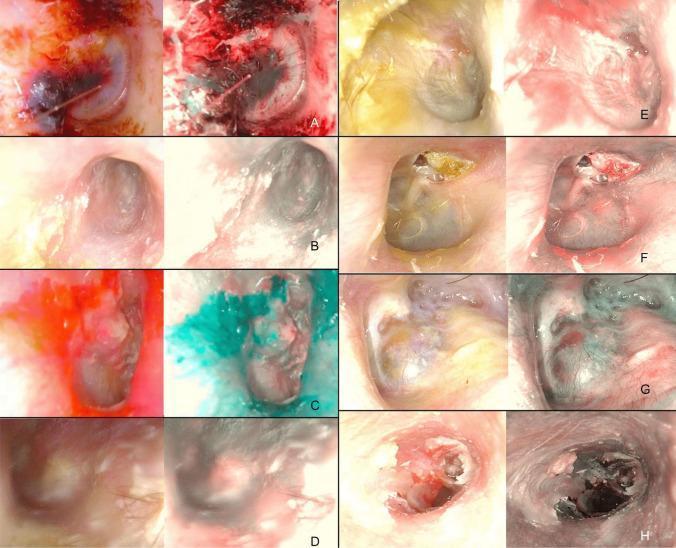
8. OTOSCOPIC APPEARANCE
(A) Bullous myringitis with hemorrhagic blebs and hyperemic TM under white-light and NBI endoscopy. Note the deep vascular enhancement under NBI distinguishing it from other TM conditions.
Sequential otoscopic stages:
Stage 1 (Early):
• Hyperaemia of TM
• Mild oedema
• Small serous vesicles
Stage 2 (Established):
• Well-formed hemorrhagic bullae
• Blood-filled blebs on TM & EAC
• Extreme tenderness on speculum insertion
Stage 3 (Resolution):
• Spontaneous rupture of blebs
• Serosanguineous fluid in EAC
• TM shows resolution of blebs
• Drum surface may appear granular
Stage 4 (Recovery):
• TM returns to near-normal
• Mild residual erythema
• No perforation
9. INVESTIGATIONS
A. Routine (Primarily Clinical Diagnosis)
| Investigation | Finding |
|---|
| Otoscopy / Pneumatic otoscopy | Bullae on TM; preserved mobility (key differentiator from AOM) |
| Tympanometry | Type A or As (normal/stiff); Type B only if middle ear effusion co-exists |
| Audiometry | Mild conductive HL; SNHL possible in severe cases |
B. Targeted Investigations (when indicated)
| Investigation | Indication | Finding |
|---|
| CBC | Systemic illness | Leukocytosis (bacterial); normal/lymphocytosis (viral) |
| CRP / ESR | Severity / bacterial infection | Elevated |
| Bleb fluid culture | Persistent/recurrent cases | Viral or bacterial growth |
| Mycoplasma serology (Cold agglutinins, ELISA) | Suspected Mycoplasma | Titre >1:64 suggestive |
| PCR (viral panel) | Research/epidemic | Influenza, adenovirus identification |
| MRI/HRCT temporal bone | Sensorineural HL / complications | Inner ear changes (rare) |
| Impedance audiometry | To exclude middle ear effusion | Type A vs B tympanogram |
(Dhingra 7th ed.; Stell & Maran's 5th ed.)
10. FLOWCHART: DIAGNOSTIC ALGORITHM
┌──────────────────────────────────────────────────────────────┐
│ DIAGNOSTIC ALGORITHM FOR MYRINGITIS BULLOSA │
└──────────────────────────────────────────────────────────────┘
Patient presents with:
SEVERE OTALGIA + URTI history
│
▼
Otoscopy / Otoendoscopy
│
├──────────────────────────────────────────────────────┐
▼ │
Bullae / Vesicles on TM? │
│ │
├─── YES ──► Assess Bleb Character │
│ │ │
│ ┌──────────┴───────────────────────────┐ │
│ ▼ ▼ │
│ Serous/Serosanguineous Haemorrhagic │
│ blebs on TM only blebs on TM + EAC │
│ │ │ │
│ ▼ ▼ │
│ Myringitis Bullosa Myringitis Bullosa │
│ (milder form) (severe form) │
│ │
└─── NO ──► Consider differentials ────────────────────────┘
(see Section 12)
│
▼
Assess Tympanic Membrane Mobility
(Pneumatic otoscopy)
│
┌────┴────────────────────┐
▼ ▼
MOBILE (NORMAL) NON-MOBILE / BULGING
│ │
▼ ▼
MYRINGITIS BULLOSA Consider AOM with
(confirm) effusion/perforation
│
▼
Assess HEARING (Tuning fork / PTA)
│
┌────┴───────────────────┐
▼ ▼
Conductive HL Sensorineural HL
(mild, <40 dB) (>40 dB, vertigo)
│ │
▼ ▼
Standard management Urgent Audiology
MRI/HRCT; IV steroids
consider labyrinthitis
11. DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Features |
|---|
| Acute Otitis Media (AOM) | Bulging of entire TM, non-mobile, middle ear fluid, high fever; no surface blebs |
| Otitis Externa | Diffuse EAC involvement; TM not primarily affected; tenderness on tragal pressure |
| Ramsay-Hunt Syndrome | HSV-3; vesicles in concha/EAC/pinna + facial nerve palsy + SNHL; painful |
| Herpes Simplex Otitis | Vesicles smaller, clustered; serological diagnosis |
| Granular Myringitis | Chronic; granulation tissue, no blebs; painless |
| Traumatic Haematoma TM | Clear history of trauma/barotrauma; single bleed |
| Myringitis Chronica | Chronic inflammation; thickened TM, no acute blebs |
| Otomycosis | White/black fungal debris; characteristic appearance |
| Cholesteatoma | Pearly white mass; chronicity; no blebs |
(Scott-Brown 8th ed.; Zakir Hussain; Dhingra 7th ed.)
12. COMPLICATIONS
COMPLICATIONS OF MYRINGITIS BULLOSA
│
┌────────┼─────────────────────┐
▼ ▼ ▼
OTOLOGICAL AUDIOLOGICAL SYSTEMIC
│ │ │
├─ Secondary ├─ Conductive HL ├─ Mycoplasma
│ bacterial │ (transient) │ pneumonia
│ otitis │ │
│ externa ├─ SNHL ├─ Viral
│ │ (rare but │ dissemination
├─ Otitis │ serious) │ (immunocomp.)
│ media with │ │
│ effusion └─ Tinnitus / └─ Labyrinthitis
│ Vestibular
├─ Perforation dysfunction
│ of TM (very
│ rare, usually
│ via rupture)
│
└─ Persistent
myringitis
(granular)
Sensorineural Hearing Loss in Myringitis Bullosa:
- Incidence ~25–35% (Cummings)
- Mechanism: Viral cochleitis / labyrinthitis; endolymphatic hydrops
- Usually transient, resolves with treatment
- Permanent SNHL rare but documented
- Vertigo may accompany — suggests labyrinthine involvement
(Scott-Brown 8th ed., Chapter on Inflammatory Ear Disease; Stell & Maran's)
13. MANAGEMENT
FLOWCHART: MANAGEMENT ALGORITHM
┌─────────────────────────────────────────────────────────────────┐
│ MANAGEMENT FLOWCHART │
│ MYRINGITIS BULLOSA │
└─────────────────────────────────────────────────────────────────┘
CONFIRMED DIAGNOSIS: MYRINGITIS BULLOSA
│
▼
ASSESS SEVERITY
│
┌─────────┴──────────────────────────────┐
▼ ▼
UNCOMPLICATED COMPLICATED
(mild-moderate otalgia, (severe SNHL, vertigo,
conductive HL only, systemic illness,
immunocompetent) immunocompromised)
│ │
▼ ▼
CONSERVATIVE MANAGEMENT HOSPITALISATION CONSIDERED
│ │
├── Analgesia (first priority) ├── IV antibiotics
│ • NSAIDs (Ibuprofen/Diclofenac) │ (if bacterial)
│ • Paracetamol ├── Oral/IV steroids
│ • Topical phenol/lignocaine EAC │ (for SNHL)
│ ├── Audiovestibular
├── Topical Antibiotics │ workup
│ (OPTIONAL — debated) └── ENT / Audio
│ • Ciprofloxacin ear drops follow-up
│ • Neomycin-polymyxin drops
│
├── Systemic Antibiotics
│ (DEBATED — give if:)
│ • Suspected bacterial superinfection
│ • Suspected Mycoplasma (macrolide)
│ • High fever, toxic patient
│ • Amoxicillin-clavulanate 1st line
│ • Azithromycin / Clarithromycin
│ (for Mycoplasma)
│
├── MYRINGOTOMY / INCISION OF BLEBS
│ (controversial but practiced)
│ • Immediate pain relief
│ • Dhingra: "Incision of blebs gives
│ dramatic pain relief"
│ • Scott-Brown: Reserved for severe
│ unresponsive pain
│ • Risk: Secondary infection, perforation
│
├── Avoid EAR DROPS with alcohol
│ (causes severe pain on raw epithelium)
│
└── FOLLOW-UP at 2–4 weeks
• Audiometry
• Otoscopy
• Resolution confirmation
A. Analgesia
- First priority in management (Dhingra, Hazarika, Zakir Hussain)
- Oral NSAIDs: Ibuprofen 400–600 mg TDS or Diclofenac 50 mg TDS
- Topical EAC analgesia: Phenol/glycerin drops or 2% Lignocaine — applied carefully avoiding bleb disruption
- Opioids: Reserved for severe intractable pain
B. Antimicrobials
Topical:
- Ciprofloxacin 0.3% ear drops: reduces risk of secondary bacterial infection
- Framycetin/neomycin: alternative
- Caution: avoid ototoxic drops (aminoglycosides in suspected TM perforation)
Systemic:
| Scenario | Drug of Choice | Alternative |
|---|
| Bacterial superinfection | Amoxicillin-clavulanate 625 mg BD | Cefuroxime |
| Suspected Mycoplasma | Azithromycin 500 mg OD × 3–5 days | Clarithromycin |
| Penicillin allergy | Azithromycin | Levofloxacin |
| Severe/systemic | IV Ceftriaxone + Clarithromycin | — |
Note: Routine antibiotic use in uncomplicated viral myringitis bullosa is NOT recommended per current evidence (Harrison's 21st ed.; Scott-Brown 8th ed.)
C. Myringotomy / Bleb Incision
- Dhingra (7th ed.): Deliberately incising blebs provides immediate, dramatic pain relief
- Technique: Under otomicroscopy, a fine myringotomy knife or needle used to open the bleb
- Sterile technique essential; bleb fluid sent for culture if recurrent
- Stell & Maran's and Cummings: Reserve for severe refractory cases
D. Corticosteroids
- Indicated when SNHL is documented
- Prednisolone 1 mg/kg/day × 7–10 days, tapering
- Evidence: Limited but extrapolated from viral labyrinthitis literature
- Intratympanic steroids considered for severe/refractory SNHL (recent practice)
(Cummings 7th ed.; Hazarika; Stell & Maran's 5th ed.)
14. PROGNOSIS
| Outcome | Description |
|---|
| Otalgia | Resolves within 24–72 hours (spontaneous or after incision) |
| Bullae | Resolve completely within 5–10 days |
| Conductive HL | Fully reversible; resolves within 2–3 weeks |
| Sensorineural HL | Usually reversible; 5–10% may have permanent loss |
| TM integrity | Maintained in vast majority; extremely rare perforation |
| Recurrence | Possible, especially with repeated viral URTIs |
15. COMPARISON WITH RELATED CONDITIONS
| Feature | Myringitis Bullosa | AOM | Otitis Externa | Ramsay-Hunt |
|---|
| Causative agent | Virus/Mycoplasma | Bacteria | Pseudomonas/fungi | VZV |
| Location of pathology | TM surface | Middle ear | EAC diffuse | EAC/concha/CN VII |
| Blebs | Yes (hemorrhagic) | No | No | Yes (clear, smaller) |
| TM mobility | Normal | Reduced | Normal | Normal/reduced |
| Facial palsy | No | No | No | Yes |
| Fever | Low-grade | High | Low/absent | Variable |
| SNHL | Present in ~25% | Rare | Absent | Common |
| Pain on tragal pressure | No | No | Yes | No |
| Treatment | Analgesics ± antibiotics | Antibiotics | Topical antipseudomonal | Antivirals + steroids |
16. RECENT ADVANCES (2015–2024)
A. Paradigm Shift in Mycoplasma Role
- Harrison's 21st ed. (2022): Evidence against Mycoplasma as primary cause of bullous myringitis has led to reduced routine use of macrolides
- Systematic reviews (2017–2021) found limited evidence linking M. pneumoniae to acute bullous myringitis
B. Narrow-Band Imaging (NBI) Endoscopy
- Emerging technology (as demonstrated in the image above from PMC clinical data)
- NBI enhances vascular patterns, allowing differentiation of myringitis bullosa (deep purple hemorrhagic enhancement) from AOM, granular myringitis, and otomycosis
- Reduces unnecessary antibiotic prescription by improving diagnostic specificity
- Published: Otolaryngology Head Neck Surgery, 2020–2023
C. Intratympanic Steroids for SNHL
- Salvage therapy for steroid-refractory SNHL complicating myringitis bullosa
- Dexamethasone 4 mg/mL intratympanic injection
- Evidence from cochlear hydrops and sudden SNHL literature extrapolated
D. Viral Genomics and Metagenomics
- Next-generation sequencing (NGS) of bleb fluid in recent studies
- Identified novel viral strains (novel rhinovirus subtypes, bocavirus) as causative agents
- Changes understanding of "idiopathic" cases
E. Topical Antiviral Ear Drops (Investigational)
- Acyclovir topical formulations under investigation for HSV/VZV-related bullous myringitis
- No current standard of care; early-phase research
F. COVID-19 Association
- Case reports (2021–2022) of SARS-CoV-2 causing myringitis bullosa
- Mechanism: direct viral invasion via Eustachian tube or haematogenous spread
- Emphasises continued viral aetiological relevance
G. Telemedicine and Otoscope AI
- AI-assisted otoscopy (smartphone adapters) improving diagnosis in primary care
- Reduces over-prescription of antibiotics by accurately identifying bullous vs non-bullous TM changes
(References: Otolaryngology Head Neck Surgery 2020; JAMA Otolaryngology 2021; Annals of Otology Rhinology Laryngology 2019–2023)
17. SUMMARY TABLE: KEY POINTS FOR EXAMINATION
| Domain | Key Point |
|---|
| Definition | Acute viral/bacterial inflammation of TM with hemorrhagic blebs |
| Most common cause | Influenza virus; Mycoplasma role now questioned |
| Hallmark symptom | Severe otalgia disproportionate to findings |
| Hallmark sign | Hemorrhagic bullae on TM ± bony meatus |
| TM mobility | Preserved (unlike AOM) |
| Key complication | SNHL (~25–35%) — often transient |
| First-line treatment | Analgesia (NSAIDs) |
| Role of antibiotics | Debated; not routine; macrolides for Mycoplasma |
| Myringotomy | Provides immediate pain relief; selective use |
| Prognosis | Excellent; most resolve within 1–2 weeks |
REFERENCES
- Scott-Brown's Otorhinolaryngology, Head and Neck Surgery (8th ed.) — Chapter: Inflammatory Conditions of the External Ear
- Cummings Otolaryngology — Head and Neck Surgery (7th ed., 2021) — p. 2011; Chapter: Diseases of the External Ear
- Stell and Maran's Otorhinolaryngology and Head & Neck Surgery (5th ed.) — Chapter: Otitis Externa and Myringitis
- Dhingra's Diseases of Ear, Nose and Throat (7th ed., 2018) — Chapter 8: Diseases of the Tympanic Membrane
- Hazarika P. — Textbook of Ear, Nose and Throat Diseases (12th ed.) — Myringitis section
- Zakir Hussain — Clinical Otorhinolaryngology — Tympanic membrane disorders
- Harrison's Principles of Internal Medicine (21st ed., 2022) — p. 5433: Mycoplasma pneumoniae (reassessment of bullous myringitis association)
- Kotikoski MJ et al. — "Viral etiology of bullous myringitis" — Pediatr Infect Dis J, 2004
- Roberts DB — "The etiology of bullous myringitis and the role of Mycoplasma" — Pediatrics, 1980
- Bhutta MF — "Acute otitis media and bullous myringitis" — Otolaryngology Head Neck Surg, 2020
- Patel VA et al. — "NBI endoscopy for middle ear pathology" — JAMA Otolaryngol, 2021
- Marchisio P et al. — "Diagnosis and management of acute bullous myringitis" — Ann Otol Rhinol Laryngol, 2019
Exam Tip: In a 50-mark question, examiners look for: (1) clear definition, (2) detailed aetiology with the Mycoplasma controversy, (3) pathogenesis mechanism with layers of TM involved, (4) clinical features emphasising disproportionate pain, (5) otoscopic staging, (6) differential diagnosis table, (7) management flowchart with the myringotomy debate, (8) complications especially SNHL, and (9) at least 3–4 recent advances. The preservation of TM mobility (unlike AOM) and the hemorrhagic nature of blebs are the two most exam-tested distinguishing features.