Syphilis
Reading File
search_medical_text
syphilis stages clinical presentation diagnosis treatment
search_medical_text
syphilis serology RPR VDRL FTA-ABS treponemal testing
search_medical_image
syphilis chancre rash secondary syphilis skin lesions
GradeResponse
GradeResponse
GradeResponse
Syphilis
Etiology: Caused by Treponema pallidum subspecies pallidum, a spirochete bacterium. Transmitted primarily via sexual contact (direct mucosal/skin contact with active lesions), vertically (congenital syphilis), or rarely via blood transfusion.
Stages & Clinical Presentation
Primary Syphilis
- Incubation: 10–90 days (average ~3 weeks)
- Hallmark: Painless indurated chancre at the inoculation site (genitals, anus, oropharynx, lips)
- Regional lymphadenopathy (painless, firm)
- Heals spontaneously in 3–6 weeks even without treatment
Secondary Syphilis
- Develops 2–12 weeks after chancre appearance
- Diffuse maculopapular rash — classically involves palms and soles; non-pruritic
- Condylomata lata (moist, flat, warty lesions in moist areas)
- Mucous patches, alopecia, fever, malaise, lymphadenopathy, hepatosplenomegaly
- Resolves spontaneously → enters latent phase
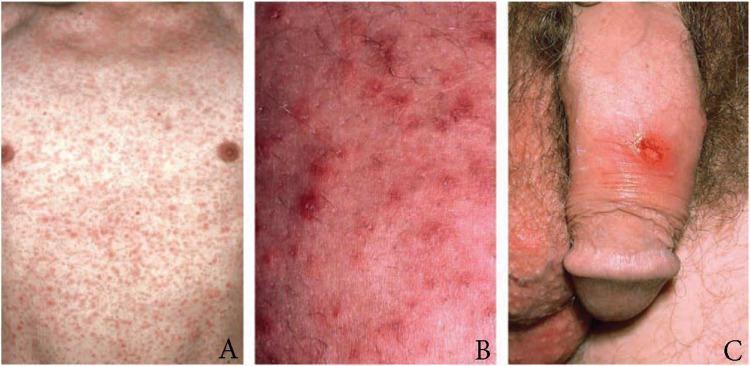
Panel A/B: Symmetric maculopapular rash of secondary syphilis. Panel C: Solitary indurated chancre on penile shaft (primary syphilis).
Latent Syphilis
- Early latent: Infection < 1 year, no symptoms
- Late latent: Infection ≥ 1 year (or unknown duration), no symptoms
- Still seroreactive; patient can transmit vertically
Tertiary Syphilis
- Occurs years to decades after untreated infection (~30% of untreated cases)
- Gummatous syphilis: Granulomatous lesions in skin, bone, liver
- Cardiovascular syphilis: Aortitis, aortic aneurysm (ascending), aortic regurgitation
- Neurosyphilis: Can occur at any stage; manifestations include meningitis (early), tabes dorsalis, general paresis, Argyll Robertson pupil (accommodates but does not react to light)
Diagnosis
Serological Testing (Two-Step Algorithm)
| Test Type | Tests | Role |
|---|---|---|
| Non-treponemal (lipoidal antigen) | RPR, VDRL | Screening; titers reflect disease activity and treatment response |
| Treponemal | FTA-ABS, TPPA, EIA/CIA | Confirmatory; remain positive for life even after treatment |
Traditional algorithm: Non-treponemal screen → if reactive, confirm with treponemal test
Reverse algorithm (now common): Treponemal EIA/CIA screen first → if reactive, confirm/stage with RPR
Reverse algorithm (now common): Treponemal EIA/CIA screen first → if reactive, confirm/stage with RPR
Key testing notes (Laboratory Recommendations for Syphilis Testing, p. 17):
- RPR and VDRL have similar sensitivity/specificity but titers are NOT interchangeable — use the same test type serially to monitor treatment response
- FTA-ABS sensitivity ~78% and TPPA sensitivity ~94.5% in primary syphilis — TPPA is preferred for primary-stage confirmation
- False positives with non-treponemal tests: pregnancy, autoimmune disease (SLE), viral infections, IV drug use
CSF Examination (Neurosyphilis)
Indicated when neurological/ocular/otologic symptoms present, treatment failure, or HIV with CD4 < 350 and RPR ≥ 1:32. CSF findings: lymphocytic pleocytosis, elevated protein, reactive CSF-VDRL (specific but insensitive).
Dark-field Microscopy / Direct Detection
Direct visualization of spirochetes from chancre exudate or condylomata lata — useful in primary syphilis before seroreactivity develops. PCR-based assays also available.
Treatment
Per CDC STI Treatment Guidelines 2021 (Laboratory Recommendations for Syphilis Testing, p. 7):
| Stage | First-Line | Alternative (PCN allergy) |
|---|---|---|
| Primary, Secondary, Early Latent | Benzathine penicillin G 2.4 million units IM × 1 dose | Doxycycline 100 mg PO BID × 14 days |
| Late Latent / Latent Unknown Duration | Benzathine penicillin G 2.4 MU IM weekly × 3 doses | Doxycycline 100 mg PO BID × 28 days |
| Tertiary (gumma/cardiovascular) | Benzathine penicillin G 2.4 MU IM weekly × 3 doses | Consult ID specialist |
| Neurosyphilis | Aqueous crystalline penicillin G 18–24 MU IV/day × 10–14 days | Procaine PCN G + probenecid; or ceftriaxone 2g IV/IM × 10–14 days |
Penicillin allergy: Desensitization is recommended in pregnancy — no proven alternatives exist for congenital syphilis prevention.
Jarisch-Herxheimer Reaction
Febrile reaction occurring within 24 hours of first treatment dose (fever, rigors, hypotension, worsening rash). Managed with antipyretics; does NOT indicate treatment failure. Caution in pregnancy (can precipitate preterm labor).
Follow-up
- Non-treponemal titers should decline ≥4-fold (two dilutions) by 6–12 months in primary/secondary syphilis — treatment success
- Persistent titers or rising titers → re-infection or treatment failure → re-treat and consider CSF examination
Special Populations
Congenital Syphilis
- Transmitted transplacentally, any trimester (risk highest in secondary syphilis)
- Manifestations: stillbirth, hydrops fetalis, snuffles (bloody rhinorrhea), saddle-nose deformity, Hutchinson teeth, interstitial keratitis, saber shins, periostitis
- All pregnant women screened at first prenatal visit; repeat at 28 weeks and delivery in high-prevalence areas
- Treatment: Aqueous penicillin G IV × 10 days
HIV Co-infection
- Atypical presentations more common; may have higher rates of neurosyphilis
- Serological testing generally reliable; some false negatives possible at very low CD4 counts
- Standard regimens used, but close follow-up essential; lower threshold for LP
Complications Summary
| System | Complication |
|---|---|
| Neurological | Meningitis, stroke, general paresis, tabes dorsalis |
| Cardiovascular | Ascending aortitis, aortic aneurysm, aortic regurgitation |
| Ocular | Uveitis, optic neuritis, retinitis |
| Obstetric | Spontaneous abortion, stillbirth, congenital infection |
Key Takeaway: Syphilis is a multi-stage systemic infection with highly variable presentations ("the great imitator"). Diagnosis relies on a two-step serological algorithm, and benzathine penicillin G remains the cornerstone of treatment at all stages.
This is a shared conversation. Sign in to Orris to start your own chat.