St evelation in 2,3 and t inversion in avf
Reading File
search_medical_text
ST elevation leads II III inferior STEMI ECG diagnosis
search_medical_text
T wave inversion aVF inferior lead ECG significance
search_medical_image
inferior STEMI ECG ST elevation leads II III aVF
GradeResponse
GradeResponse
GradeResponse
ECG Pattern: ST Elevation in II, III + T-wave Inversion in aVF
This pattern localizes to the inferior wall and represents a spectrum from early/evolving infarction to post-ischemic change.
ECG Interpretation
| Feature | Significance |
|---|---|
| ST elevation in II and III | Inferior wall injury current (transmural ischemia) |
| T-wave inversion in aVF | Evolving or post-ischemic change in the inferior wall |
| aVF partially involved | aVF is the "average" inferior lead — T inversion without full ST elevation suggests it may be in a transitional phase |
The combination is characteristic of inferior STEMI (or evolving inferior MI). According to Harrison's Principles of Internal Medicine (p. 6804):
"Inferior wall ischemia produces changes in leads II, III, and aVF. When ischemic ST elevations occur as the earliest sign of acute infarction, they are typically followed within hours to days by evolving T-wave inversions and often Q waves in the same lead distribution."
The T-wave inversion in aVF while II and III still show ST elevation suggests aVF is in the repolarization phase of evolving infarction, or the injury is most pronounced in III > II (common with RCA occlusion).
Culprit Artery
- Right Coronary Artery (RCA) — most common (80–90% of inferior MIs)
- Clue: ST elevation higher in III than II → strongly favors RCA
- Also check right-sided leads (V3R, V4R) for right ventricular infarction
- Left Circumflex (LCx) — less common
- Clue: ST elevation higher in II than III, or lateral lead involvement (V5, V6, I, aVL)
Reciprocal Changes to Look For
| Lead | Expected finding |
|---|---|
| I, aVL | ST depression (reciprocal) — confirms inferior injury |
| V1–V3 | ST depression may indicate posterior extension |
| V4R | ST elevation → RV infarction (critical — avoid nitrates!) |
Illustrated Example
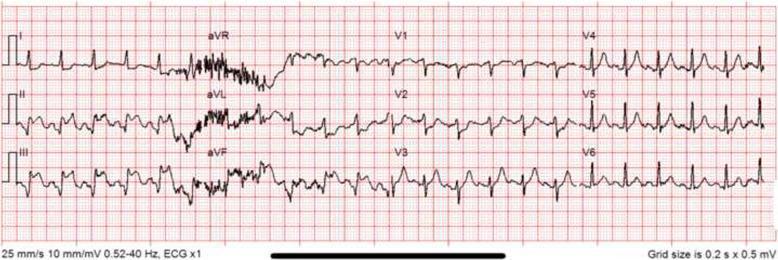
ST elevation in II, III, aVF with pathological Q-waves and reciprocal depressions in I and aVL — classic inferior STEMI pattern.
Immediate Management (Inferior STEMI)
- Activate cath lab — primary PCI is the goal (door-to-balloon <90 min)
- Aspirin 325 mg loading dose + P2Y12 inhibitor (ticagrelor 180 mg or clopidogrel 600 mg)
- Anticoagulation — unfractionated heparin or enoxaparin
- Check V4R — if RV infarct: aggressive IV fluids, avoid nitrates and diuretics
- Monitor for high-degree AV block (RCA supplies the AV node in ~90% of people)
Key Differentials
| Condition | How to distinguish |
|---|---|
| Pericarditis | ST elevation diffuse (not just inferior), saddle-shaped, no reciprocal changes |
| Early repolarization | ST elevation concave-up, no symptoms, no evolution |
| Takotsubo | Apical ballooning pattern, stress trigger, women > men |
| LVH strain | ST/T changes in hypertrophied leads, chronic pattern |
Bottom line: ST elevation in II and III with T-wave inversion in aVF = inferior STEMI until proven otherwise. Treat as STEMI, rule out RV involvement, and expedite reperfusion.
This is a shared conversation. Sign in to Orris to start your own chat.