Opthalmology
Asking for Preferences
Asking for Preferences
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"age-related macular degeneration"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Searching PubMed
"age-related macular degeneration" AND "anti-VEGF"
Reading File
Reading File
Loading Image
I now have comprehensive material from Goldman-Cecil, Wills Eye Manual, Robbins, and Histology textbooks, plus fundus photos and the pathology diagram. Let me compile the full deep-dive.
Age-Related Macular Degeneration (AMD) - Full Deep-Dive
1. Overview & Epidemiology
AMD is a neurodegenerative disease primarily affecting the retinal pigment epithelium (RPE) of the macula. It is the most common cause of irreversible central vision loss in the elderly in industrialized countries, accounting for ~8.5% of global blindness.
- Affects >1.75 million people in the United States
- Prevalence increases sharply after age 55; cumulative incidence in those >75 years is approximately 8%
- Both eyes are typically affected, though often asymmetrically
- Peripheral vision is spared - only central/macular function is lost
Sources: Goldman-Cecil Medicine; Robbins, Cotran & Kumar Pathologic Basis of Disease
2. Pathophysiology
The RPE-Bruch Membrane-Choriocapillaris Unit
The key structural unit in AMD pathogenesis is the triad of:
- Retinal Pigment Epithelium (RPE) - nourishes photoreceptors, phagocytoses spent outer segments
- Bruch's Membrane - basement membrane of the RPE
- Choriocapillaris - the innermost choroidal vasculature supplying oxygen/nutrients
Disturbance in any component of this unit leads to photoreceptor deterioration and vision loss.
Pathogenesis Diagram (Robbins)
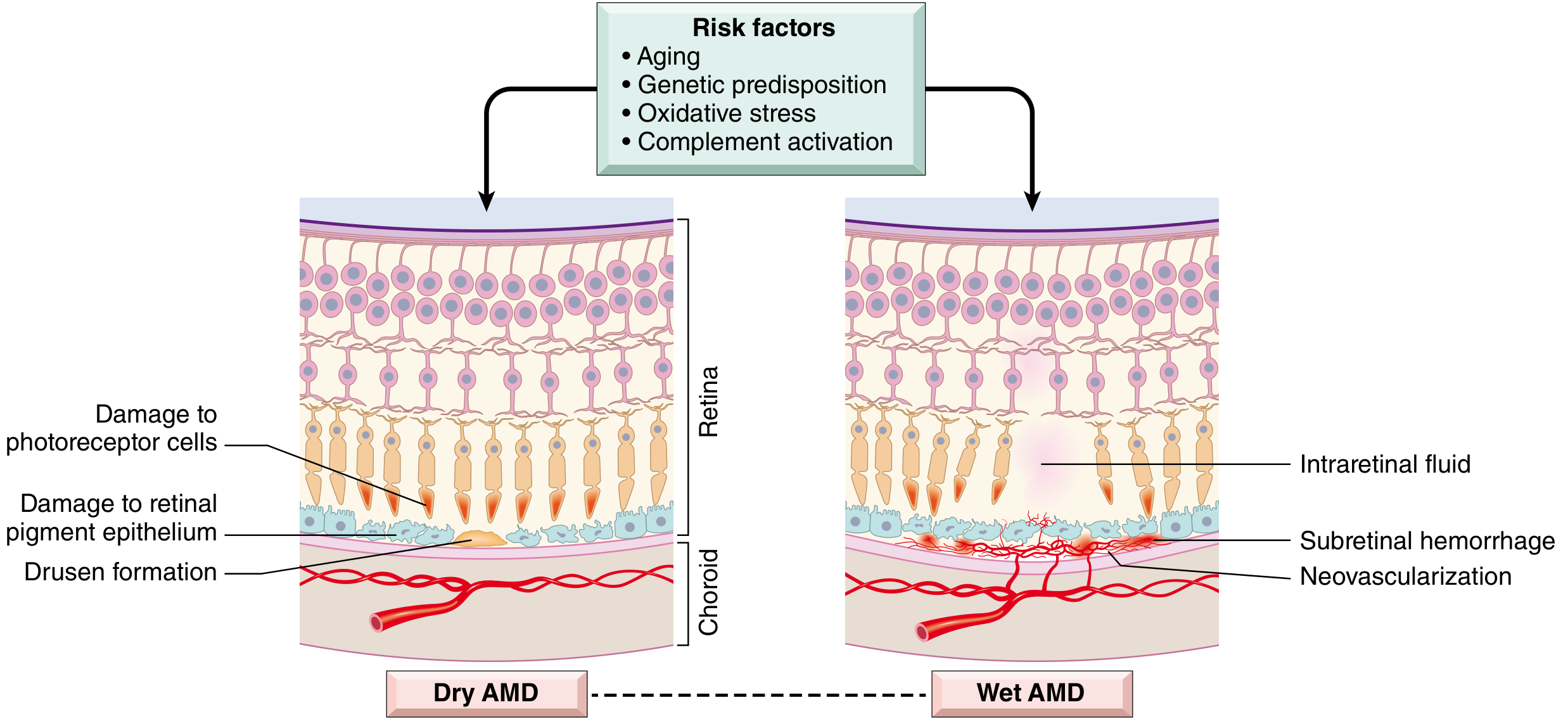
Risk factors drive both dry and wet AMD through complement activation, oxidative stress, and aging.
Dry (Atrophic) AMD
- Drusen form as focal thickenings/abnormal lipoprotein deposits within Bruch's membrane
- Lipofuscin (oxidation products of polyunsaturated fatty acids + vitamin A dimers) accumulates in stressed RPE cells
- Chronic complement system activation leads to RPE geographic atrophy and choriocapillaris loss
- Photoreceptors are secondarily lost overlying the atrophic RPE
Wet (Neovascular/Exudative) AMD
- Choroidal neovascularization (CNV): new vessels from the choriocapillaris penetrate through a breach in Bruch's membrane into the subretinal space
- These new vessels are fragile and leaky - they produce subretinal fluid (SRF), hemorrhage, and exudates
- VEGF (vascular endothelial growth factor) is the principal driver of neovascularization
- Blood may organize into a disciform scar (subretinal fibrosis), causing permanent photoreceptor loss
- Wet AMD is a complication of dry AMD, though both can coexist as parallel processes
Sources: Robbins Pathologic Basis of Disease; Histology - A Text and Atlas
3. Genetics & Risk Factors
Genetic
| Gene | Role |
|---|---|
| CFH (Complement Factor H) | Most strongly associated; abnormal CFH → unchecked complement activation |
| CFI (Complement Factor I) | Complement regulatory gene |
| Other complement regulatory genes | Polymorphisms increase risk |
Environmental & Lifestyle Risk Factors
| Factor | Notes |
|---|---|
| Smoking | Strongest modifiable risk factor; accelerates degeneration |
| Advanced age | Risk doubles each decade after 55 |
| Family history | Strong genetic component |
| Hyperopia | Associated risk |
| Blue eyes/fair skin | Increased susceptibility |
| Systemic hypertension | Vascular risk factor |
| High lipid levels | Accelerates disease |
| Uncontrolled blood sugar | Metabolic risk |
| UV exposure | Environmental oxidative stress |
Sources: Goldman-Cecil Medicine; Wills Eye Manual
4. Clinical Features
Dry AMD
Symptoms:
- Gradual, insidious loss of central vision (may be asymptomatic for years)
- Amsler grid distortion (metamorphopsia may appear as the disease progresses)
- Difficulty reading, recognizing faces
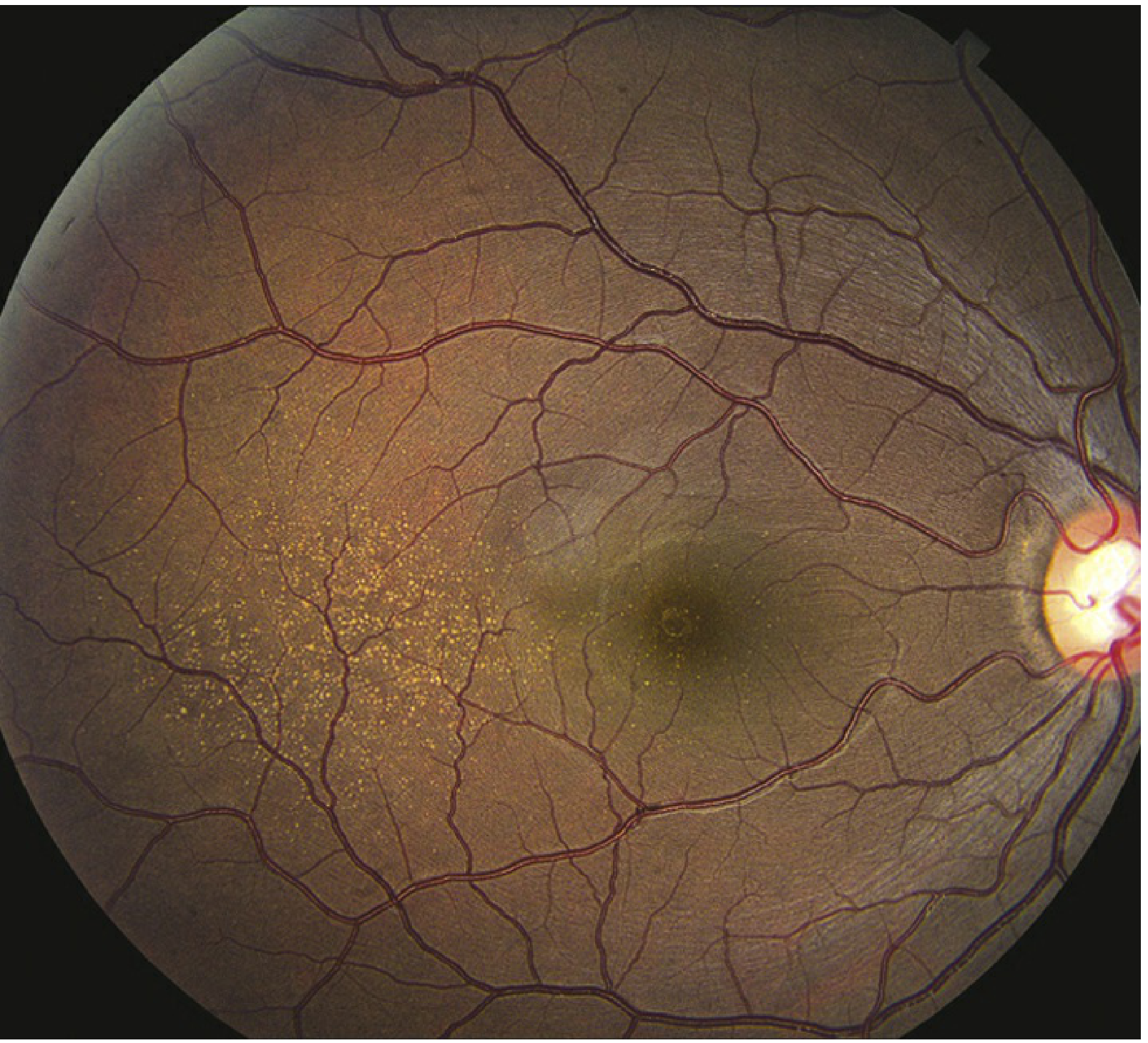
Fundus Signs:
- Drusen - soft drusen >60 µm are most significant (deep, hypopigmented spots)
- RPE mottling, depigmentation, hyperpigmentation clumps
- Geographic atrophy - well-defined areas of RPE and photoreceptor loss in advanced disease
Wet AMD
Symptoms:
- Sudden or rapid onset of central visual loss
- Central or paracentral scotoma (blind spot)
- Metamorphopsia (straight lines appear wavy) - hallmark symptom
- Photopsias in the central visual field
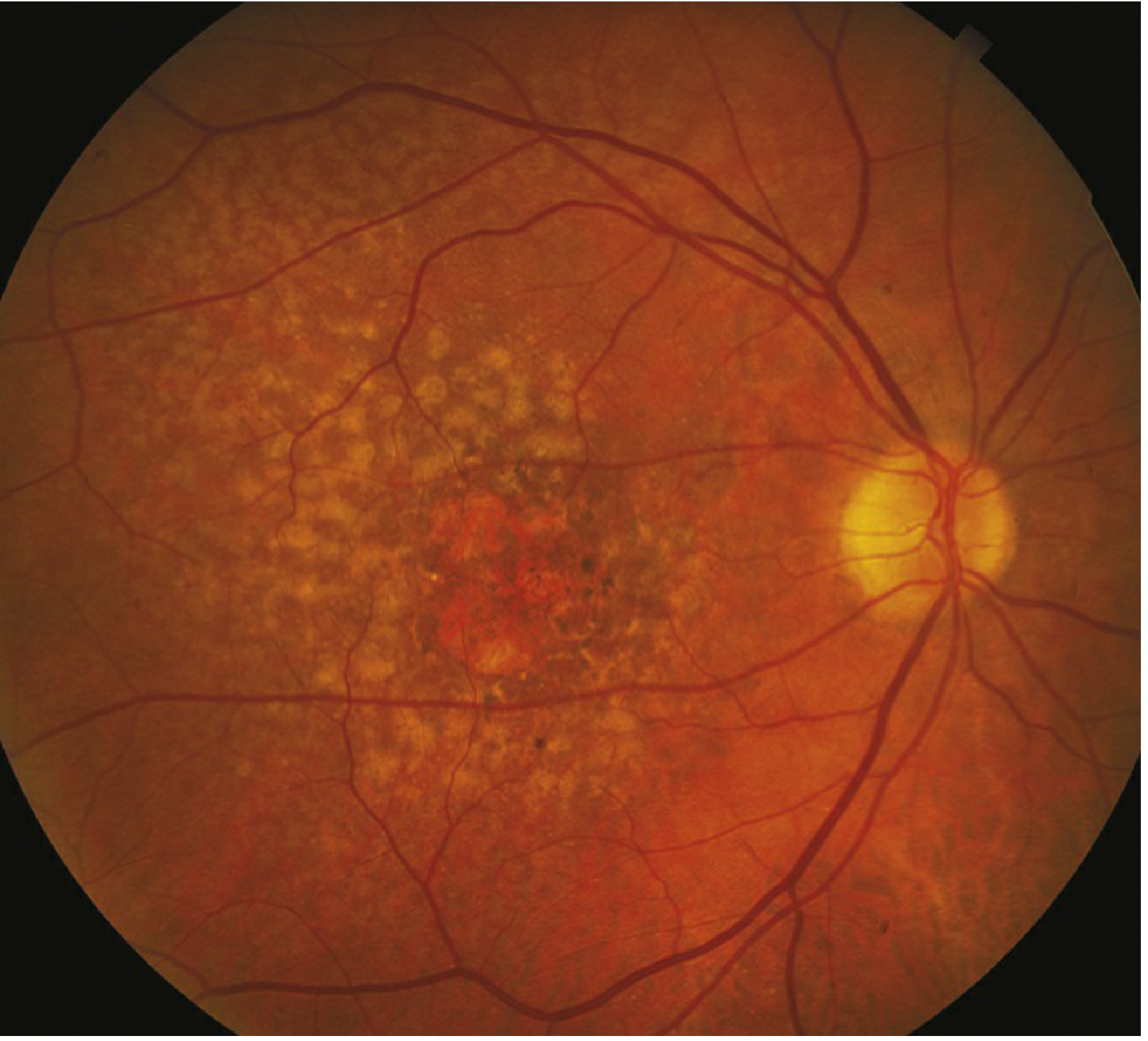
Fundus Signs:
- Subretinal fluid (SRF), macular edema (ME), or RPE detachment associated with CNV
- Subretinal or intraretinal hemorrhage
- Retinal exudates
- Subretinal fibrosis / disciform scar (end-stage)
- Retinal angiomatous proliferation (RAP) - intraretinal variant with telangiectatic vessels
A Key Clinical Pearl
Patients with peripheral retina intact can walk down a street without difficulty (peripheral function preserved), but cannot recognize faces of people they meet (macular function lost). - Goldman-Cecil Medicine
5. Diagnosis & Investigations
At the Slit-Lamp / Fundus Exam
- Dilated fundus exam with indirect ophthalmoscopy
- Soft drusen, RPE changes, CNV membranes, hemorrhage
Amsler Grid Testing
- Home monitoring tool for detecting metamorphopsia
- Patients with dry AMD at risk for CNV should perform daily Amsler grid testing and seek urgent attention if new distortion appears
Optical Coherence Tomography (OCT) - Gold Standard for Wet AMD
- Identifies subretinal fluid, intraretinal fluid, RPE detachments, CNV membranes
- Used for monitoring treatment response to anti-VEGF therapy
Fluorescein Angiography (FA)
- Identifies classic vs. occult CNV
- Classic CNV: well-defined, leaks early and progressively
- Occult CNV: poorly defined, late leakage
Indocyanine Green Angiography (ICGA)
- Better delineates occult CNV, polypoidal choroidal vasculopathy (PCV)
OCT Angiography (OCTA)
- Non-invasive visualization of CNV without dye injection
- Increasingly used in diagnosis and follow-up
Sources: Wills Eye Manual; Goldman-Cecil Medicine
6. Staging (AMD Classification)
| Stage | Features |
|---|---|
| Early AMD | Small to medium drusen (<125 µm), no pigmentary changes |
| Intermediate AMD | Large drusen (>125 µm) or medium drusen with pigmentary changes |
| Advanced Dry AMD | Geographic atrophy of RPE ± photoreceptors, not involving the fovea |
| Advanced Wet AMD | CNV with subretinal fluid/hemorrhage, disciform scar |
7. Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Myopic degeneration | Peripapillary changes, macular changes without drusen, high myopia |
| Central serous chorioretinopathy (CSCR) | Serous retinal elevation, usually <50 years, no drusen |
| Ocular histoplasmosis | Small white-yellow chorioretinal scars, peripapillary atrophy |
| Inherited macular dystrophies (Stargardt, Best disease) | Usually <50 years, familial, no drusen |
| Chloroquine toxicity | Bull's eye maculopathy, drug history |
| Angioid streaks | Sub-retinal red-brown bands radiating from optic disc |
| IPCV (polypoidal choroidal vasculopathy) | Polyp-like aneurysmal choroidal dilations on ICGA; common in Asian patients |
Source: Wills Eye Manual
8. Management
Dry AMD - No Proven Curative Treatment
AREDS Supplementation (Age-Related Eye Disease Study):
The AREDS2 formula may retard progression from intermediate to advanced AMD:
- Vitamin C (500 mg)
- Vitamin E (400 IU)
- Lutein (10 mg) + Zeaxanthin (2 mg) - replaces beta-carotene
- Zinc (80 mg)
- Copper (2 mg) - to prevent zinc-induced copper deficiency
Note: Beta-carotene is NOT recommended in smokers due to increased risk of lung cancer.
Behavioral Modifications:
- Cessation of smoking (most important)
- Control of blood pressure, blood sugar, and lipids
- Dietary changes (green leafy vegetables rich in lutein/zeaxanthin)
Geographic Atrophy - Emerging Therapy:
- Complement inhibitors are being investigated (target C3 or C5 pathway)
Low Vision Aids:
- Special magnifying glasses
- Video-based magnification aids
- Allow patients to continue independent living
Wet AMD - Anti-VEGF Therapy (Mainstay)
Intravitreal injections of anti-VEGF agents are the standard of care for wet AMD. When administered promptly, they not only prevent vision loss but can result in gains in vision.
| Drug | Class | Notes |
|---|---|---|
| Ranibizumab (Lucentis) | Anti-VEGF-A fragment (Fab) | FDA-approved, gold standard |
| Bevacizumab (Avastin) | Full anti-VEGF antibody | Off-label, widely used; comparable efficacy in CATT trial |
| Aflibercept (Eylea) | VEGF trap (VEGF-A + PlGF) | Longer dosing intervals possible |
| Faricimab (Vabysmo) | Dual inhibitor of VEGF-A + Angiopoietin-2 | Newest agent; longest dosing intervals (up to 16 weeks) |
Recent Evidence Update (2025): A network meta-analysis (PMID: 40241463) comparing all intravitreal anti-VEGF therapies for neovascular AMD showed comparable efficacy across agents. A systematic review of faricimab (PMID: 39043575) confirmed non-inferiority to ranibizumab and aflibercept with extended dosing intervals.
Treatment Regimens:
- Loading phase: Monthly injections for 3 months
- Maintenance: Pro re nata (PRN), treat-and-extend (T&E), or fixed dosing depending on agent and response
Other Treatments for Wet AMD
- Photodynamic therapy (PDT) with verteporfin - used in classic subfoveal CNV; less common since anti-VEGF era
- Laser photocoagulation - for extrafoveal CNV lesions; risk of scotoma
- Macular translocation surgery - retina detached, translocated away from CNV; then laser applied to destroy pathological vessels (advanced/salvage cases)
- Vitrectomy - for advanced cases with vitreous hemorrhage or large subretinal hemorrhage
9. Prognosis & Follow-up
- Dry AMD progresses slowly over months to decades; most patients retain some functional vision
- Wet AMD without treatment: rapid central vision loss within months
- With anti-VEGF treatment: ~33% gain >15 letters vision; 90%+ maintain or improve
- Patients with wet AMD in one eye have 10-12% annual risk of CNV developing in the fellow eye
- High-risk features for fellow eye: multiple/confluent soft drusen, RPE clumping
10. Summary Table
| Feature | Dry AMD | Wet AMD |
|---|---|---|
| Frequency | 90% of cases | 10% of cases |
| Vision loss | Gradual, over years | Sudden/rapid |
| Key finding | Drusen, geographic atrophy | CNV, subretinal fluid/hemorrhage |
| VEGF role | Not primary driver | Central driver (→ CNV) |
| Treatment | AREDS2 supplements, lifestyle | Anti-VEGF injections |
| Prognosis | Variable; can be severe | Poor if untreated; treatable if caught early |
Sources:
- Goldman-Cecil Medicine International Edition (2024)
- The Wills Eye Manual, 8th Edition
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology
- Katzung's Basic and Clinical Pharmacology, 16th Edition
- Butler et al., Acta Ophthalmol, 2025 - Network Meta-Analysis PMID 40241463
- Samacá-Samacá et al., BMJ Open Ophthalmol, 2024 - Faricimab Systematic Review PMID 39043575
Make a ppt
Reading File
Reading File
Reading File
Running Command
mkdir -p /home/daytona/workspace/amd-ppt && node /home/daytona/skills/shared/scr…
Writing File
~/amd-ppt/amd.js
const pptxgen = require("pptxgenjs");
const fs = require("fs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Age-Related Macular Degeneration (AMD)";
pres.author = "Orris Medical";
// Load images
const img0 = fs.readFileSync("/home/daytona/workspace/amd-ppt/img0.txt", "utf8"); // pathogenesis diagram dry vs wet
const img1 = fs.readFileSync("/home/daytona/workspace/amd-ppt/img1.txt", "utf8"); // fundus dry AMD
const img2 = fs.readFileSync("/home/daytona/workspace/amd-ppt/img2.txt", "utf8"); // fundus wet AMD
// ── Color Palette ──────────────────────────────────────────────
const DARK_BG = "0D1B2A"; // deep navy
const MID_BG = "1A2E42"; // slate navy
const ACCENT = "1E90FF"; // clinical blue
const ACCENT2 = "E83030"; // alert red (wet AMD)
const ACCENT3 = "2ECC71"; // treatment green
const WHITE = "FFFFFF";
const LIGHT_GRAY= "D0D8E4";
const GOLD = "F4C430"; // soft gold for headers
// ── Helper: dark slide background ──────────────────────────────
function darkBg(slide) {
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 5.625,
fill: { color: DARK_BG }, line: { type: "none" }
});
}
function midBg(slide) {
slide.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 5.625,
fill: { color: "F0F4F8" }, line: { type: "none" }
});
}
// ── Slide 1: Title ─────────────────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
// Top accent bar
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 0.08,
fill: { color: ACCENT }, line: { type: "none" }
});
// Eye cross-section decorative shape on right
s.addShape(pres.shapes.OVAL, {
x: 6.5, y: 0.8, w: 3.2, h: 3.2,
fill: { color: MID_BG, transparency: 30 },
line: { color: ACCENT, width: 1.5 }
});
s.addShape(pres.shapes.OVAL, {
x: 7.5, y: 1.8, w: 1.2, h: 1.2,
fill: { color: ACCENT, transparency: 50 },
line: { color: ACCENT, width: 0.5 }
});
// Title text
s.addText("Age-Related", {
x: 0.5, y: 0.9, w: 6.5, h: 0.8,
fontSize: 36, bold: true, color: WHITE, fontFace: "Calibri",
charSpacing: 2, margin: 0
});
s.addText("Macular Degeneration", {
x: 0.5, y: 1.65, w: 6.5, h: 0.8,
fontSize: 36, bold: true, color: ACCENT, fontFace: "Calibri",
charSpacing: 2, margin: 0
});
s.addText("(AMD)", {
x: 0.5, y: 2.4, w: 6.5, h: 0.6,
fontSize: 28, bold: false, color: LIGHT_GRAY, fontFace: "Calibri",
margin: 0
});
// Divider line
s.addShape(pres.shapes.RECTANGLE, {
x: 0.5, y: 3.1, w: 4.5, h: 0.04,
fill: { color: GOLD }, line: { type: "none" }
});
s.addText([
{ text: "Pathophysiology • Diagnosis • Management", options: { color: LIGHT_GRAY } }
], {
x: 0.5, y: 3.25, w: 8, h: 0.4, fontSize: 13, fontFace: "Calibri", margin: 0
});
s.addText([
{ text: "Sources: Goldman-Cecil Medicine | Wills Eye Manual | Robbins Pathology", options: { color: "7A8FA6", italic: true } }
], {
x: 0.5, y: 5.1, w: 9, h: 0.35, fontSize: 9.5, fontFace: "Calibri", margin: 0
});
// Bottom accent bar
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 5.545, w: 10, h: 0.08,
fill: { color: ACCENT2 }, line: { type: "none" }
});
}
// ── Slide 2: Overview & Epidemiology ──────────────────────────
{
const s = pres.addSlide();
midBg(s);
// Left accent bar
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 0.08, h: 5.625,
fill: { color: ACCENT }, line: { type: "none" }
});
// Header band
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 0.85,
fill: { color: DARK_BG }, line: { type: "none" }
});
s.addText("Overview & Epidemiology", {
x: 0.3, y: 0.1, w: 9, h: 0.65,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
// Stat boxes
const stats = [
{ val: "#1", label: "Cause of irreversible\ncentral vision loss in\nelderly (W. countries)", color: ACCENT },
{ val: "8.5%", label: "Of global blindness\ncaused by AMD", color: "8B5E3C" },
{ val: "1.75M+", label: "Americans affected", color: ACCENT2 },
{ val: "8%", label: "Cumulative incidence\nin those aged 75+", color: "2E8B57" }
];
stats.forEach((st, i) => {
const x = 0.4 + i * 2.35;
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x, y: 1.0, w: 2.1, h: 1.8,
fill: { color: WHITE },
line: { color: st.color, width: 2 },
shadow: { type: "outer", color: "000000", blur: 5, offset: 2, angle: 135, opacity: 0.1 },
rectRadius: 0.1
});
s.addText(st.val, {
x: x + 0.05, y: 1.1, w: 2.0, h: 0.7,
fontSize: 28, bold: true, color: st.color, align: "center", fontFace: "Calibri", margin: 0
});
s.addText(st.label, {
x: x + 0.05, y: 1.8, w: 2.0, h: 0.9,
fontSize: 10, color: "333333", align: "center", fontFace: "Calibri", margin: 0
});
});
// Key points
s.addShape(pres.shapes.RECTANGLE, {
x: 0.15, y: 3.0, w: 9.7, h: 2.4,
fill: { color: MID_BG }, line: { type: "none" },
shadow: { type: "outer", color: "000000", blur: 4, offset: 1, angle: 135, opacity: 0.2 }
});
s.addText([
{ text: "Key Facts", options: { bold: true, color: GOLD, breakLine: true, fontSize: 13 } },
{ text: "• Neurodegenerative disease of the retinal pigment epithelium (RPE) in the macula\n", options: { color: WHITE, fontSize: 11 } },
{ text: "• Affects both eyes; only central vision is lost — peripheral vision is spared\n", options: { color: WHITE, fontSize: 11 } },
{ text: "• Prevalence doubles each decade after age 55 | Risk: smoking, genetics (CFH gene), hypertension\n", options: { color: WHITE, fontSize: 11 } },
{ text: "• Two forms: Dry (90%) and Wet (10%) — wet causes most severe vision loss", options: { color: WHITE, fontSize: 11 } }
], {
x: 0.4, y: 3.05, w: 9.3, h: 2.3, fontFace: "Calibri", margin: 5
});
}
// ── Slide 3: Pathophysiology ───────────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 0.85,
fill: { color: MID_BG }, line: { type: "none" }
});
s.addText("Pathophysiology", {
x: 0.3, y: 0.12, w: 9, h: 0.65,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
s.addShape(pres.shapes.RECTANGLE, {
x: 9.2, y: 0, w: 0.8, h: 0.85,
fill: { color: ACCENT }, line: { type: "none" }
});
// Diagram image - Robbins
s.addImage({ data: img0, x: 0.15, y: 0.95, w: 5.6, h: 3.4 });
// Caption
s.addText("Fig: Dry vs Wet AMD — Robbins Pathologic Basis of Disease", {
x: 0.15, y: 4.35, w: 5.6, h: 0.3,
fontSize: 8, color: "7A8FA6", italic: true, fontFace: "Calibri", margin: 0
});
// Right: annotation boxes
const items = [
{ label: "RPE-Bruch's-Choriocapillaris Unit", body: "Functional triad. Disruption of any one component → photoreceptor loss", color: ACCENT },
{ label: "Dry AMD", body: "Drusen (lipoprotein deposits in Bruch's membrane) → geographic atrophy via complement activation (CFH gene)", color: "2ECC71" },
{ label: "Wet AMD", body: "VEGF-driven choroidal neovascularization (CNV) penetrates Bruch's → leakage, hemorrhage, disciform scar", color: ACCENT2 }
];
items.forEach((it, i) => {
const y = 0.95 + i * 1.5;
s.addShape(pres.shapes.RECTANGLE, {
x: 6.0, y, w: 3.8, h: 1.35,
fill: { color: MID_BG }, line: { color: it.color, width: 1.5 }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 6.0, y, w: 3.8, h: 0.3,
fill: { color: it.color }, line: { type: "none" }
});
s.addText(it.label, {
x: 6.05, y: y + 0.02, w: 3.7, h: 0.28,
fontSize: 9.5, bold: true, color: WHITE, fontFace: "Calibri", margin: 2
});
s.addText(it.body, {
x: 6.05, y: y + 0.32, w: 3.7, h: 0.95,
fontSize: 10, color: LIGHT_GRAY, fontFace: "Calibri", margin: 4
});
});
}
// ── Slide 4: Types & Clinical Features ────────────────────────
{
const s = pres.addSlide();
midBg(s);
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 0.85,
fill: { color: DARK_BG }, line: { type: "none" }
});
s.addText("Types & Clinical Features", {
x: 0.3, y: 0.12, w: 9, h: 0.65,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
// Dry AMD column
s.addShape(pres.shapes.RECTANGLE, {
x: 0.2, y: 0.95, w: 4.5, h: 4.5,
fill: { color: WHITE },
line: { color: "2ECC71", width: 2 },
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.1 }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 0.2, y: 0.95, w: 4.5, h: 0.38,
fill: { color: "2ECC71" }, line: { type: "none" }
});
s.addText("DRY AMD (90%)", {
x: 0.3, y: 0.97, w: 4.3, h: 0.35,
fontSize: 12, bold: true, color: WHITE, fontFace: "Calibri", margin: 2
});
s.addImage({ data: img1, x: 0.35, y: 1.4, w: 2.5, h: 1.6 });
s.addText("Fundus: fine macular drusen", {
x: 0.35, y: 3.0, w: 2.5, h: 0.25,
fontSize: 7.5, color: "555555", italic: true, fontFace: "Calibri", margin: 0, align: "center"
});
s.addText([
{ text: "Symptoms\n", options: { bold: true, color: "2E8B57", breakLine: false } },
{ text: "• Gradual central vision loss\n• Metamorphopsia (Amsler grid)\n• May be asymptomatic for years\n\n", options: { color: "333333" } },
{ text: "Key Signs\n", options: { bold: true, color: "2E8B57", breakLine: false } },
{ text: "• Soft drusen >60 μm\n• RPE mottling / depigmentation\n• Geographic atrophy (advanced)", options: { color: "333333" } }
], {
x: 2.9, y: 1.38, w: 1.7, h: 3.0,
fontSize: 9.5, fontFace: "Calibri", margin: 3
});
// Wet AMD column
s.addShape(pres.shapes.RECTANGLE, {
x: 5.2, y: 0.95, w: 4.5, h: 4.5,
fill: { color: WHITE },
line: { color: ACCENT2, width: 2 },
shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.1 }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 5.2, y: 0.95, w: 4.5, h: 0.38,
fill: { color: ACCENT2 }, line: { type: "none" }
});
s.addText("WET AMD (10%)", {
x: 5.3, y: 0.97, w: 4.3, h: 0.35,
fontSize: 12, bold: true, color: WHITE, fontFace: "Calibri", margin: 2
});
s.addImage({ data: img2, x: 5.35, y: 1.4, w: 2.5, h: 1.6 });
s.addText("Fundus: CNV with hemorrhage & drusen", {
x: 5.35, y: 3.0, w: 2.5, h: 0.25,
fontSize: 7.5, color: "555555", italic: true, fontFace: "Calibri", margin: 0, align: "center"
});
s.addText([
{ text: "Symptoms\n", options: { bold: true, color: ACCENT2, breakLine: false } },
{ text: "• Sudden central vision loss\n• Metamorphopsia (wavy lines)\n• Central/paracentral scotoma\n\n", options: { color: "333333" } },
{ text: "Key Signs\n", options: { bold: true, color: ACCENT2, breakLine: false } },
{ text: "• Subretinal fluid / CNV\n• Subretinal hemorrhage\n• Disciform scar (end-stage)", options: { color: "333333" } }
], {
x: 7.85, y: 1.38, w: 1.75, h: 3.0,
fontSize: 9.5, fontFace: "Calibri", margin: 3
});
}
// ── Slide 5: Risk Factors & Genetics ─────────────────────────
{
const s = pres.addSlide();
darkBg(s);
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 0.85,
fill: { color: MID_BG }, line: { type: "none" }
});
s.addText("Risk Factors & Genetics", {
x: 0.3, y: 0.12, w: 9, h: 0.65,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
// Genetic factors
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.2, y: 0.98, w: 4.5, h: 2.5,
fill: { color: "0A1628" }, line: { color: ACCENT, width: 1.5 }, rectRadius: 0.08
});
s.addText("🧬 Genetic Factors", {
x: 0.35, y: 1.05, w: 4.2, h: 0.4,
fontSize: 13, bold: true, color: ACCENT, fontFace: "Calibri", margin: 0
});
s.addText([
{ text: "CFH ", options: { bold: true, color: GOLD } },
{ text: "(Complement Factor H) — strongest association\n", options: { color: LIGHT_GRAY } },
{ text: "CFI ", options: { bold: true, color: GOLD } },
{ text: "(Complement Factor I) — regulatory gene\n", options: { color: LIGHT_GRAY } },
{ text: "Other complement regulatory gene polymorphisms\n", options: { color: LIGHT_GRAY } },
{ text: "→ Excess complement activity → RPE injury", options: { color: ACCENT, italic: true } }
], {
x: 0.35, y: 1.45, w: 4.2, h: 1.9,
fontSize: 10.5, fontFace: "Calibri", margin: 4
});
// Modifiable risk factors
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.2, y: 3.6, w: 4.5, h: 1.8,
fill: { color: "0A1628" }, line: { color: ACCENT2, width: 1.5 }, rectRadius: 0.08
});
s.addText("🚬 Modifiable Risk Factors", {
x: 0.35, y: 3.67, w: 4.2, h: 0.4,
fontSize: 13, bold: true, color: ACCENT2, fontFace: "Calibri", margin: 0
});
s.addText([
{ text: "• Smoking (strongest modifiable RF)\n", options: { bold: true, color: ACCENT2 } },
{ text: "• Hypertension • Dyslipidaemia\n• Poor glycaemic control\n• UV exposure", options: { color: LIGHT_GRAY } }
], {
x: 0.35, y: 4.07, w: 4.2, h: 1.3,
fontSize: 10.5, fontFace: "Calibri", margin: 4
});
// Non-modifiable risk factors
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 5.2, y: 0.98, w: 4.5, h: 4.42,
fill: { color: "0A1628" }, line: { color: GOLD, width: 1.5 }, rectRadius: 0.08
});
s.addText("Non-Modifiable Risk Factors", {
x: 5.35, y: 1.05, w: 4.2, h: 0.4,
fontSize: 13, bold: true, color: GOLD, fontFace: "Calibri", margin: 0
});
const nrfs = [
["Age", "Risk doubles every decade after 55; cumulative 8% at 75+"],
["Family history", "Strong genetic heritability"],
["Hyperopia", "Long-sighted individuals at higher risk"],
["Blue eyes / fair skin", "Lower macular pigment density"],
["Female sex", "Slightly higher prevalence in women"],
["Fellow eye involvement", "10–12% annual risk of CNV in second eye if first eye affected"]
];
nrfs.forEach((r, i) => {
s.addText([
{ text: r[0] + ": ", options: { bold: true, color: GOLD } },
{ text: r[1], options: { color: LIGHT_GRAY } }
], {
x: 5.35, y: 1.5 + i * 0.63, w: 4.2, h: 0.55,
fontSize: 10, fontFace: "Calibri", margin: 3
});
if (i < nrfs.length - 1) {
s.addShape(pres.shapes.RECTANGLE, {
x: 5.35, y: 2.03 + i * 0.63, w: 4.2, h: 0.01,
fill: { color: "2A3D55" }, line: { type: "none" }
});
}
});
}
// ── Slide 6: Diagnosis & Investigations ───────────────────────
{
const s = pres.addSlide();
midBg(s);
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 0.85,
fill: { color: DARK_BG }, line: { type: "none" }
});
s.addText("Diagnosis & Investigations", {
x: 0.3, y: 0.12, w: 9, h: 0.65,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
const investigations = [
{
title: "Amsler Grid",
body: "Home monitoring tool\nDetects metamorphopsia (wavy/distorted lines)\nDaily use mandatory for at-risk patients",
color: "2ECC71", icon: "📊"
},
{
title: "Dilated Fundus Exam",
body: "First-line clinical exam\nIdentifies drusen, RPE changes, CNV, hemorrhage\nBilateral evaluation essential",
color: ACCENT, icon: "👁"
},
{
title: "OCT (Gold Standard)",
body: "Detects SRF, IRF, RPE detachments, CNV\nQuantifies fluid for treatment monitoring\nOCT-A: non-invasive CNV mapping (no dye)",
color: GOLD, icon: "🔬"
},
{
title: "Fluorescein Angiography",
body: "Classic CNV: early leakage, well-defined\nOccult CNV: late, poorly defined leakage\nStill gold standard for CNV characterisation",
color: ACCENT2, icon: "💉"
},
{
title: "ICGA",
body: "Indocyanine green angiography\nBetter for occult CNV & polypoidal choroidal vasculopathy (PCV)\nEssential in Asian patients",
color: "9B59B6", icon: "🩺"
},
{
title: "AMD Staging (AREDS)",
body: "Early: small/medium drusen\nIntermediate: large drusen ±pigment change\nAdvanced: geographic atrophy or wet AMD",
color: "E67E22", icon: "📋"
}
];
investigations.forEach((inv, i) => {
const col = i % 3;
const row = Math.floor(i / 3);
const x = 0.15 + col * 3.3;
const y = 0.98 + row * 2.25;
s.addShape(pres.shapes.RECTANGLE, {
x, y, w: 3.1, h: 2.1,
fill: { color: WHITE },
line: { color: inv.color, width: 1.5 },
shadow: { type: "outer", color: "000000", blur: 4, offset: 1, angle: 135, opacity: 0.08 }
});
s.addShape(pres.shapes.RECTANGLE, {
x, y, w: 3.1, h: 0.38,
fill: { color: inv.color }, line: { type: "none" }
});
s.addText(inv.title, {
x: x + 0.05, y: y + 0.03, w: 3.0, h: 0.33,
fontSize: 11, bold: true, color: WHITE, fontFace: "Calibri", margin: 3
});
s.addText(inv.body, {
x: x + 0.08, y: y + 0.42, w: 2.95, h: 1.6,
fontSize: 9.5, color: "333333", fontFace: "Calibri", margin: 3
});
});
}
// ── Slide 7: Management — Dry AMD ─────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 0.85,
fill: { color: "0F2D1A" }, line: { type: "none" }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 0.08, h: 5.625,
fill: { color: ACCENT3 }, line: { type: "none" }
});
s.addText("Management — Dry AMD", {
x: 0.3, y: 0.12, w: 9, h: 0.65,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
// AREDS2 box
s.addShape(pres.shapes.RECTANGLE, {
x: 0.2, y: 1.0, w: 5.8, h: 3.2,
fill: { color: "0A2012" }, line: { color: ACCENT3, width: 2 }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 0.2, y: 1.0, w: 5.8, h: 0.42,
fill: { color: ACCENT3 }, line: { type: "none" }
});
s.addText("AREDS2 Supplementation Formula", {
x: 0.3, y: 1.03, w: 5.6, h: 0.38,
fontSize: 13, bold: true, color: WHITE, fontFace: "Calibri", margin: 2
});
const areds = [
["Vitamin C", "500 mg"],
["Vitamin E", "400 IU"],
["Lutein", "10 mg"],
["Zeaxanthin", "2 mg"],
["Zinc", "80 mg"],
["Copper", "2 mg (prevents zinc-induced deficiency)"]
];
areds.forEach((a, i) => {
s.addText([
{ text: a[0] + " ", options: { bold: true, color: ACCENT3 } },
{ text: a[1], options: { color: LIGHT_GRAY } }
], {
x: 0.4, y: 1.5 + i * 0.37, w: 5.5, h: 0.35,
fontSize: 10.5, fontFace: "Calibri", margin: 2
});
});
s.addShape(pres.shapes.RECTANGLE, {
x: 0.25, y: 3.9, w: 5.7, h: 0.02,
fill: { color: ACCENT3 }, line: { type: "none" }
});
s.addText([
{ text: "⚠ Beta-carotene is NOT recommended in smokers", options: { bold: true, color: ACCENT2 } },
{ text: " — increased lung cancer risk", options: { color: LIGHT_GRAY } }
], {
x: 0.3, y: 3.95, w: 5.7, h: 0.45,
fontSize: 10, fontFace: "Calibri", margin: 3
});
// Lifestyle column
s.addShape(pres.shapes.RECTANGLE, {
x: 6.2, y: 1.0, w: 3.6, h: 4.4,
fill: { color: "0A2012" }, line: { color: GOLD, width: 1.5 }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 6.2, y: 1.0, w: 3.6, h: 0.42,
fill: { color: GOLD }, line: { type: "none" }
});
s.addText("Lifestyle & Monitoring", {
x: 6.3, y: 1.03, w: 3.4, h: 0.38,
fontSize: 13, bold: true, color: DARK_BG, fontFace: "Calibri", margin: 2
});
const lifestyle = [
["Stop smoking", "Most important modifiable action"],
["Control BP", "Reduces vascular stress on RPE"],
["Control lipids", "Limit drusen progression"],
["Glycaemic control", "Prevents metabolic damage"],
["Diet", "Green leafy veg (lutein/zeaxanthin)"],
["Amsler grid", "Daily home monitoring for CNV onset"],
["Low vision aids", "Magnifiers, video aids for independence"]
];
lifestyle.forEach((l, i) => {
s.addText([
{ text: l[0] + ": ", options: { bold: true, color: GOLD } },
{ text: l[1], options: { color: LIGHT_GRAY } }
], {
x: 6.3, y: 1.5 + i * 0.55, w: 3.4, h: 0.48,
fontSize: 10, fontFace: "Calibri", margin: 3
});
});
// Footer note
s.addText("No curative treatment exists for dry AMD. Supplements retard progression from intermediate → advanced AMD.", {
x: 0.2, y: 5.1, w: 9.6, h: 0.35,
fontSize: 9, color: "5A8F70", italic: true, fontFace: "Calibri", margin: 0, align: "center"
});
}
// ── Slide 8: Management — Wet AMD ─────────────────────────────
{
const s = pres.addSlide();
midBg(s);
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 0.85,
fill: { color: DARK_BG }, line: { type: "none" }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 0.08, h: 5.625,
fill: { color: ACCENT2 }, line: { type: "none" }
});
s.addText("Management — Wet AMD (Anti-VEGF Therapy)", {
x: 0.3, y: 0.12, w: 9, h: 0.65,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
// Anti-VEGF drugs table
const drugs = [
{ name: "Ranibizumab", brand: "Lucentis", class: "Anti-VEGF-A Fab fragment", notes: "FDA-approved. Gold standard. Monthly injection.", color: ACCENT },
{ name: "Bevacizumab", brand: "Avastin", class: "Full anti-VEGF-A antibody", notes: "Off-label. Comparable efficacy (CATT trial). Lower cost.", color: "2E86AB" },
{ name: "Aflibercept", brand: "Eylea", class: "VEGF trap (VEGF-A + PlGF)", notes: "Longer dosing intervals possible (8 weeks).", color: "8E44AD" },
{ name: "Faricimab", brand: "Vabysmo", class: "Dual inhibitor: VEGF-A + Ang-2", notes: "Newest agent. Up to 16-week intervals. 2025 meta-analysis confirms non-inferiority.", color: ACCENT2 }
];
drugs.forEach((d, i) => {
const y = 0.98 + i * 1.12;
s.addShape(pres.shapes.RECTANGLE, {
x: 0.2, y, w: 9.6, h: 1.05,
fill: { color: WHITE },
line: { color: d.color, width: 1.5 },
shadow: { type: "outer", color: "000000", blur: 3, offset: 1, angle: 135, opacity: 0.08 }
});
s.addShape(pres.shapes.RECTANGLE, {
x: 0.2, y, w: 0.5, h: 1.05,
fill: { color: d.color }, line: { type: "none" }
});
s.addText(d.name, {
x: 0.85, y: y + 0.05, w: 2.2, h: 0.4,
fontSize: 13, bold: true, color: d.color, fontFace: "Calibri", margin: 0
});
s.addText("(" + d.brand + ")", {
x: 0.85, y: y + 0.48, w: 2.2, h: 0.3,
fontSize: 9.5, color: "666666", italic: true, fontFace: "Calibri", margin: 0
});
s.addShape(pres.shapes.RECTANGLE, {
x: 3.15, y: y + 0.18, w: 0.02, h: 0.7,
fill: { color: "CCCCCC" }, line: { type: "none" }
});
s.addText(d.class, {
x: 3.3, y: y + 0.05, w: 2.8, h: 0.95,
fontSize: 10, color: "333333", fontFace: "Calibri", margin: 4, valign: "middle"
});
s.addShape(pres.shapes.RECTANGLE, {
x: 6.2, y: y + 0.18, w: 0.02, h: 0.7,
fill: { color: "CCCCCC" }, line: { type: "none" }
});
s.addText(d.notes, {
x: 6.35, y: y + 0.05, w: 3.3, h: 0.95,
fontSize: 10, color: "333333", fontFace: "Calibri", margin: 4, valign: "middle"
});
});
// Footer regimen note
s.addShape(pres.shapes.RECTANGLE, {
x: 0.2, y: 5.1, w: 9.6, h: 0.4,
fill: { color: "EFF4F9" }, line: { color: ACCENT, width: 1 }
});
s.addText([
{ text: "Treatment Regimen: ", options: { bold: true, color: ACCENT } },
{ text: "Loading phase (3 monthly injections) → Maintenance via PRN or treat-and-extend (T&E) protocol | ", options: { color: "333333" } },
{ text: "Early treatment = gains in vision (33% gain >15 letters)", options: { color: ACCENT2, bold: true } }
], {
x: 0.3, y: 5.12, w: 9.4, h: 0.36,
fontSize: 9.5, fontFace: "Calibri", margin: 2
});
}
// ── Slide 9: Differential Diagnosis ───────────────────────────
{
const s = pres.addSlide();
darkBg(s);
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 0.85,
fill: { color: MID_BG }, line: { type: "none" }
});
s.addText("Differential Diagnosis", {
x: 0.3, y: 0.12, w: 9, h: 0.65,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
const diffs = [
{ dx: "Myopic Degeneration", clue: "High myopia, peripapillary changes, macular changes WITHOUT drusen", color: ACCENT },
{ dx: "CSCR", clue: "Central serous chorioretinopathy. Serous elevation, usually <50 yrs, no drusen, often males", color: "27AE60" },
{ dx: "Ocular Histoplasmosis", clue: "White-yellow chorioretinal scars, peripapillary atrophy, CNV possible", color: GOLD },
{ dx: "Stargardt / Best Disease", clue: "Inherited macular dystrophies. Usually <50 yrs, familial, no drusen, variable atrophy", color: "9B59B6" },
{ dx: "Chloroquine Toxicity", clue: "Bull's-eye maculopathy — ring of hyperpigmentation. Drug history essential", color: ACCENT2 },
{ dx: "Angioid Streaks", clue: "Red-brown/gray bands radiating from optic disc. Associated with pseudoxanthoma elasticum", color: "E67E22" },
{ dx: "IPCV (Polypoidal Choroidal Vasculopathy)", clue: "Polyp-like aneurysmal choroidal dilations on ICGA. Common in Asian patients. Serosanguineous RPE detachments", color: "1ABC9C" }
];
diffs.forEach((d, i) => {
const col = i < 4 ? 0 : 1;
const row = i < 4 ? i : i - 4;
const x = col === 0 ? 0.2 : 5.15;
const y = 0.98 + row * 1.17;
const w = col === 0 ? 4.7 : 4.7;
s.addShape(pres.shapes.RECTANGLE, {
x, y, w, h: 1.1,
fill: { color: "0A1628" }, line: { color: d.color, width: 1 }
});
s.addShape(pres.shapes.RECTANGLE, {
x, y, w: 0.35, h: 1.1,
fill: { color: d.color }, line: { type: "none" }
});
s.addText(d.dx, {
x: x + 0.45, y: y + 0.05, w: w - 0.5, h: 0.38,
fontSize: 10.5, bold: true, color: d.color, fontFace: "Calibri", margin: 2
});
s.addText(d.clue, {
x: x + 0.45, y: y + 0.43, w: w - 0.5, h: 0.6,
fontSize: 9.5, color: LIGHT_GRAY, fontFace: "Calibri", margin: 2
});
});
}
// ── Slide 10: Prognosis & Summary ─────────────────────────────
{
const s = pres.addSlide();
darkBg(s);
// Top bar
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 0, w: 10, h: 0.08,
fill: { color: ACCENT }, line: { type: "none" }
});
s.addText("Prognosis & Key Summary", {
x: 0.3, y: 0.18, w: 9, h: 0.65,
fontSize: 22, bold: true, color: WHITE, fontFace: "Calibri", margin: 0
});
s.addShape(pres.shapes.RECTANGLE, {
x: 0.3, y: 0.82, w: 9.4, h: 0.03,
fill: { color: ACCENT }, line: { type: "none" }
});
// Summary table
const rows = [
["", "DRY AMD", "WET AMD"],
["Frequency", "90% of cases", "10% of cases"],
["Vision loss", "Gradual (years to decades)", "Rapid / sudden"],
["Key finding", "Drusen, geographic atrophy", "CNV, hemorrhage, SRF"],
["VEGF role", "Not primary driver", "Central driver"],
["Treatment", "AREDS2 + lifestyle", "Anti-VEGF injections"],
["Prognosis", "Variable; can preserve vision", "Good if treated early; poor if not"]
];
const colW = [2.0, 3.5, 3.5];
const colX = [0.3, 2.4, 5.95];
rows.forEach((row, ri) => {
row.forEach((cell, ci) => {
const isHeader = ri === 0;
const isRowHeader = ci === 0 && ri > 0;
const bg = isHeader ? ACCENT : (ri % 2 === 0 ? "1A2E42" : "0D1B2A");
s.addShape(pres.shapes.RECTANGLE, {
x: colX[ci], y: 0.93 + ri * 0.63, w: colW[ci], h: 0.6,
fill: { color: bg }, line: { color: "2A3D55", width: 0.5 }
});
s.addText(cell, {
x: colX[ci] + 0.05, y: 0.95 + ri * 0.63, w: colW[ci] - 0.1, h: 0.56,
fontSize: isHeader ? 11 : (isRowHeader ? 10.5 : 10),
bold: isHeader || isRowHeader,
color: isHeader ? WHITE : (isRowHeader ? GOLD : LIGHT_GRAY),
fontFace: "Calibri", align: isHeader ? "center" : "left", valign: "middle", margin: 4
});
});
});
// Prognosis callouts
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 0.3, y: 5.1, w: 4.3, h: 0.42,
fill: { color: "0A2012" }, line: { color: ACCENT3, width: 1 }, rectRadius: 0.06
});
s.addText("✓ Anti-VEGF: 33% gain >15 letters | 90%+ maintain/improve vision", {
x: 0.4, y: 5.12, w: 4.1, h: 0.38,
fontSize: 9, color: ACCENT3, fontFace: "Calibri", margin: 3
});
s.addShape(pres.shapes.ROUNDED_RECTANGLE, {
x: 5.0, y: 5.1, w: 4.7, h: 0.42,
fill: { color: "1A0A0A" }, line: { color: ACCENT2, width: 1 }, rectRadius: 0.06
});
s.addText("⚠ Fellow eye: 10–12% annual risk of CNV if one eye already affected", {
x: 5.1, y: 5.12, w: 4.5, h: 0.38,
fontSize: 9, color: ACCENT2, fontFace: "Calibri", margin: 3
});
// Bottom bar
s.addShape(pres.shapes.RECTANGLE, {
x: 0, y: 5.545, w: 10, h: 0.08,
fill: { color: ACCENT2 }, line: { type: "none" }
});
}
// ── Write file ─────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/amd-ppt/AMD_Ophthalmology.pptx" })
.then(() => console.log("SUCCESS: AMD_Ophthalmology.pptx written"))
.catch(e => { console.error("ERROR:", e); process.exit(1); });
Running Command
cd /home/daytona/workspace/amd-ppt && node amd.js 2>&1
Running Command
ls -lh /home/daytona/workspace/amd-ppt/AMD_Ophthalmology.pptx
Your AMD presentation is ready (3.1 MB):
AMD Ophthalmology
Presentation · PPTX
What's inside — 10 slides with a deep navy/clinical blue theme and embedded fundus photos:
| Slide | Content |
|---|---|
| 1 | Title slide — AMD with design accents |
| 2 | Overview & Epidemiology — 4 stat boxes + key facts |
| 3 | Pathophysiology — Robbins dry vs wet AMD diagram (embedded) + annotated mechanism boxes |
| 4 | Types & Clinical Features — Side-by-side dry vs wet with real fundus photographs |
| 5 | Risk Factors & Genetics — CFH/CFI genetics, modifiable vs non-modifiable RF |
| 6 | Diagnosis & Investigations — 6 investigation cards (Amsler, OCT, FA, ICGA, staging) |
| 7 | Management — Dry AMD — Full AREDS2 formula + lifestyle/monitoring column |
| 8 | Management — Wet AMD — Anti-VEGF drug table (Ranibizumab, Bevacizumab, Aflibercept, Faricimab) |
| 9 | Differential Diagnosis — 7 differentials with distinguishing features |
| 10 | Prognosis & Summary — Comparison table + prognosis callouts |
This is a shared conversation. Sign in to Orris to start your own chat.