HIV
Reading File
search_medical_text
HIV etiology pathophysiology transmission epidemiology
search_medical_text
HIV diagnosis staging antiretroviral therapy management
search_medical_image
HIV life cycle CD4 lymphocyte diagram
GradeResponse
GradeResponse
GradeResponse
HIV (Human Immunodeficiency Virus)
Overview
HIV is a retrovirus (Lentivirus family) that targets CD4+ T-lymphocytes, macrophages, and dendritic cells, progressively destroying cell-mediated immunity. Untreated, it leads to Acquired Immunodeficiency Syndrome (AIDS). Two types exist: HIV-1 (global, more virulent) and HIV-2 (predominantly West Africa, slower progression).
Transmission
| Route | Key Details |
|---|---|
| Sexual contact | Most common globally; receptive anal intercourse carries highest per-act risk |
| Blood-borne | IV drug use, transfusions, needle-stick injuries |
| Vertical (mother-to-child) | In utero, intrapartum, or via breastfeeding |
| Healthcare personnel to patient | Extremely rare; mostly linked to substance use diversion |
Risk is proportional to viral load — an undetectable viral load renders transmission effectively impossible (U=U: Undetectable = Untransmittable).
Pathophysiology
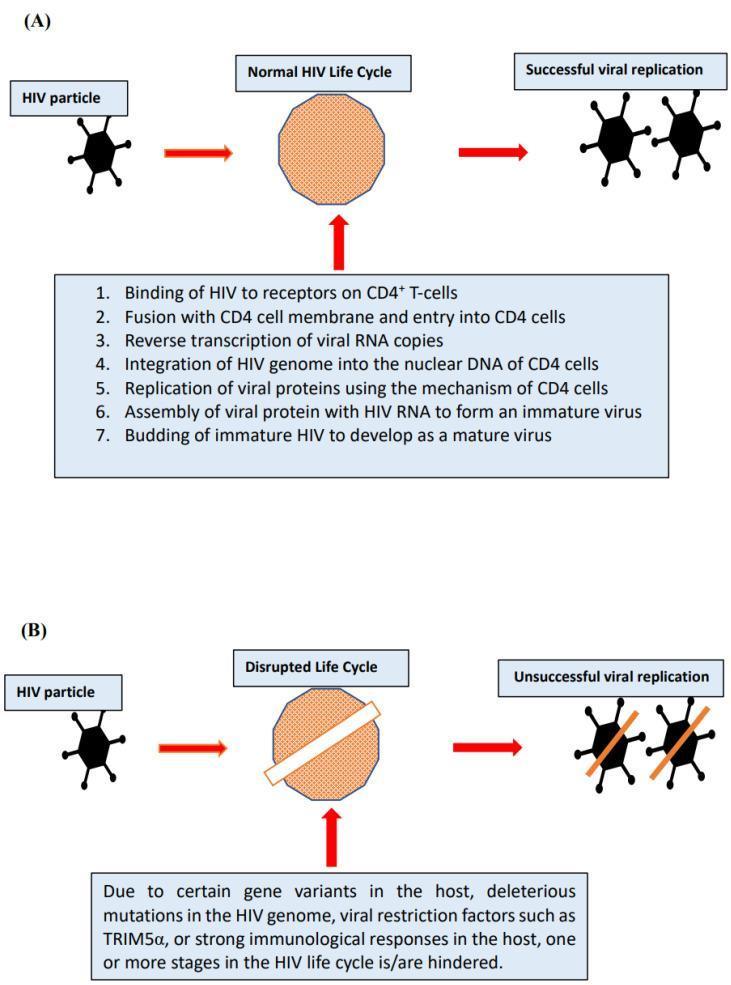
HIV binds CD4 receptors and CCR5/CXCR4 co-receptors on T-helper cells. The viral life cycle proceeds through:
- Binding & fusion to CD4+ T-cell
- Reverse transcription (RNA → DNA via reverse transcriptase)
- Integration into host genome (provirus)
- Replication and transcription
- Assembly & budding of new virions
Progressive CD4+ T-cell depletion leads to immunosuppression. AIDS is defined as CD4 count < 200 cells/μL or the presence of an AIDS-defining illness.
Clinical Stages
1. Acute HIV Infection (2–4 weeks post-exposure)
- Flu-like syndrome: fever, lymphadenopathy, pharyngitis, rash, myalgias, headache
- Very high viral load; highly infectious
- Often missed or misdiagnosed as mononucleosis
2. Chronic HIV Infection (Clinical Latency)
- Asymptomatic or mild lymphadenopathy
- Ongoing viral replication; CD4 count slowly declines
- Can last years (median ~10 years untreated)
3. AIDS (CD4 < 200 cells/μL)
- Susceptibility to opportunistic infections (OIs) and AIDS-defining malignancies
AIDS-Defining Conditions (Selected)
| CD4 Threshold | Opportunistic Infections |
|---|---|
| < 500 | Oral/vaginal candidiasis, TB, Kaposi sarcoma, lymphoma |
| < 200 | Pneumocystis jirovecii pneumonia (PCP), Toxoplasmosis |
| < 100 | Cryptococcal meningitis, disseminated MAC |
| < 50 | CMV retinitis, disseminated MAC |
Diagnosis
- 4th-generation Ag/Ab combination immunoassay — initial test of choice (detects both p24 antigen and antibodies)
- HIV-1/HIV-2 differentiation immunoassay — confirmatory
- HIV RNA PCR (viral load) — confirms acute infection when antibodies are not yet present; also used to monitor treatment
- CD4+ T-cell count — staging, treatment decisions, OI prophylaxis thresholds
Management
Antiretroviral Therapy (ART)
Per Harrison's Principles of Internal Medicine (21st Ed., p. 5957), ART should be initiated as soon as possible following HIV diagnosis. The primary goals are:
- Suppress viral load to undetectable (< 50 copies/mL)
- Restore/preserve CD4 count
- Prevent OIs and transmission
Note: A brief delay (several weeks) may be warranted before initiating ART in cases of cryptococcal or TB meningitis, to reduce the risk of severe Immune Reconstitution Inflammatory Syndrome (IRIS).
ART Drug Classes
| Class | Mechanism | Examples |
|---|---|---|
| NRTIs | Inhibit reverse transcriptase (chain termination) | Tenofovir (TDF/TAF), Emtricitabine (FTC), Abacavir (ABC) |
| NNRTIs | Non-competitive reverse transcriptase inhibition | Efavirenz, Rilpivirine, Doravirine |
| PIs | Inhibit HIV protease | Darunavir, Atazanavir (+ ritonavir/cobicistat boost) |
| INSTIs | Inhibit integrase | Dolutegravir, Bictegravir, Raltegravir |
| Entry inhibitors | Block CCR5 or fusion | Maraviroc, Enfuvirtide |
Preferred first-line regimens typically consist of 2 NRTIs + 1 INSTI (e.g., Bictegravir/TAF/FTC as a single daily tablet).
OI Prophylaxis (by CD4 threshold)
| CD4 Count | Prophylaxis |
|---|---|
| < 200 | TMP-SMX for PCP |
| < 100 | TMP-SMX also covers Toxoplasma; add if seropositive |
| < 50 | Azithromycin for MAC |
Prevention
- PrEP (Pre-Exposure Prophylaxis): TDF/FTC (Truvada) or TAF/FTC (Descovy) daily, or on-demand (2-1-1 regimen) — highly effective in high-risk individuals
- PEP (Post-Exposure Prophylaxis): 28-day course started within 72 hours of exposure
- Condom use, harm reduction programs, needle exchange
- MTCT prevention: ART during pregnancy, elective C-section if viral load > 1000 copies/mL, avoidance of breastfeeding where safe alternatives exist
Prognosis
With modern ART, people living with HIV who are diagnosed early and maintain viral suppression have a near-normal life expectancy. The key predictors of outcome are:
- Time to ART initiation
- Adherence to therapy
- CD4 count nadir
- Presence of co-infections (HBV, HCV, TB)
This is a shared conversation. Sign in to Orris to start your own chat.