St elevation in 2,3 avf
Reading File
search_medical_text
ST elevation leads II III aVF inferior STEMI ECG diagnosis
search_medical_text
inferior STEMI management treatment right ventricular infarction
search_medical_image
ST elevation inferior leads II III aVF ECG inferior STEMI
GradeResponse
GradeResponse
GradeResponse
ST Elevation in II, III, aVF — Inferior STEMI
Localization
ST elevation in leads II, III, and aVF localizes to the inferior wall of the left ventricle (Harrison's, p. 6804). This is the classic ECG signature of an inferior STEMI and represents transmural ischemia of the inferior myocardium.
Culprit Artery
| Finding | Likely Culprit |
|---|---|
| ST elevation III > II | Right Coronary Artery (RCA) occlusion (~80% of cases) |
| ST elevation II > III | Left Circumflex (LCx) occlusion (~20% of cases) |
| ST elevation in V5–V6 as well | LCx more likely |
Key Associated ECG Findings
Reciprocal changes (look for these to confirm):
- ST depression in I and aVL — hallmark reciprocal change; confirms inferior STEMI and rules out pericarditis
- ST depression in V1–V3 — suggests posterior wall extension
Right Ventricular (RV) involvement — critical to identify:
- Seen in ~40% of inferior STEMIs (proximal RCA occlusion)
- Diagnose with right-sided leads: ST elevation ≥1 mm in V4R is most specific
- Always obtain right-sided leads (V3R–V4R) in every inferior STEMI
ECG Example
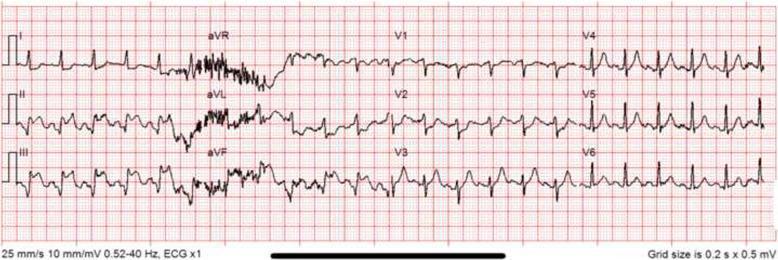
ST elevation in II, III, aVF with reciprocal ST depression in I and aVL. Lead III elevation > Lead II elevation, consistent with RCA occlusion. Pathological Q waves indicate infarction progression.
Differentials for Inferior ST Elevation
| Condition | Distinguishing Features |
|---|---|
| Inferior STEMI | Reciprocal depression in I/aVL; dynamic changes; symptoms |
| Pericarditis | Diffuse ST elevation; no reciprocal changes (except aVR); PR depression |
| Early repolarization | Concave ("smiley face") ST morphology; no reciprocal changes; asymptomatic |
| Pulmonary embolism | May mimic; look for S1Q3T3, right heart strain pattern |
| Hyperkalemia | Peaked T-waves, wide QRS, no true ST elevation pattern |
Immediate Management
- Activate cath lab — door-to-balloon time <90 minutes (primary PCI is first-line)
- Dual antiplatelet therapy: Aspirin 325 mg + P2Y12 inhibitor (ticagrelor or prasugrel preferred over clopidogrel)
- Anticoagulation: Unfractionated heparin or bivalirudin
- Nitrates — USE WITH CAUTION if RV infarction suspected: can precipitate severe hypotension (RV is preload-dependent)
- IV fluids if RV infarction with hypotension (volume resuscitation)
- Avoid diuretics and morphine in RV infarction
RV Infarction — Special Considerations
The triad of hypotension + clear lung fields + elevated JVP in the setting of inferior STEMI = RV infarction until proven otherwise. Management differs critically:
- Aggressive IV fluids (normal saline boluses)
- Early reperfusion of the RCA
- Avoid vasodilators (nitrates, morphine, diuretics)
- Dopamine/norepinephrine if refractory hypotension
Bottom line: ST elevation in II, III, aVF is inferior STEMI until proven otherwise. Get right-sided leads immediately, activate the cath lab, and be alert for RV involvement before giving nitrates.
T elevation in 2,3 and t inversion in avf
search_medical_text
T wave elevation leads II III T wave inversion aVF ECG differential diagnosis
search_medical_image
T wave inversion aVF inferior leads ECG pattern
GradeResponse
GradeResponse
This is an interesting and specific ECG pattern worth carefully parsing.
T Wave Elevation in II & III + T Wave Inversion in aVF
Understanding the Pattern
This combination — upright/tall T waves in II and III, but inverted T wave in aVF — is unusual and requires careful interpretation. Here's why:
Normally, leads II, III, and aVF all "look" at the inferior wall from slightly different angles:
- Lead II: 60° (between I and aVF)
- Lead III: 120°
- aVF: 90° (directly inferior)
When T waves are discordant across these three inferior leads (positive in II & III but inverted in aVF), this suggests the T wave vector is oriented such that it projects away from aVF (superiorly or leftward) but toward II and III.
Key Differentials
| Condition | Mechanism | Supporting Features |
|---|---|---|
| Normal variant / lead placement error | aVF electrode misplaced or loose | No symptoms; resolves with repeat ECG |
| Dextrocardia | Rightward axis shifts T vector | Absent R-wave progression V1–V6; axis abnormality |
| Right ventricular hypertrophy / strain | RV dominance shifts repolarization vector | Tall R in V1, RAD, P pulmonale |
| Pulmonary embolism | Acute RV strain | S1Q3T3, sinus tachycardia, right heart strain |
| Post-inferior MI (evolving) | After reperfusion, T-wave inversion develops unevenly | History of prior STEMI; Q waves may be present |
| Hyperacute T waves in II & III (early ischemia) | Early inferior occlusion with uneven repolarization | Dynamic; evolves to ST elevation; chest pain |
| Wellens-like pattern shifted inferiorly | Critical ischemia with reperfusion | Clinical context critical |
| Limb lead reversal (LA/LL swap) | LA and LL electrode swap | Lead I appears inverted; aVR/aVL appearance reversed |
Most Important Consideration: Lead Reversal
Left arm (LA) / Left leg (LL) reversal is one of the most common technical errors and produces exactly this pattern:
- Leads II and III swap appearance
- aVF is unaffected (uses both LA and LL mathematically, so shows different changes)
Always verify electrode placement before interpreting this pattern clinically.
If Ischemia is the Concern
Tall T waves in II and III can represent hyperacute T waves — the earliest sign of inferior wall ischemia, appearing before ST elevation. If:
- Patient has chest pain, diaphoresis, or hemodynamic instability
- T waves are asymmetric, broad-based, or taller than usual
- Pattern is dynamic on serial ECGs
→ Treat as possible early inferior STEMI equivalent and obtain:
- Repeat ECG in 15–20 minutes
- Right-sided leads (V3R–V4R)
- Posterior leads (V7–V9)
- Troponin (serial)
- Urgent cardiology review
Post-MI Evolutionary Pattern
If the patient has a known prior inferior STEMI, T inversion in aVF (with persistent positivity in II/III) can represent the subacute/evolving phase of infarction as repolarization abnormalities develop unevenly across the inferior territory.
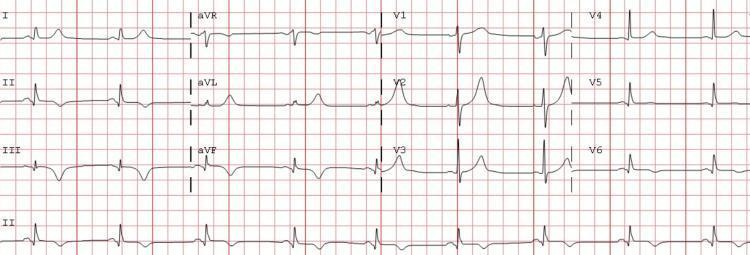
Subacute inferior MI with T-wave inversions in inferior leads following resolution of ST elevation — illustrates how T-wave changes can be heterogeneous across II, III, aVF during evolution.
Bottom Line
| Priority | Action |
|---|---|
| 1st | Check electrode placement — rule out LA/LL reversal |
| 2nd | Assess clinical context — symptoms, prior MI history |
| 3rd | Serial ECGs to assess for dynamic change |
| 4th | If any suspicion of active ischemia, manage as ACS until proven otherwise |
The key question is: is this a technical artifact or a true electrical finding? In an asymptomatic patient with no prior history, lead misplacement is the most likely explanation. In a symptomatic patient, treat as ischemia until proven otherwise.
This is a shared conversation. Sign in to Orris to start your own chat.