I now have all the supplementary material needed. Let me compile the updated and enhanced long case incorporating IAL classification (New Indian Classification), Jopling/Ridley original concepts, nerve grading from the IAL Practical Manual, and additional details from Dermatology 2-Volume Set (Bourke/Griffiths equivalent), Fitzpatrick's, and Park's.
LEPROSY (Hansen's Disease) - Complete Long Case for Dermatology Residency
Updated Edition with IAL, Ridley-Jopling & Nepal Guidelines
Primary References:
- Ridley DS & Jopling WH (1966). Classification of Leprosy According to Immunity: A Five-Group System. Int J Lepr 34(3):255-273
- IAL (Indian Association of Leprologists) - New Indian Classification (1981) / IAL Textbook of Leprosy concepts via Practical Manual of Leprosy
- International Textbook of Leprosy (internationaltextbookofleprosy.org)
- Andrews' Diseases of the Skin, 13th ed. (Clinical Dermatology)
- Dermatology, 2-Volume Set 5e (Bourke, Coulson, English et al.)
- Fitzpatrick's Dermatology, 9th ed.
- Park's Textbook of Preventive & Social Medicine, 26th ed.
- Red Book 2021 (AAP)
- Nepal National Leprosy Strategy 2021-2025
CLASSIFICATIONS - THE ESSENTIAL FRAMEWORK
Before the history and examination, a dermatology resident must be clear on all three classification systems used in practice:
1. RIDLEY-JOPLING (R-J) CLASSIFICATION (1966) - Gold Standard for Clinical & Research Use
Proposed by Ridley DS and Jopling WH based on clinical, bacteriological, immunological, and histological criteria. Published in Int J Lepr 1966;34(3):255-273. It places leprosy on a continuous spectrum from high CMI (tuberculoid) to absent CMI (lepromatous):
| Group | Abbreviation | CMI | BI | Lepromin |
|---|
| Tuberculoid | TT | Maximal | 0 | ++ to +++ |
| Borderline Tuberculoid | BT | High | 0 to 1+ | + to ++ |
| Mid-Borderline | BB | Moderate | 1+ to 3+ | ± |
| Borderline Lepromatous | BL | Low | 3+ to 5+ | - |
| Lepromatous (polar) | LL (LLp/LLs) | Absent | 5+ to 6+ | Strongly - |
Jopling's key insight (1966): The borderline group is immunologically unstable - borderline patients can shift toward TT (upgrading/reversal) or toward LL (downgrading), unlike the stable polar forms TT and LL. This instability is the biological basis for Type 1 (reversal) reactions.
2. NEW INDIAN CLASSIFICATION (IAL, 1981)
Adopted by the Indian Association of Leprologists at their conference in 1981. A simplified 5-group system that incorporated the maculoanesthetic form into TT:
| IAL Group | Corresponds to R-J |
|---|
| I - Indeterminate | Indeterminate |
| T - Tuberculoid | TT + maculoanesthetic |
| B - Borderline | BT + BB + BL |
| L - Lepromatous | LL |
| P - Polyneuritis | Pure neuritic leprosy |
IAL Key Principle: The Polyneuritis (P) group formally recognizes pure neuritic leprosy as a distinct category - important because Nepal has a high burden of pure neuritic leprosy (up to 5% of new cases). The IAL textbook emphasizes that this category should never be missed.
3. WHO OPERATIONAL CLASSIFICATION (Used in Nepal for MDT)
| Category | Definition |
|---|
| Paucibacillary (PB) | 1-5 skin lesions + SSS negative + ≤1 nerve trunk involved |
| Multibacillary (MB) | >5 skin lesions OR SSS positive OR >1 nerve trunk involved |
Nepal Program Note: From 2023, WHO updated to uniform 3-drug MDT for both PB and MB (only duration differs: 6 months vs. 12 months). Nepal's National Leprosy Strategy 2021-2025 is aligning to this update.
PART 1: DETAILED HISTORY TAKING
APPROACH TO THE PATIENT
Begin by establishing rapport. In Nepal, leprosy carries significant social stigma. Patients are often reluctant to disclose symptoms or may have delayed seeking care for months to years. A non-judgmental, empathetic opening is essential.
"I am going to ask you some questions about your illness. Everything you tell me is strictly confidential."
Always take the history in the patient's language or with an interpreter. The IAL Textbook of Leprosy emphasizes that in community settings, health workers often conduct the initial screening; at the dermatology level, a full structured history is mandatory.
A. PRESENTING COMPLAINTS
Record in order of duration (longest first):
- Skin patch/discoloration - duration
- Numbness or altered sensation - location, duration
- Weakness of hand, foot, or face - duration
- Thickening or pain in a nerve - location
- Deformity of fingers, toes, foot
- Painless wounds or ulcers
B. HISTORY OF PRESENTING ILLNESS
1. Regarding Skin Lesion(s)
Ask each of the following with clinical significance:
| Question | Clinical Significance |
|---|
| When did you first notice the patch? | Indeterminate/TT: may be months to years old; LL: insidious onset over years |
| How many patches do you have? | Fundamental for WHO classification (≤5 = PB; >5 = MB); count lesions precisely |
| Where did it start? Which body part? | TT/BT: face, limbs, trunk - asymmetric; LL: symmetric, face, ears, extremities |
| Has the number of patches increased? | Suggests MB spectrum or ongoing exposure/downgrading |
| Has it grown in size or spread? | Active disease vs. resolving (TT may spontaneously heal centrally) |
| What is the color of the patch - lighter or darker than normal skin? | Hypopigmented (most common); erythematous in fair-skinned; diffuse in LL |
| Is the surface dry, scaly, or hairless within the patch? | Anhidrosis + hair loss = autonomic fiber damage (classic TT/BT) |
| Does the patch itch? | LEPROSY DOES NOT ITCH - absence of itch in a hypopigmented patch is a cardinal clue |
| Can you feel the touch of your finger on the patch? | Loss of sensation = cardinal sign; compare with normal skin |
| Did the patch become suddenly red, swollen, and tender? | Type 1 (Reversal) reaction in borderline types - URGENT |
| Did new painful red bumps appear on skin not previously affected? | ENL (Type 2 reaction) in BL/LL - URGENT |
IAL textbook emphasizes: Never dismiss a hypopigmented patch with normal sensation as "definitely not leprosy" - indeterminate leprosy may have near-normal sensation. Always correlate with nerve examination and SSS.
2. Regarding Neural Symptoms - Ask Systematically
The IAL Practical Manual protocol for neural history:
| Question | Significance |
|---|
| Do you have numbness or reduced feeling anywhere? | Primary neuropathic complaint; 90% of patients first notice numbness even before skin lesions |
| Can you distinguish hot from cold with your hands/feet? | Temperature is lost first (small fiber, A-delta/C); "dissociation of sensibility" - highly suspicious for leprosy per Jopling |
| Have you ever accidentally burned yourself while cooking? | Loss of protective temperature sensation |
| Do you have tingling or "pins and needles"? | May indicate early active neuritis |
| Do you have pain along any nerve (arm, leg)? | Acute neuritis - urgently needs steroid |
| Can you grip things normally? | Ulnar nerve (grip strength reduced in claw hand) |
| Can you spread your fingers apart? | Interosseous weakness - ulnar nerve |
| Can you oppose your thumb? | Median nerve - thenar weakness |
| Can you lift your foot/toes when walking? | Foot drop - common peroneal nerve |
| Can you close your eye completely? | Zygomatic branch of facial nerve - lagophthalmos |
| Do you have eye pain, redness, blurring of vision? | Iritis/iridocyclitis (ENL), exposure keratitis (lagophthalmos), corneal neuropathy |
| Have you cut or injured your hand/foot without feeling it? | Anaesthetic hand/foot - high risk for trophic ulcers |
| Has weakness appeared suddenly or come on gradually? | Sudden = reaction-associated acute neuritis; gradual = chronic neuropathy |
3. Regarding Leprosy Reactions
Reactions are an emergency. Per IAL guidelines, they are the principal pathway by which nerve damage occurs.
| Question | Type 1 Reaction Features | Type 2 (ENL) Features |
|---|
| Existing lesions become red/swollen/tender? | YES - cardinal feature | Sometimes |
| New red nodular lesions on uninvolved skin? | No | YES - cardinal feature |
| Fever, malaise? | Uncommon | Common |
| Joint pains? | Uncommon | Common |
| Testicular pain/swelling? | No | Yes (orchitis in LL) |
| Eye redness/pain? | Rare | Common (iritis in ENL) |
| Nerve pain suddenly severe? | Very common (severe neuritis) | Present but less severe |
4. Systemic Review
| System | Question | Significance |
|---|
| Nose | Blocked nose, blood from nose, change in nose shape | LL - nasal mucosa earliest internal site; saddle nose deformity |
| Voice | Hoarseness | Laryngeal leprosy (LL) |
| Eyes | Eyebrow/eyelash loss, redness, vision change | Madarosis (LL); iritis (ENL); corneal ulcer (lagophthalmos) |
| Testes | Pain, swelling, infertility | LL - testicular infiltration → atrophy → impotence, gynecomastia |
| Hands/feet | Painless wounds, ulcers, finger shortening | Trophic changes from anesthesia |
| Mental health | Low mood, social withdrawal, suicidal thoughts | Stigma - a major cause of morbidity in Nepal |
C. PAST HISTORY
| Question | Significance |
|---|
| Previous episodes of similar patches? | Reactivation/relapse |
| Previous MDT treatment - which drugs, how long, completion? | Current status (on treatment, relapse, default) |
| Reactions during previous treatment? | Risk factor for future reactions |
| Previous deformity or nerve damage? | Establish baseline disability grading |
| Tuberculosis history | Co-infection; BCG status; rifampicin interactions |
| Diabetes mellitus, alcohol use | Confounding neuropathy; compliance risk |
D. FAMILY AND CONTACT HISTORY
Nepal National Leprosy Strategy mandates contact screening. Household contacts have 8-10 times higher risk.
| Question | Significance |
|---|
| Anyone in household with skin patches, numbness, or similar condition? | Direct transmission risk; must be screened and offered SDR-PEP |
| Family history of leprosy across generations? | HLA-associated genetic susceptibility (HLA-DR2, HLA-DR3 in TT; HLA-DQ1 in LL) |
| Who at home has had closest physical contact? | Identifies highest-risk contacts for priority screening |
| Have contacts been screened by health worker? | Nepal program compliance check |
E. PERSONAL, SOCIAL & OCCUPATIONAL HISTORY
| Question | Significance |
|---|
| Residence - which district/province? | Province 2 (Terai) = highest burden in Nepal; Terai plains = endemic |
| Occupation | Agricultural, forestry workers in endemic areas; indoor crowding at work |
| Living conditions | Overcrowding; poor ventilation = facilitates droplet transmission |
| Nutritional status | Malnutrition suppresses CMI; promotes downgrading toward LL |
| Alcohol use | Peripheral neuropathy co-existence; compliance issues |
| Awareness of diagnosis | Many patients unaware; address stigma early |
| Employment/income impact | Assess for disability allowance eligibility (Government of Nepal) |
| Psychological impact | Depression screen; social support system |
| Recent pregnancy (women) | Reactions common in puerperium; MDT safety counseling needed |
PART 2: CLINICAL EXAMINATION
GENERAL PRINCIPLES (IAL Textbook)
- Conduct examination in good natural light - preferably sunlight, not fluorescent (which masks subtle hypopigmentation)
- Fully expose the patient; examine the entire body surface
- Maintain patient dignity; explain each step
- Proceed in a systematic head-to-toe sequence
- Use gloves when palpating lesions
- Never skip nerve examination - per IAL Practical Manual: "Nerve examination is an integral part of assessing patients with leprosy and should never be skipped"
A. GENERAL EXAMINATION
- General appearance: Well/ill, distressed
- Nutritional status, BMI
- Vital signs (fever in ENL, Type 2 reaction)
- Lymphadenopathy: axillary, inguinal (generalized in MB/LL; also in ENL)
- Eyes: general inspection (redness, lagophthalmos visible at a glance)
- Gynecomastia (LL - testicular infiltration → elevated estrogen)
- Gait: high-stepping (foot drop - common peroneal palsy); antalgic gait
B. SKIN EXAMINATION
Step 1: Count and Map all Lesions
Total count determines WHO classification. Map lesions on a body diagram.
| Feature | TT | BT | BB | BL | LL |
|---|
| Number | 1-3 | 3-10 | Several, variable | Many | Innumerable |
| Size | Large | Large | Medium | Smaller | Small to diffuse |
| Border | Well-defined, raised | Defined outer; vague satellite | Punched-out inner/vague outer | Irregular | Ill-defined, merges |
| Surface | Dry, scaly, hairless | Dry, slightly scaly | Less dry | Shiny early | Waxy/varnished |
| Color | Hypopigmented/erythematous | Hypopig/erythematous | Mixed | Pale/erythematous | Pale macules or diffuse |
| Distribution | Asymmetric | Asymmetric | May be symmetric | Symmetric | Bilaterally symmetric |
| Anhidrosis | Marked | Moderate | Partial | Minimal | Absent late |
| Hair loss in lesion | Marked | Moderate | Variable | Minimal | Absent early |
| Central healing | Common ("saucer right-side up") | Present | Annular ("Swiss cheese") | Occasional | Absent |
| Sensation | Absent | Reduced | Moderately reduced | Mildly reduced | Late loss |
BB - "Swiss cheese" / "Punched-out" appearance: Fitzpatrick's and Dermatology 2-Volume Set (5e) describe the mid-borderline (BB) lesion as having annular plaques with a "Swiss cheese" or punched-out appearance due to holes of apparently normal skin within the lesion ring. This is characteristic of BB.
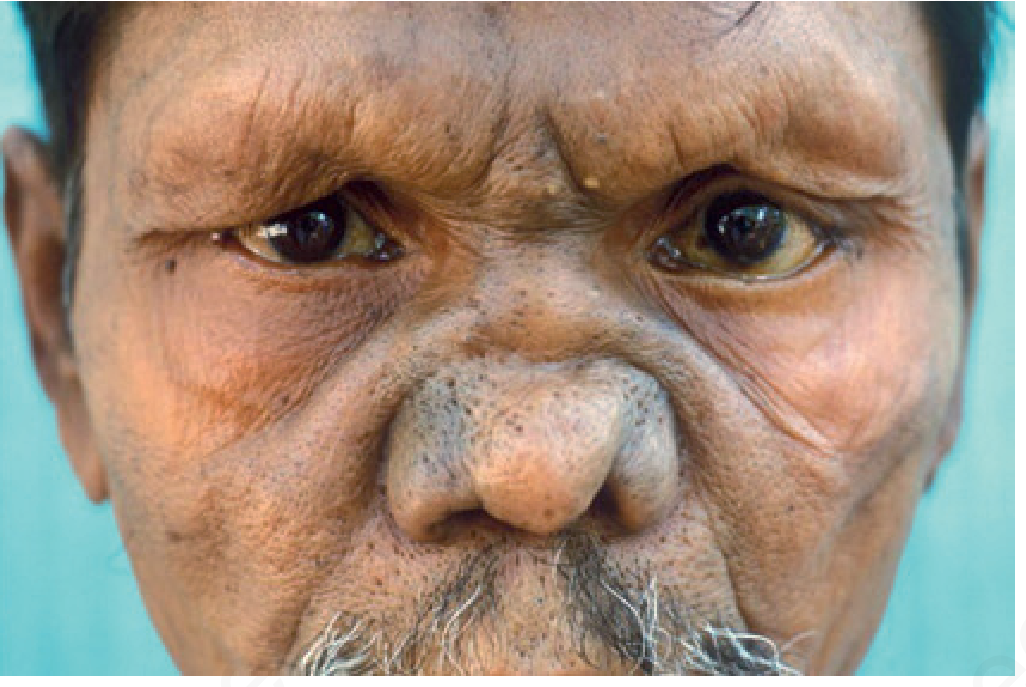
LL - "Leonine facies": Diffuse infiltration of the forehead, cheeks, earlobes, and periorbital skin creates a lion-like thickening. Also "varnished" skin appearance. - Dermatology 2-Volume Set 5e
Step 2: Immune (Spared) Sites - Always Check
The following areas are spared because M. leprae favors cooler areas:
- Scalp
- Axillae
- Groin and perineum
- Inner aspects of elbows and knees
- Dorsal midline of back (warmer, over spine)
Finding a lesion in these sites should prompt re-evaluation of the diagnosis - these are almost never affected in leprosy.
Step 3: Sensory Testing of Lesions
IAL/Park's recommended technique - Ballpoint pen test:
- Use a light ballpoint pen (plastic body, without cap)
- Explain and demonstrate to the patient while their eyes are open
- Touch normal skin first - ask patient to point to where they feel the touch (eyes open, practice)
- Ask patient to close eyes
- Touch the lesion and normal skin alternately - randomize timing and location
- Ask: "Can you feel this?" and "Where is it?" (patient points to location)
- For inaccessible areas (back, buttocks): ask patient to count each touch
Do NOT use: pins, cotton wool, feathers - these are less standardized. The ballpoint pen (Park's/IAL recommended method) gives reproducible results.
Sequence of sensory modalities to test:
- Light touch (ballpoint pen or cotton wisp)
- Temperature (hot and cold test tubes, 40°C and 5°C)
- Pain/pinprick (sterile pin)
Temperature is lost first → then light touch → then pain.
Step 4: Madarosis Assessment
- Inspect eyebrows: outer 1/3 loss first in LL (madarosis)
- Inspect eyelashes: loss later in LL
- Inspect body hair on arms/legs: gradual loss in LL
- Inspect beard area in males
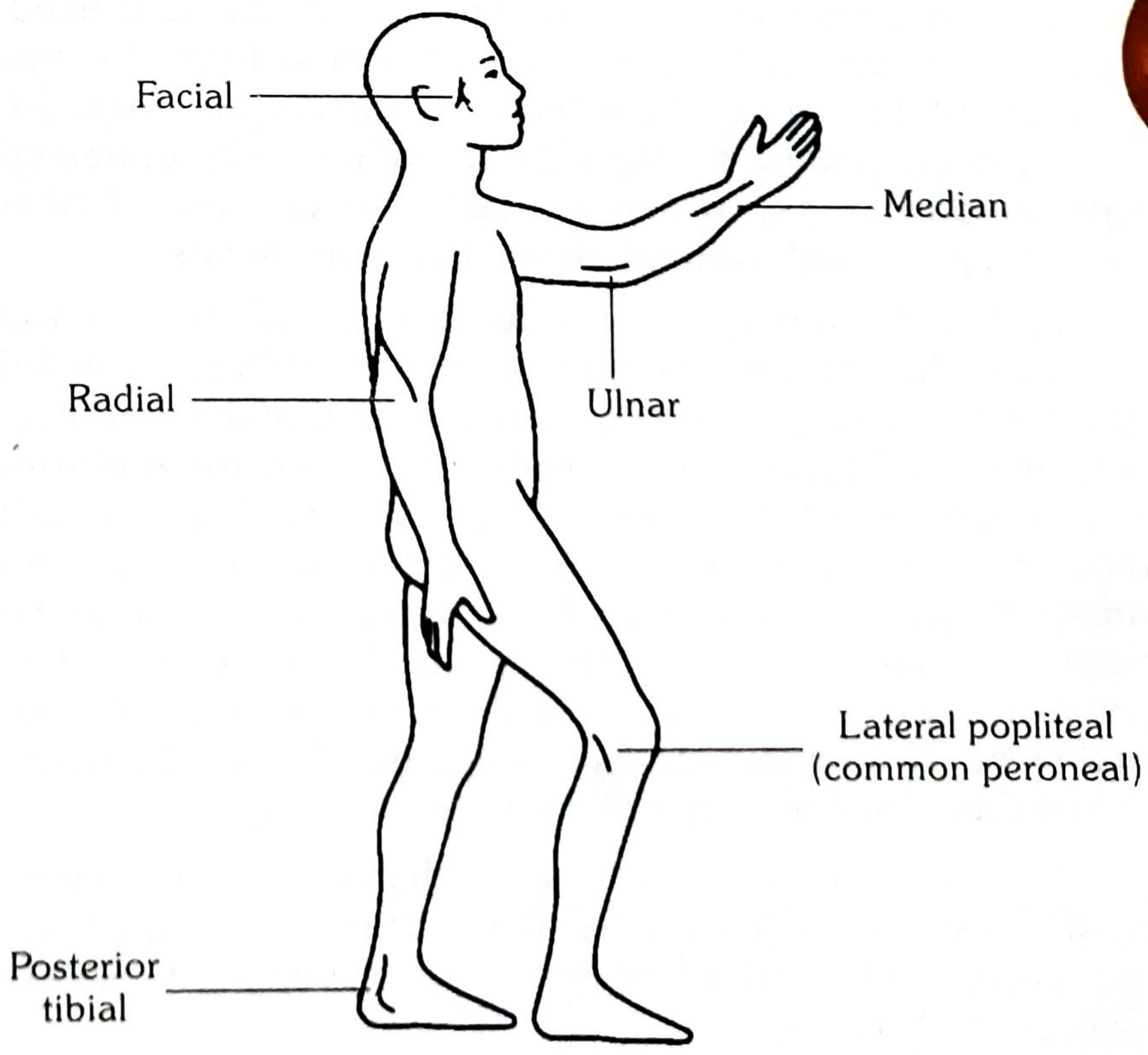
Sites of nerve involvement in leprosy. Source: Park's Textbook of Preventive & Social Medicine
C. DETAILED NERVE EXAMINATION
Per IAL Practical Manual and Park's Textbook, nerve examination has two components:
- Palpation - for thickening, tenderness, consistency
- Nerve function assessment - sensory AND motor
Technique of palpation (IAL standard):
- Use pads of index and middle fingers
- Palpate the nerve over its most superficial location for at least 5-10 cm of its length
- Detect: beading, nodularity, fusiform thickening
- Compare both sides
- Apply mild to firm pressure and watch for patient response (wincing = tenderness)
GRADING OF NERVE THICKNESS (IAL Practical Manual - 4-grade scale)
| Grade | Description |
|---|
| 0 | Normal - not thickened |
| 1 | Slightly thickened - palpable, just detectable above normal |
| 2 | Moderately thickened - clearly palpable, firm cord |
| 3 | Grossly thickened - visibly enlarged; may be beaded or nodular |
GRADING OF NERVE TENDERNESS (IAL Practical Manual - 4-grade scale)
| Grade | Description |
|---|
| 0 | No tenderness |
| 1 | Mild - slight discomfort on firm pressure |
| 2 | Moderate - obvious pain, patient verbalizes discomfort |
| 3 | Severe - patient winces, withdraws limb; spontaneous pain also present |
Clinical significance of grading: Grading nerve thickness and tenderness is used for: (a) baseline documentation, (b) communication between leprosy workers, (c) monitoring response to steroids in reactions, (d) detecting silent neuritis. A sudden increase in tenderness grade signals acute neuritis - requires urgent steroid intervention.
NERVE-BY-NERVE EXAMINATION
1. GREAT AURICULAR NERVE (GAN)
Course: Emerges from C2-C3 root, winds around the posterior border of the SCM, runs obliquely across the surface of the muscle upward toward the parotid gland and auricle. Supplies sensation to the parotid region, angle of mandible, and earlobe.
Palpation:
- Ask patient to turn head to the opposite side - this tightens the SCM and makes the GAN more prominent
- Palpate the posterior surface of the SCM at the junction of upper and middle third
- The nerve runs obliquely (posteroinferior to anterosuperior) across the SCM surface
- Normal: barely palpable or impalpable
- Abnormal: firm cord, may be nodular, beaded, visibly enlarged
Sensory test: Skin over angle of jaw, parotid area, earlobe - light touch and temperature
Clinical pearl (IAL): GAN is the most commonly visibly enlarged nerve in leprosy. Its enlargement is almost pathognomonic when accompanied by a skin lesion. It can be enlarged in TT, BT, and sometimes LL.
2. SUPRA-ORBITAL NERVE (Branch of V1, Trigeminal)
Course: Exits through supra-orbital notch/foramen at the superior orbital rim, approximately at the mid-pupillary line (junction of medial and middle thirds of supraorbital rim).
Palpation: Palpate along the entire superior orbital rim for tenderness and any nodular thickening at the notch.
Sensory test: Touch the forehead and anterior scalp - compare both sides.
Motor (associated facial nerve): Zygomatic branch supplies orbicularis oculi - test separately (see below).
3. FACIAL NERVE
Course: Exits stylomastoid foramen, enters parotid gland, and divides into:
- Temporal branch: Frontalis (forehead wrinkling), upper orbicularis oculi
- Zygomatic branch: Orbicularis oculi (lower, eye closure) - most affected in leprosy
- Buccal branch: Orbicularis oris, zygomaticus, nasalis
- Marginal mandibular branch: Depressor anguli oris
- Cervical branch: Platysma
Palpation: Not routinely palpable; assess by function.
Motor testing (sequence):
- Eye closure (lagophthalmos test): Ask patient to close eyes gently. Observe gap between lids - measure in mm. Check Bell's phenomenon (eye rolls upward when patient tries to close; protective reflex - if absent, corneal risk is even higher).
- Forceful eye closure: Ask to close eyes tightly - assesses residual orbicularis oculi function.
- Forehead wrinkling: Ask to raise eyebrows - temporal branch.
- Smile and show teeth: Buccal/zygomatic.
- Puff cheeks: Buccal branch.
- Lower lip depression: Marginal mandibular.
IAL/WHO grading for eye closure:
- Grade 0: Complete eye closure (normal)
- Grade 1: Incomplete closure - gap <3mm (monitor)
- Grade 2: Gap >3mm with corneal exposure (disability grade 2 if corneal damage)
Associated trigeminal (V1) test: Corneal reflex - touch cornea gently with cotton wisp from the side. Response = blink. Absent/reduced corneal reflex (V1 damage) + lagophthalmos (VII damage) = catastrophic combination for corneal ulceration.
4. ULNAR NERVE
Course: Medial cord of brachial plexus (C8, T1). Passes medially down arm, enters the ulnar groove posterior to the medial epicondyle (cubital tunnel), passes between heads of flexor carpi ulnaris (FCU), runs down medial forearm with ulnar artery, passes through Guyon's canal at the wrist, divides into superficial (sensory) and deep (motor) branches.
Most common site of leprosy involvement: The nerve as it passes through the cubital tunnel (cool, superficial, mechanical pressure point).
Palpation (primary site):
- Patient's elbow flexed to 90-110° (this opens the cubital tunnel and makes the nerve more palpable)
- Palpate in the groove between medial epicondyle and olecranon
- Roll the nerve gently against the bony floor
- Then palpate proximally up the medial upper arm along the medial intermuscular septum
Motor testing - Ulnar nerve:
- Claw hand test: Ask patient to straighten all fingers. Ulnar claw = inability to fully extend ring (4th) and little (5th) fingers at IP joints (due to loss of 3rd and 4th lumbricals).
- Card test (interosseous test): Place card between adjacent fingers; patient holds it while you pull. Weakness of interossei = card slides out easily.
- Froment's sign: Hold a piece of paper between thumb and index finger; patient grips while examiner pulls. If adductor pollicis (ulnar) is weak, the thumb IP joint flexes (FPL compensates) = positive Froment's sign.
- Little finger abduction: Ask to spread little finger out (abductor digiti minimi - ulnar).
- Inspect for interosseous guttering (dorsum of hand between metacarpals) and hypothenar wasting.
Sensory testing:
- Medial 1.5 fingers: little finger + medial half of ring finger (dorsal and palmar)
- Medial border of hand
- Use ballpoint pen or monofilament
5. MEDIAN NERVE
Course: C5-T1, lateral and medial cords. Runs medial to brachial artery, enters cubital fossa medial to biceps tendon, passes between pronator teres heads, runs between FDS and FDP, passes through carpal tunnel under flexor retinaculum. Divides into recurrent motor branch (thenar muscles) and common/proper digital sensory branches.
Site most affected in leprosy: Carpal tunnel (at wrist).
Palpation:
- At the wrist: palpate medial to FCR tendon, lateral to palmaris longus, at the proximal wrist crease
- Can also be palpated in the mid-forearm between FDS and FDP
Motor testing:
- Thumb abduction (APB test): Ask patient to point thumb perpendicular to the palm (toward ceiling). Resist downward pressure. Weakness/absence = thenar wasting from median palsy.
- Pen cap test / "OK sign": Weakness of FPL and FDP index (anterior interosseous nerve) causes inability to make a circle; patient makes a rectangular/rectangular pinch instead.
- Bottle sign: Cannot fully oppose thumb and index around a cylindrical bottle.
- Inspect thenar eminence for wasting (flattening = "ape hand" when combined with thenar + hypothenar wasting).
Sensory testing:
- Radial 3.5 fingers: thumb, index, middle, radial half of ring (dorsal and palmar distal)
- Thenar eminence (palmar cutaneous branch - outside carpal tunnel)
6. RADIAL NERVE (Superficial/Cutaneous Branch)
Course: The superficial (sensory) branch of the radial nerve leaves the main trunk approximately 8-10 cm above the wrist, passes deep to brachioradialis, emerges at the lateral forearm to supply the dorsum of the radial 3.5 fingers and dorsal thenar area.
Palpation site:
- Radial aspect of the distal forearm, just lateral to the radial artery at the wrist
- Palpate under the brachioradialis tendon, rolling the nerve over the radial styloid
Motor testing (if main radial trunk involved - less common in leprosy):
- Wrist extension, finger extension, thumb extension
- Wrist drop if radial nerve proper is involved
Sensory testing:
- Dorsum of first web space (between thumb and index) - most reliable
- Dorsal thumb and radial 3.5 fingers
7. COMMON PERONEAL NERVE (Lateral Popliteal Nerve)
Course: Branch of the sciatic nerve. Passes from the posterior knee, winds around the neck of the fibula (very superficial here - most vulnerable to leprosy), pierces the peroneus longus, divides into:
- Deep peroneal: Tibialis anterior, extensor digitorum longus, extensor hallucis longus; sensory: first web space of foot
- Superficial peroneal: Peroneus longus and brevis; sensory: dorsum of foot
Palpation:
- Stand behind/beside the patient
- Identify the fibular head (prominent bony prominence on lateral knee)
- The nerve wraps around the neck of the fibula, approximately 2-3 cm below the fibular head on the posterior-lateral aspect
- Roll the nerve against the fibula - it should feel like a cord crossing the bone
- Palpate both distally (as it enters lateral compartment) and posteriorly (in the popliteal fossa above the fibular head)
Motor testing:
- Foot drop: Ask patient to walk; look for high-stepping gait and slapping of foot
- Dorsiflexion: "Pull your toes and foot up toward your shin" against resistance - tests tibialis anterior (deep peroneal)
- Toe extension: Extend toes against resistance - extensor digitorum longus
- Eversion: "Turn your foot outward (sole faces out)" against resistance - peroneus longus and brevis (superficial peroneal)
Sensory testing:
- Dorsum of foot (superficial peroneal)
- First web space (deep peroneal)
8. POSTERIOR TIBIAL NERVE
Course: Terminal branch of the tibial nerve. Passes behind the medial malleolus with the posterior tibial artery, through the tarsal tunnel (under flexor retinaculum), divides into medial plantar, lateral plantar, and calcaneal branches.
Memory aid for structures behind medial malleolus (anterior to posterior):
"Tom, Dick and Harry" = Tibialis posterior → flexor Digitorum longus → posterior tibial Artery and Nerve → flexor Hallucis longus
Palpation:
- Find the medial malleolus
- Palpate the groove between the medial malleolus and the Achilles tendon
- The nerve lies posterior to the pulsating posterior tibial artery
- Roll the nerve gently; it is softer and less prominent than the artery
Motor testing:
- Intrinsic foot muscles (abductors/flexors of toes): Ask patient to flex and spread toes
- Observe for claw toes (intrinsic minus foot)
- Plantar flexion (S1 primarily, but tibial nerve contributes)
Sensory testing:
- Entire plantar surface of the foot (medial and lateral plantar nerves)
- Medial and lateral toes (plantar aspect)
- Heel (medial calcaneal branch)
Clinical significance: Posterior tibial nerve damage = loss of plantar sensation = painless plantar ulcers - the most common cause of morbidity and limb loss in leprosy. Per IAL Practical Manual, this is why regular plantar sensory testing is mandatory.
9. SURAL NERVE
Course: Purely sensory; formed by medial sural cutaneous nerve (from tibial) and peroneal communicating branch (from common peroneal). Runs subcutaneously along the lateral border of the Achilles tendon to the lateral malleolus and lateral foot.
Palpation: Along the lateral border of the Achilles tendon, approximately 3-5 cm proximal to the lateral malleolus.
Sensory test: Lateral aspect of foot and little toe.
Significance: The sural nerve is the most commonly biopsied nerve in leprosy for nerve biopsy specimens (accessible, purely sensory = no motor deficit from biopsy). Enlargement with lateral foot anesthesia points to sural nerve leprosy.
NERVE FUNCTION ASSESSMENT - QUICK CLINICAL PROTOCOL
Per WHO/IAL standard for field and clinic use, test these 4 key motor functions and 3 sensory areas:
Motor (4 nerves - WHO minimum):
- Facial nerve: Eye closure (complete/incomplete)
- Ulnar nerve: Little finger abduction (spread 5th finger out)
- Median nerve: Thumb abduction (point thumb up from palm)
- Common peroneal (lateral popliteal): Foot dorsiflexion (pull toes up)
Sensory (3 areas):
- Ulnar and median sensory territory in hand (palmar surface at little finger and index finger)
- Plantar surface of foot (posterior tibial territory)
- Over skin lesions (using ballpoint pen)
Grade each as: Normal / Impaired / Absent.
D. EYE EXAMINATION
Systematic, urgent - leprosy is a leading preventable cause of blindness:
- Visual acuity - Snellen chart; finger counting if severe
- Lagophthalmos - measure gap in mm; test Bell's phenomenon
- Cornea - clarity (ulcer, scarring, pannus); corneal anesthesia (V1 testing with cotton wisp from lateral approach)
- Iris/pupil - irregular pupil, posterior synechiae, Koeppe nodules (iris lepromas), constricted/sluggish pupil
- Conjunctiva - perilimbal injection (ciliary flush in iritis); tarsal nodules
- Sclera - scleritis (ENL)
- Eyelids - madarosis (loss of brows/lashes), ectropion/entropion
E. NOSE AND THROAT EXAMINATION
- Nose: Saddle deformity (nasal bridge collapse - septal destruction in LL), nostril atrophy, epistaxis
- Throat: Hoarseness (laryngeal leprosy - LL), palpate neck for GAN
F. HAND AND FOOT EXAMINATION
Hands:
- Inspect dorsum: claw (ulnar/combined), wrist drop (radial), interosseous guttering, trophic changes
- Inspect palm: thenar and hypothenar wasting, callus, fissures, trophic ulcers
- Test all digits for sensation
- Assess grip strength
Feet:
- Inspect dorsum: foot drop, trophic changes, digital deformities
- Inspect sole: plantar ulcers (at pressure points - metatarsal heads, heel, ball of foot); callus, fissures
- Assess plantar sensation (posterior tibial territory)
- Check pulses
PART 3: INVESTIGATIONS (SEQUENCE AND SIGNIFICANCE)
INVESTIGATION 1: SLIT-SKIN SMEAR (SSS)
Sites (IAL recommended): Both earlobes (× 2), both active lesion edges (× 2), chin, forehead = minimum 4-6 sites for MB; for PB, may include only active lesion edge and earlobes.
Technique (step-by-step):
- Clean site with spirit, allow to dry completely
- Pinch skin firmly between thumb and forefinger to blanch - reduces bleeding and concentrates tissue fluid
- Make a 5mm incision, 2-3mm deep (dermis only)
- Scrape incision walls firmly 3-4 times with the blade edge
- Spread material as a uniform circular smear (5-7mm diameter) on a grease-free glass slide
- Air-dry, fix with methanol
- Stain: Fite-Faraco (preferred) or modified ZN (5% H₂SO₄)
- Examine 100 oil-immersion fields (100×)
Reading:
- Bacillary Index (BI): Ridley's scale 0-6+ (log scale)
- Morphological Index (MI): % solid-staining (viable) bacilli
BI drops ~1 unit per year on effective MDT. Rising BI after release from treatment = relapse.
Per Dermatology 2-Volume Set (5e): Organisms found in 100% LL patients, 75% borderline, only 5% TT. For tuberculoid-suspected lesions, examine at least 6 histology sections before declaring negative.
INVESTIGATION 2: SKIN BIOPSY & HISTOPATHOLOGY
IAL recommendation for biopsy:
- From the most active, representative lesion
- Include the active edge (not the healed center)
- Full-thickness punch biopsy (4-6mm) to subcutaneous fat
- Request Fite-Faraco + H&E + S-100 stain
Why Fite-Faraco over ZN? - Dermatology 2-Volume Set (5e): "Fite-Faraco stain is more sensitive; Ziehl-Neelsen stain may also stain bacilli red, but is less reliable for M. leprae due to incomplete preservation of staining."
Histopathological Findings by Type (Ridley-Jopling):
| Type | Granuloma | Giant cells | Grenz zone | AFB | Nerves |
|---|
| TT | Well-formed epithelioid; lymphocytes at periphery | Langhans' (prominent) | Absent - reaches epidermis | None/rare | Destroyed (perineural concentric fibrosis - S100 shows remnants) |
| BT | Similar to TT but less mature epithelioid cells | Present, fewer | Narrow but present | Rare | Grossly swollen nerve bundles; intraneural granuloma |
| BB | Ill-defined; immature epithelioid cells | Absent | Present | Moderate | Not prominently swollen |
| BL | Foamy histiocytes predominant; lymphocytes dispersed | Absent | Present | Abundant; clumps | Perineural lymphocytic infiltration |
| LL | Virchow foam cells; lipid-laden, bacilli-laden macrophages | Absent | Wide, prominent | Globi (6+) | Laminated onion-skin perineurium |
| Histoid | Spindle cells (histiocytes) in whorls/storiform pattern | Absent | Absent | Very abundant (bacilli along spindle cell long axis) | Variable |
| Indeterminate | Non-specific lymphohistiocytic; no granuloma | Absent | Variable | None/rare | Perineural mononuclear infiltrate |
Jopling's original description (1966): In TT, "foci of well-developed epithelioid cells with or without Langhans giant cells, encompassed by a zone of dense lymphocyte infiltration. The granuloma extends up to the epidermis without a subepidermal zone." In BT, "the best point of distinction is that there is a clear subepidermal zone, although it may be very narrow."
INVESTIGATION 3: LEPROMIN (MITSUDA) TEST
Preparations:
- Dharmendra antigen (integral, heat-killed suspension) - more standardized
- Mitsuda antigen (crude, from infected tissue)
Technique:
- Inject 0.1 mL intradermally into the flexor forearm
- Fernandez reaction: Read at 48 hours - erythema and induration (measures sensitization similar to tuberculin)
- Mitsuda reaction: Read at 28 days - papule/nodule (measures granuloma-forming CMI capacity)
Mitsuda interpretation:
| Result | Induration | Spectrum |
|---|
| Strongly positive (+++) | >10mm, may ulcerate | TT - maximal CMI |
| Strongly positive (++) | 5-10mm firm nodule | BT - good CMI |
| Positive (+) | 3-5mm | BB - moderate CMI |
| Weakly positive/negative | <3mm | BL |
| Strongly negative | No reaction | LL - absent CMI |
NOT a diagnostic test - positive in BCG-vaccinated individuals and TB contacts. It is a prognostic and classification tool (Jopling).
IAL note: The Mitsuda reaction is used in India and Nepal for classification in ambiguous cases and for research; it is not routinely performed at district health facilities.
INVESTIGATION 4: SENSORY TESTING (FORMAL)
Semmes-Weinstein Monofilament Test (SWMT):
Standard monofilaments (2g for hand, 10g for foot) applied until bending. Maps sensory loss areas precisely. The WHO recommends monofilament testing for all leprosy patients at diagnosis and every 3 months during MDT.
Ballpoint pen test (IAL/Park's): See examination section above.
Hot-Cold tubes: Formal temperature discrimination - especially important as it is the first modality lost.
INVESTIGATION 5: VOLUNTARY MUSCLE TESTING (VMT)
Graded per MRC scale (0-5) for all key muscles. Documented on a standard VMT chart:
Minimum set to test (WHO/IAL):
- Orbicularis oculi (facial/zygomatic)
- APB = Abductor pollicis brevis (median)
- ADM = Abductor digiti minimi + 1st dorsal interosseous (ulnar)
- Tibialis anterior (common peroneal)
- EHL = Extensor hallucis longus (deep peroneal)
Documented at: diagnosis, monthly during MDT, at completion, and at each follow-up.
INVESTIGATION 6: WHO DISABILITY GRADING
| Grade | Eyes | Hands | Feet |
|---|
| 0 | No problem due to leprosy | No anesthesia, no deformity | No anesthesia, no deformity |
| 1 | Eye problems due to leprosy but vision not severely affected (VA ≥6/60); no lagophthalmos | Anesthesia present but NO visible deformity | Anesthesia present but NO visible deformity |
| 2 | Severe visual impairment (VA <6/60) OR lagophthalmos, corneal disease | Visible deformity/damage (claw, wrist drop, absorption of digits, ulcer) | Visible deformity/damage (foot drop, claw toes, plantar ulcer, absorption of digits) |
Nepal NLS 2021-2025: New Grade 2 Disability (G2D) at diagnosis is a key program indicator. Nepal recorded 95 new G2D cases in FY 2020/21 - a measure of late case detection.
INVESTIGATION 7: ADDITIONAL INVESTIGATIONS
| Test | Indication | Significance |
|---|
| CBC | Before MDT | Dapsone → hemolytic anemia; clofazimine → GI changes |
| G6PD levels | Before dapsone, especially in male patients | G6PD deficiency → severe hemolysis with dapsone |
| LFTs | Before and during MDT | Rifampicin hepatotoxicity |
| RFTs | Baseline | Relevant for drug dosing |
| Blood glucose | All patients | Diabetic neuropathy as co-morbidity/differential |
| Nerve conduction study (NCS/EMG) | Pure neural leprosy; ambiguous neuropathy | Documents large-fiber neuropathy; useful in reactions - Fitzpatrick's 9th ed. |
| High-resolution ultrasound (HRUS) of nerves | Pure neural leprosy; nerve abscess suspicion | Enlargement pattern; nerve cross-sectional area; vascularity [PMID 41773898] |
| MRI neurography | Proximal nerve involvement assessment | Shows nerve enlargement, increased T2 signal, nodular enhancement |
| PCR for M. leprae | PB/pure neural/indeterminate with negative SSS and biopsy | Positive in ~50% PB; higher in MB; reference centers |
| Anti-PGL-1 antibody | Research/contact screening | >90% positive in LL; ~50% TT; poor PB sensitivity |
| CXR | Baseline before rifampicin | Rule out TB co-infection |
| Slit-lamp examination | ENL/suspected iritis | Posterior synechiae, Koeppe nodules, iris lepromas |
PART 4: DIFFERENTIAL DIAGNOSIS
(See previous comprehensive table; additional IAL-referenced differentials:)
Maculoanesthetic leprosy (IAL category) vs. Vitiligo:
IAL groups maculoanesthetic leprosy with TT. The key distinguishing feature from vitiligo: maculoanesthetic patches have impaired sensation and may have subtle nerve thickening. Vitiligo is chalk-white depigmentation (not just hypopigmentation), normal sensation, and normal nerve examination.
Post-kala-azar dermal leishmaniasis (PKDL) - Nepal-specific differential:
PKDL is endemic in Nepal's Terai (Province 2 - same as leprosy hotspot). Presents with hypopigmented macules and nodules. Distinguishing: NO nerve involvement, NO sensory loss; skin smear/biopsy shows Leishmania amastigotes; history of prior kala-azar. This differential is especially important in Province 2.
Mycosis Fungoides (Hypopigmented variant):
Hypopigmented patches; may have mild hypoesthesia confusing clinicians; biopsy shows Pautrier microabscesses and CD8+ T-cell epidermotropism. No nerve thickening.
PART 5: MANAGEMENT AS PER NEPAL GUIDELINES
(Updated with IAL/WHO 2024 guidance)
A. CLASSIFICATION AND TREATMENT
Nepal follows WHO classification for treatment decisions aligned with the National Leprosy Strategy 2021-2025.
Key update (2023-2025): WHO now recommends uniform 3-drug MDT for both PB and MB cases (previously PB received only 2 drugs). Nepal's National Program is implementing this. The only difference is duration (6 months vs. 12 months).
MDT Regimens - Nepal/WHO (Current):
PAUCIBACILLARY (PB) - 6 months
| Drug | Adult | Child (10-14 yr) | Child (<10 yr or <40 kg) | Route |
|---|
| Rifampicin | 600 mg once monthly (supervised) | 450 mg once monthly | 10 mg/kg monthly | Oral |
| Dapsone | 100 mg daily | 50 mg daily | 2 mg/kg/day | Oral |
| Clofazimine | 300 mg monthly + 50 mg daily | 150 mg monthly + 50 mg alt. days | 100 mg monthly + 50 mg twice weekly | Oral |
MULTIBACILLARY (MB) - 12 months
| Drug | Adult | Child (10-14 yr) | Child (<10 yr or <40 kg) | Route |
|---|
| Rifampicin | 600 mg once monthly (supervised) | 450 mg once monthly | 10 mg/kg monthly | Oral |
| Clofazimine | 300 mg monthly + 50 mg daily | 150 mg monthly + 50 mg alt. days | 6 mg/kg/month + 1 mg/kg/day | Oral |
| Dapsone | 100 mg daily | 50 mg daily | 2 mg/kg/day | Oral |
MDT is free at all public health facilities in Nepal. Drugs come pre-packed in color-coded blister packs (maroon for MB, brown for PB).
B. MANAGEMENT OF REACTIONS
Jopling's principle: "Reactions are a common reason why patients seek consultation. If a patient believes the chemotherapy is triggering the reaction, the patient will tend to discontinue treatment, leading to treatment failure." MDT must NEVER be stopped.
Type 1 (Reversal) Reaction
- Prednisolone 40-60 mg/day (1 mg/kg/day), minimum 6-month tapering course
- Starting dose: 40 mg/day for 2 weeks, then gradually taper (reduce by 5 mg every 2-4 weeks based on response)
- Steroid-sparing: methotrexate 7.5-15 mg/week if prolonged course or steroid dependence
- Analgesics for nerve pain
- Splint affected limb in acute neuritis (prevents contracture)
- Continue MDT throughout
Type 2 (ENL) Reaction
- Mild: NSAIDs + chloroquine 300 mg/day
- Moderate-severe: Prednisolone 40-60 mg/day (shorter taper than Type 1, typically 4-8 weeks)
- Severe/recurrent/chronic ENL: Thalidomide 100-400 mg/day (start at 400 mg for 4 days, taper; NOT in women of childbearing age)
- Clofazimine 300 mg/day (anti-inflammatory in ENL; takes 4-6 weeks; reduces steroid dependence in chronic ENL)
- Treat orchitis: bed rest, scrotal support, NSAIDs
- Iritis: Urgent ophthalmology + topical prednisolone + atropine
- Continue MDT throughout
Silent Neuritis
IAL Textbook emphasizes: Silent neuritis (nerve function impairment without pain or active reaction) must be detected by regular VMT/sensory testing - it is managed the same way as overt neuritis with prednisolone.
C. DISABILITY PREVENTION AND SELF-CARE (Nepal Program)
Per Nepal National Leprosy Strategy 2021-2025 Pillar 3:
- Eye care: Artificial tears 4-6 times/day; protective glasses; visual inspection daily
- Hand care: Warm water soaking + oil massage (prevents dryness from clofazimine); wound inspection daily; protective gloves for hot objects
- Foot care: Custom molded footwear; daily plantar inspection with a mirror; no barefoot walking
- Wound management: Regular debridement + dressings for plantar ulcers; complete offloading
- Physiotherapy: Active and passive exercises; splinting for acute neuritis
- Reconstructive surgery: Tendon transfers for claw hand (NLEP programs in Nepal); tarsal tunnel decompression; nerve abscess drainage
D. CONTACT MANAGEMENT - SDR-PEP (Nepal 2021-25 Strategy)
- Screen all household and close contacts
- Eligible contacts receive Single Dose Rifampicin (SDR-PEP):
- Adults: 600 mg single oral dose
- Children 6-14 years: 450 mg single oral dose
- Children 2-5 years: 150-300 mg single oral dose
- Exclude: Active TB, already on rifampicin, rifampicin allergy, children <2 years
- Efficacy: ~57% risk reduction in contacts
- Register in Nepal's Nikusth online platform
- Re-screen contacts annually for 5 years
E. FOLLOW-UP
- Monthly: supervised rifampicin; examine for reactions, new lesions; dispense daily drugs
- VMT/sensory testing: every 3 months during MDT; at completion
- Disability grading: at diagnosis and completion
- Post-treatment: MB every 6-12 months for 5 years; PB for 2 years
- BI monitoring: 6 monthly in MB (should fall ~1 unit/year)
PART 6: VIVA QUESTIONS & QUIZ (IAL/Jopling-Integrated)
VIVA QUESTIONS
Q1. What were the original criteria used by Ridley and Jopling (1966) to classify leprosy into 5 groups?
A: Ridley and Jopling (Int J Lepr, 1966;34(3):255-273) defined five groups based on four parameters simultaneously assessed:
- Clinical: Number, size, distribution, and character of skin lesions; nerve involvement pattern
- Bacteriological: Bacillary Index (BI) from SSS/biopsy; Morphological Index (MI)
- Immunological: Lepromin (Mitsuda) test result at 28 days
- Histopathological: Nature and organization of granuloma; presence/absence of grenz zone; nerve involvement pattern; giant cells
The key insight of Ridley-Jopling was that these four parameters correlate with each other because they are all driven by the same underlying variable: the host's cell-mediated immunity (CMI) against M. leprae. The classification is therefore an immune spectrum.
Q2. How does the IAL (New Indian) classification differ from Ridley-Jopling?
A: The New Indian Classification (IAL, 1981) simplifies R-J by:
- Consolidating borderline groups BT + BB + BL → single "Borderline (B)" category
- Including maculoanesthetic leprosy within tuberculoid (T) - previously a separate category in the older Indian classification (Madrid, 1953)
- Formally recognizing Polyneuritis (P) as a separate category = pure neuritic leprosy without skin lesions
- Adding Indeterminate (I) as a starting point
The 5 IAL groups: I (Indeterminate), T (Tuberculoid), B (Borderline), L (Lepromatous), P (Polyneuritis).
This classification is practical for field and clinic use in India and Nepal where simplified grouping is needed, but the R-J system remains the gold standard for research, reactions monitoring, and detailed clinical classification.
Q3. What is the significance of the "unstable" nature of the borderline group in Jopling's classification?
A: Jopling emphasized that borderline leprosy (BT, BB, BL) is immunologically unstable - patients in this spectrum can shift in either direction along the immune spectrum:
- Upgrading (toward TT): Increasing CMI - causes Type 1 (Reversal) reaction. The sudden increase in CMI leads to inflammatory destruction of existing lesions and nerves. This is the mechanism of reversal reaction and is most severe in BL patients (greatest antigen load during upgrading).
- Downgrading (toward LL): Decreasing CMI (due to continued antigen exposure, malnutrition, immunosuppression) - causes downgrading reaction (clinically similar to reversal).
The two polar forms (TT and LL) are stable - they rarely undergo reactions or shift in spectrum. This is why monitoring and steroid treatment is most important in borderline patients.
Q4. What are the classic nerve deformities produced by each nerve in leprosy? List the nerve and its deformity.
A:
| Nerve | Deformity |
|---|
| Ulnar | Claw hand (4th and 5th fingers); interosseous wasting; hypothenar wasting |
| Median | Ape thumb deformity (thenar wasting; thumb falls into same plane as fingers); loss of opposition |
| Ulnar + Median combined | Complete claw hand (all 4 fingers); combined thenar + hypothenar wasting |
| Radial | Wrist drop (extensor weakness) |
| Facial (zygomatic branch) | Lagophthalmos (inability to close eye) → corneal ulcer → blindness |
| Common peroneal (lateral popliteal) | Foot drop; high-stepping gait |
| Posterior tibial | Loss of plantar sensation → plantar ulcers; claw toes; intrinsic foot muscle wasting |
Q5. Explain the bacteriological and morphological indices and how they help in monitoring leprosy treatment.
A:
- Bacillary Index (BI): Ridley's 0-6+ logarithmic scale measuring density of AFB in SSS. Used to confirm MB leprosy at diagnosis; monitor bacteriological response. BI falls approximately 1 unit per year on effective MDT. A BI that fails to fall or rises = drug resistance or relapse.
- Morphological Index (MI): Percentage of solid-staining (intact) bacilli - represents viable, infective organisms. Normal bacteria stain solid; dead or dying bacteria fragment and stain as beaded/granular. On effective MDT, MI drops to zero within weeks to months - first evidence of bacteriological response. Rising MI (especially >1%) after apparent cure = relapse, often with drug-resistant organisms.
Combined monitoring: MI detects early treatment response; BI detects slow clearance and relapse.
Q6. A patient with leprosy develops sudden wrist drop, claw hand, and foot drop overnight during treatment. What is happening and what is the emergency management?
A: This is acute neuritis in the context of a Type 1 (Reversal) Reaction - a dermatological and neurological emergency. The sudden immune attack on nerves can cause irreversible damage within hours if untreated.
Immediate management:
- Do NOT stop MDT
- Prednisolone 1 mg/kg/day (40-60 mg) orally - START IMMEDIATELY - every hour of delay increases risk of permanent nerve damage
- Splint the affected limb in functional position to prevent contracture (wrist in neutral/slight dorsiflexion; foot in 90° dorsiflexion)
- Analgesia for nerve pain
- Admit if bilateral, severe, or if corneal exposure
- Arrange urgent ophthalmology if lagophthalmos
- Taper prednisolone slowly over minimum 6 months
- Document VMT baseline; repeat every 2 weeks
Per IAL Textbook: "Reactions should be treated aggressively to prevent peripheral nerve damage. The goal is to reverse any nerve function impairment."
Q7. What are the lepromin test results across the R-J spectrum and why does this occur?
A:
| Type | Mitsuda (28-day) result | Reason |
|---|
| TT | +++/++ (>5mm, may ulcerate) | Maximum CMI; robust granuloma-forming capacity; IFN-γ and IL-2 dominant |
| BT | ++/+ (3-10mm) | Good CMI |
| BB | ± (weakly positive or negative) | Moderate CMI |
| BL | Negative | Poor CMI |
| LL | Strongly negative | Absent CMI to M. leprae; IL-4/IL-5/IL-10 (Th2) dominant; macrophages cannot kill bacilli |
Key point (Jopling): The lepromin test is NOT a diagnostic test - it is a measure of CMI status and helps classify ambiguous cases along the spectrum. It is also positive in BCG-vaccinated individuals and TB-infected individuals, making it non-specific for diagnosis.
Q8. What is the "immune privilege" concept in leprosy and which body sites are spared?
A: M. leprae has an optimal growth temperature of 30-32°C (below core body temperature). It therefore grows preferentially in cooler areas of the body. Areas that are relatively warmer due to proximity to major vessels, hair insulation, or body folds are spared.
Spared "immune privileged" sites (warm areas):
- Scalp
- Axillae
- Groin and perineum
- Inner aspects of elbows and knees
- Mid-back (over spine)
- Webspaces of toes (in early disease)
Sites commonly affected (cool areas):
- Face, ears, earlobes (especially LL)
- Buttocks, upper arms, thighs
- Hands, feet
Q9. Describe the histoid leprosy - its clinical features, histopathology, and significance.
A: Histoid leprosy is an atypical form of multibacillary (LL) leprosy, first described by Wade (1963). It most commonly occurs:
- After dapsone monotherapy with resistance (hence called "histoid" due to histiocyte spindle cell pattern)
- After irregular/incomplete MDT
- Occasionally de novo
Clinical features:
- Firm, shiny, dome-shaped papules and nodules (1-15mm)
- Yellow-red to skin-colored
- Appear on normal background skin (unlike regular LL where skin is diffusely infiltrated)
- Favor buttocks, lower back, face, bony prominences
- May resemble dermatofibromas or molluscum contagiosum
Histopathology (pathognomonic):
- Spindle-shaped histiocytes arranged in whorls, storiform pattern, or tight circles
- Bacilli extremely abundant, aligned along the long axis of spindle cells
- BI 6+ (maximum)
- Solid-staining bacilli (high MI) - indicates viable, potentially drug-resistant organisms
- Distinct from surrounding tissue
Significance:
- High bacillary load → highly infectious
- Suggests dapsone resistance → test MI and folP1 gene mutation
- Treat with full MB-MDT; if dapsone resistant, use alternative regimen (Rifampicin + Ofloxacin + Minocycline - ROM)
Q10. What is Lucio phenomenon and how does it differ from ENL?
A: Both are reactional states in LL, but they are distinct:
| Feature | ENL (Type 2) | Lucio Phenomenon |
|---|
| Form of leprosy | BL/LL (any subtype) | Diffuse Lepromatous Leprosy (Lucio leprosy = non-nodular, diffuse form) |
| Geographic distribution | Global | Mainly Mexico and Central America |
| Mechanism | Immune complex-mediated (Type III) | Endarteritis obliterans with vascular occlusion and necrosis |
| Skin lesions | Tender red nodules (ENL) on normal skin | Irregular hemorrhagic infarcts; angular punched-out ulcerations on extremities |
| Systemic features | Fever, arthralgia, orchitis common | Severe; high mortality |
| Histology | Neutrophilic infiltrate; leukocytoclastic vasculitis with AFB | Endothelial proliferation and thrombus in dermal vessels; bacilli inside endothelial cells |
| Treatment | Prednisolone/thalidomide | Difficult; may need wound care, antibiotics; MDT |
MCQ QUIZ (IAL/Jopling Additions)
Q1. The Ridley-Jopling classification was published in which journal and year?
- A) Lancet, 1962
- B) Int J Leprosy, 1966
- C) BMJ, 1970
- D) JAMA, 1968
Answer: B. Ridley DS, Jopling WH. Classification of leprosy according to immunity. A five-group system. Int J Lepr. 1966;34(3):255-273. The preliminary version was published in Lepr Rev 1962 but the definitive 5-group paper appeared in 1966.
Q2. In the IAL New Indian Classification (1981), pure neuritic leprosy without skin lesions falls under which group?
- A) Indeterminate (I)
- B) Tuberculoid (T)
- C) Borderline (B)
- D) Polyneuritis (P)
Answer: D - Polyneuritis (P). This is the unique contribution of the IAL classification - it formally recognizes pure neuritic leprosy as a distinct group, which is especially relevant for Nepal where PNL is common.
Q3. In Ridley-Jopling classification, which form of leprosy is described as "immunologically unstable" and prone to reactions?
- A) TT and LL
- B) Borderline (BT, BB, BL)
- C) Indeterminate only
- D) LL only
Answer: B - Borderline (BT, BB, BL). Jopling's core principle: the two polar forms (TT and LL) are immunologically stable. The borderline group is inherently unstable and can shift in either direction, manifesting as Type 1 reactions during upgrading.
Q4. The Mitsuda reaction in lepromin test is READ at:
- A) 24 hours (Fernandez reaction)
- B) 72 hours
- C) 7 days
- D) 28 days
Answer: D - 28 days. The Fernandez (early) reaction is at 24-48 hours. The Mitsuda (late) reaction at 28 days is the clinically relevant reading, reflecting the granuloma-forming capacity of CMI.
Q5. Which statement about the grenz zone is CORRECT according to Jopling's 1966 classification?
- A) The grenz zone is absent in lepromatous leprosy
- B) The grenz zone is present in TT because the infiltrate does not reach the epidermis
- C) In TT, granulomas extend to the epidermis WITHOUT a grenz zone; in BT there is a clear (though narrow) subepidermal zone
- D) The grenz zone is only seen in histoid leprosy
Answer: C. Per Jopling's original description: TT has granulomas that "extend up to the epidermis without a subepidermal zone." The grenz zone (subepidermal clear zone) appears from BT onward and widens toward the lepromatous pole.
Q6. Histoid leprosy is associated with:
- A) Clofazimine monotherapy failure
- B) Rifampicin resistance
- C) Dapsone monotherapy or dapsone resistance
- D) Treatment with thalidomide
Answer: C. Histoid leprosy (Wade, 1963) is classically described after dapsone monotherapy (pre-MDT era) or in patients with dapsone resistance. It can also occur de novo but dapsone resistance must always be considered. The folP1 gene mutation in M. leprae is the molecular mechanism of dapsone resistance.
Q7. In lepromatous leprosy, the principal cytokines that suppress CMI are:
- A) IFN-γ and TNF-α
- B) IL-4, IL-5, IL-10 (Th2 dominant)
- C) IL-12 and IL-17
- D) IL-2 and IL-23
Answer: B. LL represents a classic Th2 response. IL-4 and IL-10 downregulate CMI, suppress macrophage activation (macrophages cannot kill M. leprae), and enhance antibody production (polyclonal hypergammaglobulinemia, false-positive VDRL, RF, ANA). TT is a Th1 response (IFN-γ, IL-2, IL-12).
Q8. Which nerve is palpated at the neck of the fibula in leprosy examination?
- A) Posterior tibial nerve
- B) Sural nerve
- C) Saphenous nerve
- D) Common peroneal (lateral popliteal) nerve
Answer: D - Common peroneal (lateral popliteal) nerve. It wraps around the neck of the fibula (approximately 2-3 cm below the fibular head), which is its most superficial point and the site of leprosy involvement. This is the nerve responsible for foot drop when damaged.
Q9. A 4-grade scale for grading nerve thickness in leprosy is used in which textbook/manual?
- A) Fitzpatrick's only
- B) IAL Practical Manual of Leprosy
- C) Park's only
- D) Red Book
Answer: B - IAL Practical Manual of Leprosy. The 4-grade scale (0-3) for both nerve thickness and nerve tenderness is described in the Practical Manual of Leprosy (based on IAL guidelines). Grade 0 = normal; Grade 1 = slightly thickened; Grade 2 = moderately thickened; Grade 3 = grossly thickened/visible.
Q10. The "onion skin" (laminated) perineurium on nerve histology is characteristic of:
- A) Tuberculoid leprosy
- B) Lepromatous leprosy
- C) Borderline tuberculoid leprosy
- D) Histoid leprosy
Answer: B - Lepromatous leprosy. In LL, the perineural cells undergo repeated rounds of proliferation and fibrosis in response to chronic bacillary presence, producing the characteristic "onion-skin" or lamellar lamination of the perineurium. This contrasts with TT, where nerves show perineural concentric fibrosis and are destroyed within the granuloma.
Q11. Post-kala-azar dermal leishmaniasis (PKDL) is an important differential for leprosy in Nepal because:
- A) Both are caused by acid-fast bacilli
- B) Both affect the same Province 2 (Terai) of Nepal and produce hypopigmented patches
- C) PKDL also causes nerve thickening
- D) PKDL has positive Mitsuda test
Answer: B. Province 2 (Madhesh Province, Terai) is the highest burden area for BOTH leprosy and kala-azar/PKDL in Nepal. PKDL presents with hypopigmented macules and nodules similar to leprosy. The key distinguishing features: PKDL has NO sensory loss and NO nerve thickening; skin biopsy/smear shows Leishmania amastigotes (Donovan bodies).
Q12. The "saucer right-side up" appearance is a classic description for which type of leprosy lesion?
- A) Lepromatous plaque
- B) Tuberculoid plaque
- C) ENL nodule
- D) Histoid nodule
Answer: B - Tuberculoid (TT) plaque. The TT lesion has a raised, defined peripheral border that slopes down to a flattened, atrophic, hypopigmented center - like a saucer placed right-side up. The BB lesion is described as "saucer upside-down" (outer border less defined, inner edge punched-out/cleared). These classical descriptions are from Jopling.
Q13. The IAL classification formally uses "Polyneuritis (P)" to represent:
- A) Patients with polyneuropathy from dapsone
- B) Patients with ENL causing multiple nerve involvement
- C) Pure neuritic leprosy - peripheral nerve involvement without skin lesions
- D) Patients with leprosy and co-existing diabetic neuropathy
Answer: C - Pure neuritic leprosy (PNL). This is a form in which the peripheral nerve trunks are involved without any skin lesions. Per IAL, it may be TT or BT depending on the number of nerves involved. It is classified under group P in the IAL system. Diagnosis requires nerve biopsy or PCR. Nepal has the highest burden of PNL globally, alongside Brazil and India.
QUICK REFERENCE: JOPLING'S KEY MNEMONICS & PEARLS
| Pearl | Source |
|---|
| "Temperature is lost first, before touch and pain" | Jopling - dissociation of sensation pathognomonic for leprosy |
| "The borderline group is unstable; TT and LL are stable" | Ridley-Jopling 1966 |
| "Saucer right-side up = TT; upside-down = BB" | Jopling clinical description |
| "Granuloma extends to epidermis in TT (no grenz zone); grenz zone present from BT onward" | Ridley-Jopling histology 1966 |
| "Never skip nerve examination" | IAL Practical Manual |
| "MDT must never be stopped during reactions" | IAL + WHO |
| "Histoid leprosy = dapsone resistance until proven otherwise" | IAL Textbook |
| "GAN is the most visibly enlarged nerve" | IAL/Andrews' |
| "BI falls 1 unit/year on MDT; MI falls first (weeks)" | Ridley's scale |
| "PKDL in Province 2 Nepal = key differential for leprosy" | Nepal NLS 2021-25 |
References:
- Ridley DS, Jopling WH. Classification of leprosy according to immunity: a five-group system. Int J Lepr. 1966;34(3):255-273.
- IAL - All India Leprosy Workers Conference. New Indian Classification. Lepr India. 1982;54:22-32.
- IAL Practical Manual of Leprosy (Kar HK, Kumar B eds.). Chapter on nerve examination and grading.
- International Textbook of Leprosy - Clinical Diagnosis chapter (internationaltextbookofleprosy.org)
- Andrews' Diseases of the Skin, 13th ed. (Clinical Dermatology), Chapter 17.
- Dermatology 2-Volume Set, 5e (Bourke et al.), Chapter 75.
- Fitzpatrick's Dermatology, 9th ed., Chapter 159.
- Park's Textbook of Preventive & Social Medicine, 26th ed., Chapter on Leprosy.
- Nepal National Leprosy Strategy 2021-2025.
- WHO Leprosy Guidelines & Fact Sheet (who.int).
- An update of the diagnosis, treatment, and prevention of leprosy (PMC11346855)
- High-Resolution Ultrasonography for Detecting Peripheral Neuropathy in Leprosy: A Systematic Review and Meta-Analysis (PMID 41773898)