Ethical cosiderations of MTP
Reading File
Finding Sources
Finding Sources
Searching PubMed
"massive transfusion protocol" AND ethics
Searching the Web
ethical considerations massive transfusion protocol MTP clinical ethics
It's medical termination of pregnancy
Reading File
Finding Sources
Finding Sources
Searching PubMed
"medical termination of pregnancy" AND ethics
Searching the Web
ethical considerations medical termination of pregnancy MTP abortion ethics principles
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive material. Let me compile a thorough, well-structured answer on the ethical considerations of MTP.
Ethical Considerations of Medical Termination of Pregnancy (MTP)
The ethical landscape of MTP is multi-dimensional, involving the rights and interests of the pregnant woman, the moral status of the fetus, the duties of healthcare providers, and the responsibilities of the state. These are examined below under distinct ethical dimensions.
1. The Four Pillars of Bioethics Applied to MTP
| Principle | Application to MTP |
|---|---|
| Autonomy | A woman has the right to make decisions about her own body. Consent of the husband is NOT required; consent of the woman herself is central. |
| Beneficence | MTP aims to prevent harm from unwanted pregnancy, unsafe abortion, and maternal morbidity/mortality. |
| Non-maleficence | Preventing harm from unsafe, illegal abortions; avoiding complications from late or botched procedures. |
| Justice | Equitable access to safe MTP services regardless of socioeconomic status, marital status, or geography. |
2. Autonomy and Consent
-
Woman's right to decide: The pregnant woman's consent is the cornerstone of MTP ethics. The husband's consent is explicitly not required under the MTP Act.
-
Minor/guardian consent: Written consent of a guardian is required when the woman is under 18 years or is a mentally ill person - this raises the ethical issue of balancing child protection with respecting the minor's own developing autonomy.
-
Freedom from coercion: Abortion cannot be performed at the husband's or anyone else's request if the woman herself is not willing. This is a codified protection against reproductive coercion.
-
Informed consent: The woman must be fully informed of the procedure, risks, and alternatives before giving consent.
-
The Essentials of Forensic Medicine and Toxicology 36th ed., p. 393
-
P C Dikshit Textbook of Forensic Medicine and Toxicology, p. 370
3. Moral Status of the Fetus
This is the central philosophical controversy in MTP ethics:
- Gradualist view: Moral status of the fetus increases with gestational age. This is reflected in Indian law - up to 20 weeks requires one RMP opinion, 20-24 weeks requires two RMPs, and beyond 24 weeks requires a Medical Board approval. This graduated framework implies recognition that the fetus acquires increasing moral weight over time.
- Viability threshold: The concept of fetal viability (~20-24 weeks) is ethically significant because beyond it, the fetus may be capable of independent survival, making termination more morally complex.
- No absolute fetal rights vs. maternal rights: Indian law does not recognize the fetus as a legal person, but does protect against termination purely on grounds of fetal sex (PCPNDT Act operates alongside MTP Act for this purpose).
4. Indications and Their Ethical Justifications
The law recognizes four broad ethical grounds for MTP:
| Ground | Ethical Basis |
|---|---|
| Therapeutic - risk to life/health of woman | Non-maleficence; maternal life takes priority |
| Eugenic - substantial risk of serious fetal abnormality | Prevention of suffering; quality of life consideration |
| Social/Contraceptive failure - anguish from unintended pregnancy | Respect for autonomy and reproductive self-determination |
| Humanitarian - pregnancy from rape or incest | Relief from harm inflicted without consent; trauma prevention |
- The eugenic ground raises its own ethical concern - "who decides" what constitutes a "serious abnormality" sufficient to justify termination, and whether this risks discriminatory attitudes toward people with disabilities.
- The humanitarian ground (rape/incest) is notable in that the woman's allegation alone is sufficient - she need not produce a police complaint. This ethically privileges her subjective experience of trauma over procedural proof.
5. Confidentiality
-
The MTP admission register is a secret document - information cannot be disclosed to any person.
-
Maintaining confidentiality protects the woman from social stigma, violence, and discrimination.
-
It also serves the ethical principle of respecting the woman's privacy as a foundational right.
-
The Essentials of Forensic Medicine and Toxicology 36th ed., p. 393
6. Conscientious Objection by Providers
- Physicians may, on the basis of personal moral/religious convictions, decline to perform MTP - this is recognized by the Principles of European Medical Ethics (Article 17) and widely accepted in medical ethics.
- However, conscientious objection has a critical limit: in emergencies where the woman's life is at risk, no physician can refuse on grounds of conscience. The duty to save life overrides personal objection.
- A provider who conscientiously objects must refer the patient to a willing provider. Failure to do so - causing harm to the patient - constitutes ethical and legal breach.
7. Gestational Limits and Late Termination
- The ethical tension around late MTP (>20 weeks) is significant. Women who seek late terminations often do so because of newly diagnosed fetal anomalies, delayed recognition of pregnancy, barriers to access, or circumstances like rape.
- The Supreme Court of India has permitted termination of near-30-week pregnancies in exceptional cases (e.g., 14-year-old rape victims), acknowledging that rigid gestational cutoffs can cause grave injustice in vulnerable cases.
- The Medical Board model for >24-week cases attempts to balance fetal interests with maternal welfare through multi-disciplinary clinical and ethical oversight.
8. Sex-Selective Abortion: A Major Ethical Concern
- The PCPNDT Act exists precisely because of the misuse of reproductive healthcare for sex-selective termination (female feticide). This is ethically condemned as it:
- Violates the right to life based solely on sex
- Perpetuates gender discrimination
- Distorts population sex ratios with long-term social harm
- MTP Act (permissive for other grounds) must be clearly distinguished from sex-selective abortion, which is illegal under PCPNDT Act regardless of gestational age.
| Feature | MTP Act | PCPNDT Act |
|---|---|---|
| Objective | Legal framework for termination under specified conditions | Prohibit sex-selective termination; regulate prenatal diagnostic techniques |
| Ethical focus | Maternal welfare and autonomy | Fetal rights (sex-based); gender justice |
- The Essentials of Forensic Medicine and Toxicology 36th ed., p. 394
9. Access and Justice
- Unsafe abortions disproportionately affect women who cannot access legal MTP services due to poverty, geographic remoteness, lack of trained providers, or social stigma.
- The MTP Act aims to reduce maternal mortality from unsafe abortions - this is a public health ethics mandate, not just a clinical one.
- The 2021 Amendment extended access to unmarried women (contraceptive failure ground now applies to all women, not just married women) - an ethically significant step toward equitable reproductive rights.
- Training gaps (shortage of qualified RMPs in rural areas) create a justice issue: the legal right to MTP is meaningless if services are inaccessible.
10. Good Faith Protection and Provider Accountability
- Section 8 of the MTP Act protects RMPs from legal action for any damage caused "in good faith" while following the Act. This is ethically important because it enables providers to exercise clinical judgment without fear of criminal liability.
- However, this protection does not extend to negligent or coercive practice - ethical standards of care must still be maintained.
Summary Table of Key Ethical Issues
| Ethical Issue | Core Tension |
|---|---|
| Woman's autonomy | vs. perceived fetal interests |
| Fetal moral status | vs. maternal rights |
| Gestational age limits | vs. individual circumstances |
| Conscientious objection | vs. duty of care |
| Confidentiality | vs. transparency |
| Access to services | vs. regulatory restrictions |
| Sex-selective abortion | Gender justice vs. reproductive autonomy |
| Late-term MTP | Fetal viability vs. maternal suffering |
Sources:
- The Essentials of Forensic Medicine and Toxicology, 36th ed. (2026), Chapter on MTP Act (Annexure 36.2)
- P C Dikshit Textbook of Forensic Medicine and Toxicology, Chapter on MTP
- Park's Textbook of Preventive and Social Medicine, MTP as Reproductive Health Measure
- National Abortion Federation - Ethical Principles for Abortion Care
- Stanford Encyclopedia of Philosophy - Ethics of Abortion
- AMA Code of Medical Ethics - Opinion 4.2.7 Abortion
Kidney anatomy and functions
Reading File
Finding Sources
Finding Sources
Searching the Web
kidney anatomy structure functions nephron physiology overview
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive material with excellent diagrams. Let me compile the full, detailed answer on kidney anatomy and functions.
Kidney Anatomy and Functions
Gross Anatomy
The kidneys are paired, bean-shaped, retroperitoneal organs located on either side of the vertebral column, extending from the T12 to L3 vertebrae. The right kidney is slightly lower than the left (due to the liver above it).
Size and weight:
- Males: 125-170 g, ~12 cm long, 5-7.5 cm wide, 2.5-3 cm thick
- Females: 115-155 g, slightly smaller
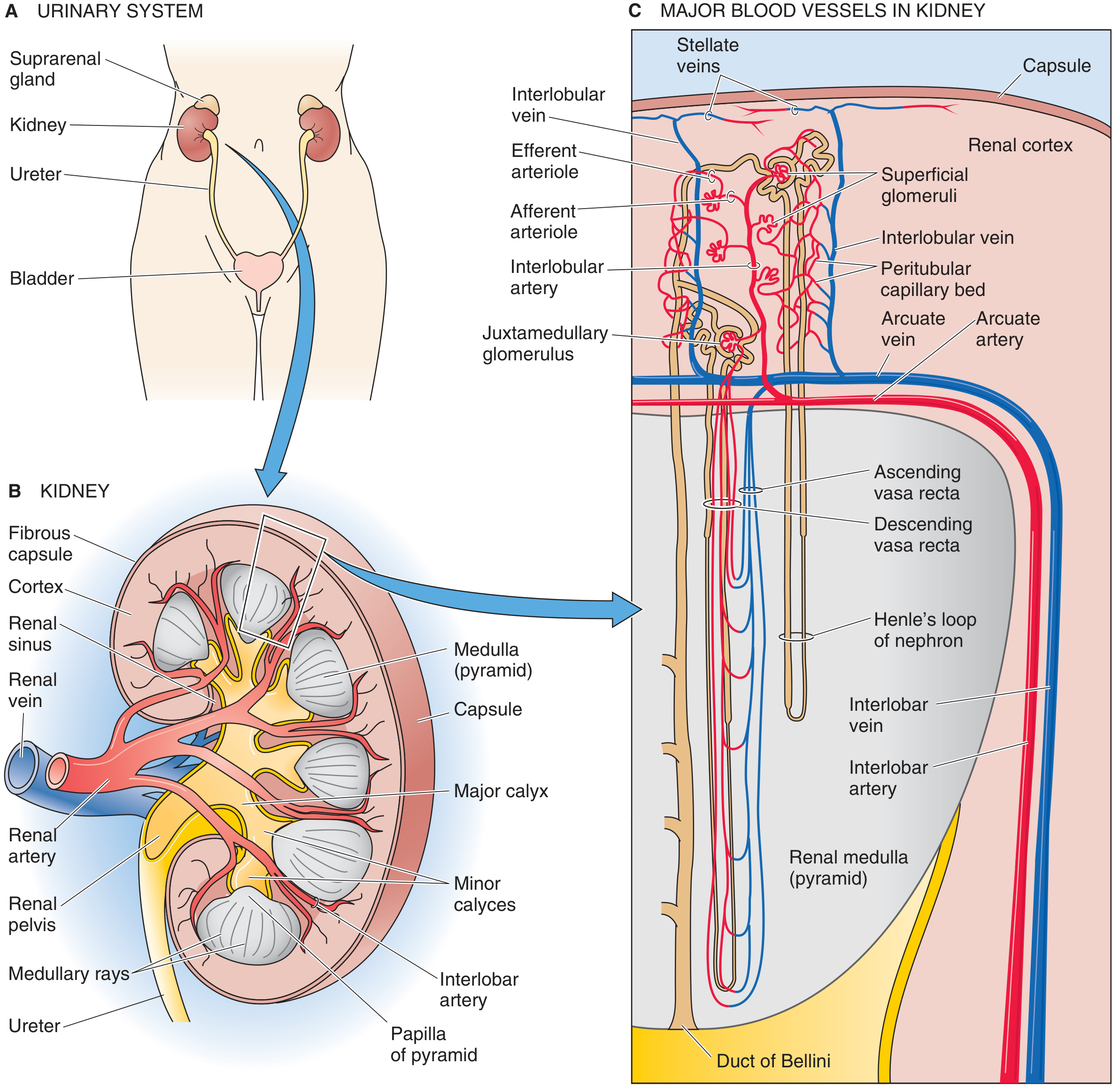
Key external features:
- Fibrous capsule - tough, nondistensible outer covering
- Hilum - medial concave indentation; entry/exit point for renal artery, renal vein, ureter, lymphatics, and nerve plexus
- Renal sinus - fat-filled space inside the hilum containing the renal pelvis, calyces, vessels, and nerves
Internal structure (on cross-section):
| Region | Features |
|---|---|
| Cortex (outer, granular) | Contains glomeruli, proximal and distal convoluted tubules; medullary rays extend downward |
| Medulla (inner, striated) | 8-18 conical renal pyramids; contains loops of Henle and collecting ducts |
| Columns of Bertin | Extensions of cortex between pyramids |
| Papilla | Apex of each pyramid; urine drips through area cribrosa into minor calyces |
| Minor calyces | Cup-shaped structures surrounding each papilla |
| Major calyces | 2-3 per kidney; formed by union of minor calyces |
| Renal pelvis | Funnel-shaped expansion that drains into the ureter |
Blood Supply
The kidneys receive ~20% of cardiac output despite being <0.5% of body weight - essential for high-volume filtration.
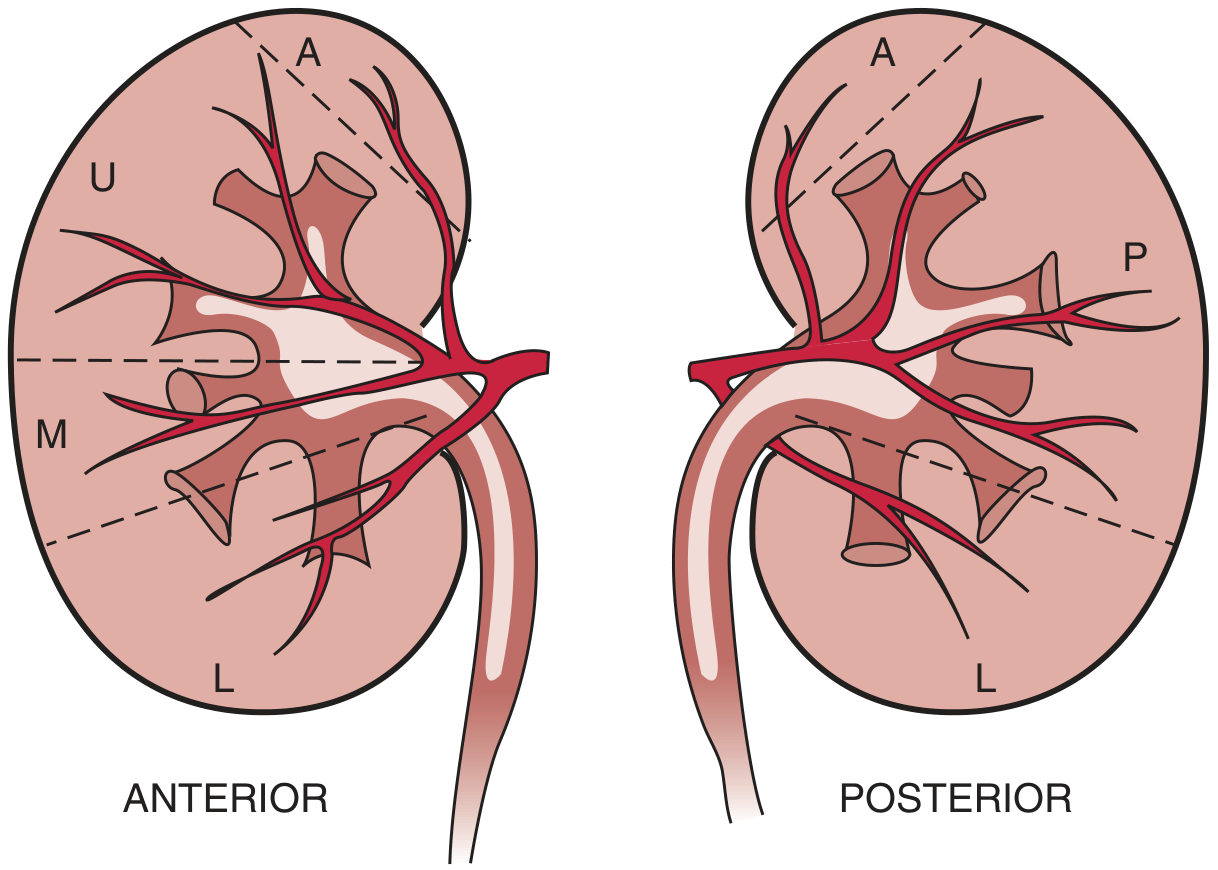
Arterial pathway:
Renal artery → Anterior/Posterior divisions → Segmental (lobar) arteries → Interlobar arteries → Arcuate arteries (at corticomedullary junction) → Interlobular arteries → Afferent arterioles → Glomerular capillaries → Efferent arterioles → Peritubular capillaries / Vasa recta
- No collateral circulation exists between segmental arteries - occlusion causes infarction
- Efferent arterioles of juxtamedullary nephrons form hairpin-shaped vasa recta supplying the medulla
- ~90% of blood perfuses the cortex; only ~10% reaches the medulla
Venous drainage: Peritubular capillaries/vasa recta → Interlobular veins → Arcuate veins → Interlobar veins → Renal vein → Inferior vena cava
The Nephron - Structural and Functional Unit
Each kidney contains 800,000 to 1,200,000 nephrons (range: 200,000 to 2.5 million). Nephrons cannot regenerate after birth; functioning nephrons decline ~10% per decade after age 40.
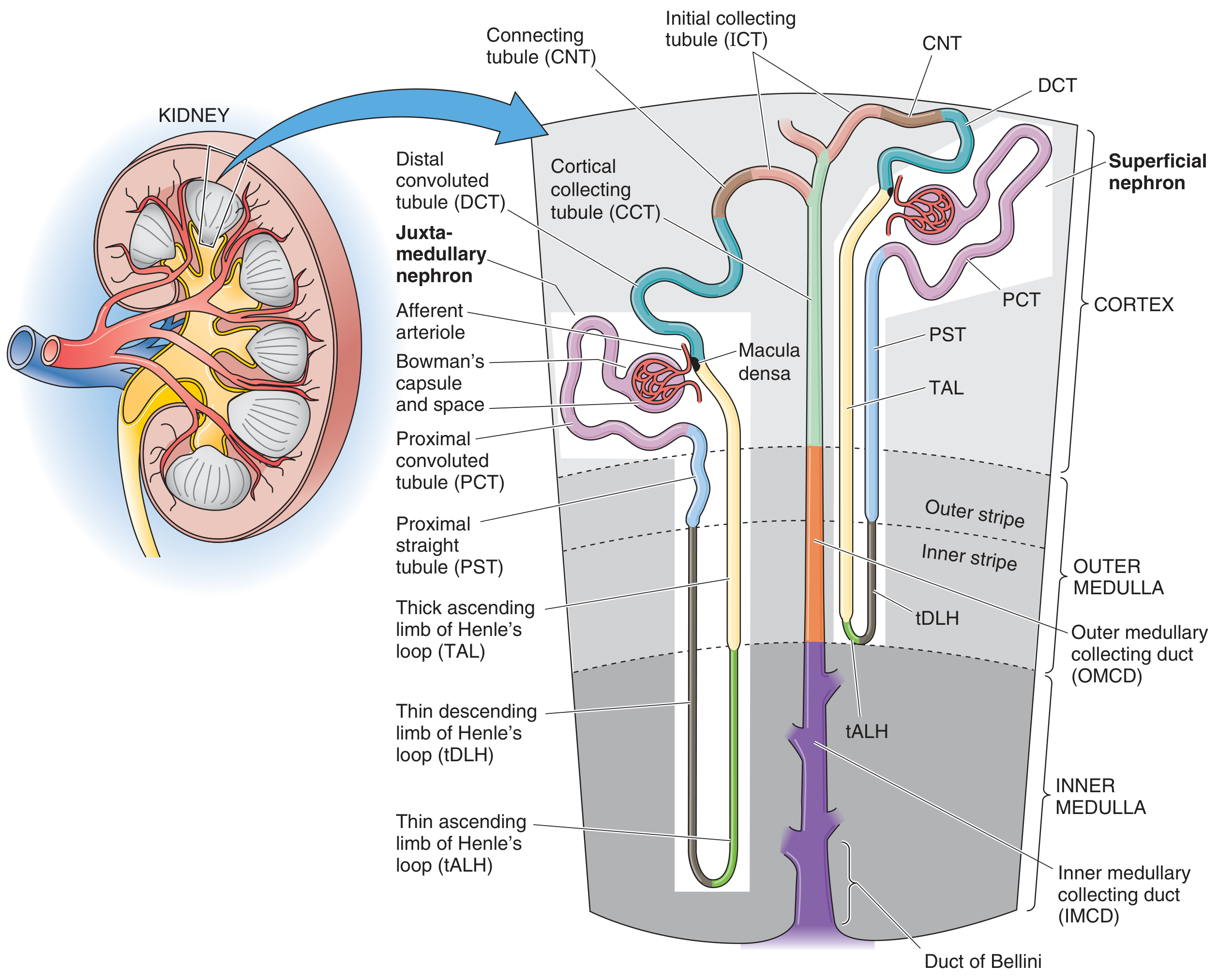
Types of Nephrons
| Type | Location | Loop of Henle | Special Role |
|---|---|---|---|
| Cortical (superficial) | Outer cortex (~85%) | Short loop; stays in outer medulla | General filtration |
| Juxtamedullary | Near corticomedullary junction (~15%) | Long loop reaching inner medulla/papilla | Urine concentration |
Components of the Nephron
1. Renal Corpuscle (Malpighian Corpuscle)
Located in the cortex; consists of:
- Glomerulus - tuft of fenestrated capillaries
- Bowman's capsule - double-walled epithelial cup surrounding the glomerulus
- Parietal layer - simple squamous epithelium
- Visceral layer - specialized podocytes with foot processes (pedicels)
- Bowman's space - between the two layers; collects the ultrafiltrate
Glomerular filtration barrier (4 layers):
- Glycocalyx (negatively charged; repels anionic proteins)
- Fenestrated endothelium (70-nm pores; excludes cells)
- Glomerular basement membrane - lamina rara interna + lamina densa + lamina rara externa (restricts molecules >1 kDa; rich in heparan sulfate proteoglycans)
- Podocyte foot processes with filtration slits (slit diaphragm; final barrier)
2. Proximal Convoluted Tubule (PCT)
- Located in cortex; highly convoluted
- Lined by cells with abundant brush border (microvilli) - greatly increases surface area
- Reabsorbs ~65-70% of filtered Na+, water, glucose, amino acids, bicarbonate, phosphate
3. Loop of Henle
- Descends into medulla and returns to cortex
- Three segments:
- Thin descending limb - freely permeable to water; impermeable to solutes
- Thin ascending limb - impermeable to water; permeable to NaCl
- Thick ascending limb (TAL) - actively pumps NaCl out (NKCC2 cotransporter); impermeable to water; creates medullary hyperosmolarity
- Countercurrent multiplication in the loop establishes the osmotic gradient needed to concentrate urine
4. Distal Convoluted Tubule (DCT)
- Returns to cortex near its own glomerulus
- Contains macula densa cells (part of the juxtaglomerular apparatus)
- Reabsorbs NaCl under the influence of aldosterone; impermeable to water unless ADH present
- Fine-tuning of Ca²+ and Mg²+ reabsorption
5. Collecting Duct System
- Not technically part of the nephron (derived from ureteric bud, not metanephric blastema)
- Consists of: initial collecting tubule → cortical collecting duct (CCD) → outer medullary collecting duct (OMCD) → inner medullary collecting duct (IMCD) → Duct of Bellini
- Final regulation of water (via ADH/vasopressin), acid-base balance, and K+ excretion
- Two cell types: principal cells (Na+/K+ exchange, ADH-sensitive water reabsorption) and intercalated cells (H+ or HCO₃⁻ secretion)
Juxtaglomerular Apparatus (JGA)
A specialized structure at the vascular pole of each glomerulus, consisting of:
| Component | Location | Function |
|---|---|---|
| Macula densa | DCT wall adjacent to arterioles | Senses luminal NaCl concentration; signals to JG cells |
| Juxtaglomerular (JG) cells | Afferent arteriole wall | Produce and secrete renin |
| Mesangial cells (extraglomerular) | Between arterioles and macula densa | Signal transduction; may modulate GFR |
The JGA is central to the renin-angiotensin-aldosterone system (RAAS) and tubuloglomerular feedback.
Functions of the Kidney
1. Urine Formation (Excretion)
Three sequential processes in each nephron:
| Process | Location | What happens |
|---|---|---|
| Filtration | Glomerulus | ~180 L/day of plasma ultrafiltrate formed; GFR ~125 mL/min |
| Reabsorption | Tubules | ~178.5 L/day returned to blood; conserves glucose, amino acids, water, electrolytes |
| Secretion | Tubules | Active transport of waste products (H+, K+, creatinine, drugs, uric acid) into tubule lumen |
Final urine output: ~1-2 L/day
2. Regulation of Fluid and Electrolyte Balance
- Controls extracellular fluid volume and osmolarity
- Regulates Na+, K+, Ca²+, Mg²+, phosphate concentrations
- Water balance regulated by ADH (increases collecting duct water permeability)
- Na+ balance regulated by aldosterone (increases PCT/collecting duct Na+ reabsorption)
3. Acid-Base Regulation
- Excretes H+ ions via NH₄+ and titratable acid
- Reabsorbs and regenerates HCO₃⁻
- Maintains blood pH in the range 7.35-7.45
- The kidneys provide slower but more powerful pH correction than respiratory buffers
4. Endocrine Functions
| Hormone | Stimulus | Effect |
|---|---|---|
| Erythropoietin (EPO) | Hypoxia | Stimulates RBC production in bone marrow |
| Renin | Low BP, low Na+, sympathetic activation | Activates RAAS → angiotensin II → aldosterone → Na+ retention |
| 1,25-dihydroxyvitamin D₃ (Calcitriol) | PTH, low Ca²+/phosphate | Activates 1α-hydroxylase; increases intestinal Ca²+ absorption |
| Prostaglandins (PGE₂, PGI₂) | Local | Modulate renal blood flow; natriuresis |
5. Gluconeogenesis
- The kidney (mainly cortex) contributes ~20% of total gluconeogenesis, especially during fasting or prolonged exercise
- Uses glutamine, lactate, and glycerol as substrates
6. Degradation of Hormones
- Kidneys degrade and excrete peptide hormones including insulin, glucagon, and PTH
- This is why insulin requirements fall in diabetic patients with renal failure
Summary: Nephron Segment Functions at a Glance
| Segment | Major Function | Key Transporters/Mediators |
|---|---|---|
| Glomerulus | Filtration (~180 L/day) | Starling forces, filtration barrier |
| PCT | Bulk reabsorption (65-70% Na+, H₂O, glucose, HCO₃⁻, amino acids) | Na+/K+-ATPase, SGLT2, NHE3 |
| Thin descending loop | Water reabsorption | Aquaporin-1 |
| Thick ascending loop | NaCl reabsorption (no water); builds medullary gradient | NKCC2 (site of furosemide action) |
| DCT | NaCl reabsorption; Ca²+ regulation | NCC (site of thiazide action); TRPV5 |
| Collecting duct | Final H₂O, Na+, K+, H+/HCO₃⁻ regulation | Aquaporin-2 (ADH-regulated); ENaC; H+/K+-ATPase |
Sources:
- Brenner and Rector's The Kidney, 2-Volume Set - Chapter: Anatomy of the Kidney
- Medical Physiology (Boron & Boulpaep) - Chapter 33: Functional Anatomy of the Kidney
What are Universal precautions for hiv
Finding Sources
Finding Sources
Searching the Web
universal precautions HIV infection control CDC bloodborne pathogens
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks and CDC guidelines. Let me compile the full answer.
Universal Precautions for HIV
Definition and Background
Universal precautions are a set of infection control practices introduced by the CDC in 1985 (updated in 1987 and 1988) in response to the HIV epidemic. The core principle is:
"Any patient may be infected with bloodborne infectious agents, and it may be difficult, if not impossible, to differentiate infected patients from their uninfected counterparts. Therefore, blood and body fluids of ALL patients should be considered potentially infectious."
Universal precautions were designed to prevent transmission of HIV, HBV (Hepatitis B), HCV (Hepatitis C), and other bloodborne pathogens - primarily to protect healthcare workers (HCWs), but also to protect patients.
Body Fluids Covered by Universal Precautions
Universal precautions APPLY to:
- Blood (most important source of HIV/HBV in occupational settings)
- Semen and vaginal secretions
- Cerebrospinal fluid (CSF)
- Synovial fluid
- Pleural, peritoneal, pericardial, and amniotic fluid
- Any body fluid visibly contaminated with blood
- Wound exudates/unfixed tissue/organ specimens
Universal precautions do NOT apply to (unless visibly blood-contaminated):
- Urine, feces, sweat
- Tears, nasal secretions
- Vomit, sputum, saliva (exception: dental settings where saliva is often blood-tinged)
The Core Components of Universal Precautions
1. Hand Hygiene (Most Important)
- Wash hands with soap and water before and after every patient contact
- Use alcohol-based hand rub if hands are not visibly soiled
- Gloves are NOT a substitute for handwashing - wash hands after glove removal
- Required immediately after contact with blood/body fluids, mucous membranes, or non-intact skin
2. Personal Protective Equipment (PPE)
| PPE Item | When to Use |
|---|---|
| Gloves | Any procedure involving contact with blood, body fluids, mucous membranes, or non-intact skin; handling sharps or specimens. Double gloving recommended in surgical procedures (reduces volume of blood from needlestick by 50%) |
| Gowns/aprons | When splashing or splattering of blood/body fluids is anticipated |
| Masks | Risk of blood/fluid droplet splash to mouth/nose; all surgical procedures |
| Protective eyewear/goggles | Risk of splash to eyes; face shields offer maximum protection |
| Shoe covers/boots | Operating room and trauma settings |
| Head covers | Surgical procedures |
3. Safe Handling of Sharp Instruments ("Sharps")
This is the single greatest risk for HIV transmission to HCWs.
Key rules:
- Never recap used needles - recapping is the most common cause of needlestick injuries
- Never bend, break, or manipulate used needles by hand
- Never pass sharps hand-to-hand; use an intermediate tray and announce transfer
- Dispose of used sharps immediately in puncture-resistant, impervious containers placed near the point of use
- Containers must be checked frequently and not overfilled
- Use self-sheathing/safety needles where available (engineering control)
- Reinforced gloves when sharp instruments or bone fragments are likely
4. Handling of Blood and Body Fluid Specimens
- All specimens must be treated as potentially infectious
- Specimens must be transported in leak-proof, labeled containers
- Gloves required for handling all biological specimens
- Clean up blood spills immediately with appropriate disinfectant (10% bleach solution or hospital-grade disinfectant)
5. Decontamination and Sterilization of Equipment
- Reusable instruments must be cleaned, disinfected, and sterilized before reuse
- Single-use items (needles, syringes) must never be reused
- Contaminated surfaces should be cleaned with appropriate hospital-grade disinfectants
6. Waste Disposal
- Contaminated waste must be disposed of in labeled biohazard bags
- Sharps disposed of in rigid puncture-resistant sharps containers
- Liquid blood/body fluid waste may be carefully poured down sanitary drains in most healthcare settings
7. Avoid Direct Patient Contact with Open Skin Lesions
- HCWs with denuded skin, open lesions, weeping dermatitis, or active exudative conditions should avoid direct patient care and should not handle contaminated equipment
- Wear appropriate dressings/double gloves if contact is unavoidable
Risk of Seroconversion After Exposure
Understanding these figures reinforces why universal precautions matter:
| Pathogen | Risk per needlestick exposure |
|---|---|
| HIV | ~0.3% percutaneous; ~0.09% mucous membrane |
| Hepatitis C (HCV) | ~1.8% |
| Hepatitis B (HBV) | ~30% (highest risk - reinforces need for HBV vaccination) |
Risk of HIV transmission is increased when:
- Device is visibly contaminated with blood
- Device was placed in a vein or artery
- Deep injury occurred
- Source patient has high viral load
- Source patient dies within 2 months of exposure (indicating advanced disease)
Post-Exposure Management (When Precautions Fail)
When a needlestick or mucous membrane exposure occurs despite precautions:
- Immediately wash/flush the wound or exposed site with soap and water (or saline for mucous membranes)
- Report the incident promptly to occupational health/supervisor
- Evaluate the source patient - test for HIV, HBV, HCV if consent obtained
- Evaluate the HCW - baseline HIV test, HBV/HCV status
- Post-Exposure Prophylaxis (PEP):
- Preferred regimen: Tenofovir disoproxil fumarate/Emtricitabine + Raltegravir or Dolutegravir
- Must be initiated within 72 hours of exposure (sooner = better)
- Continue for 28 days (4 weeks)
- Consult: National Clinicians' Post-Exposure Prophylaxis Hotline (1-888-448-4911)
- Follow-up HIV testing at 6 weeks, 3 months, and 6 months post-exposure
Universal Precautions vs. Standard Precautions
Note: In 1996, the CDC replaced "universal precautions" with the broader concept of Standard Precautions, which extended protection to include all body fluids, secretions, and excretions (regardless of visible blood), non-intact skin, and mucous membranes. Standard Precautions also incorporated elements of body substance isolation (BSI). However, the original term "universal precautions" is still widely used and remains the foundation of bloodborne pathogen protection in clinical practice.
Summary
| Precaution | Purpose |
|---|---|
| Hand hygiene | Remove contamination after every patient contact |
| Gloves | Barrier against blood/fluid contact |
| Gowns, masks, eye protection | Prevent splash/spray to skin and mucous membranes |
| Safe sharps handling | Prevent needlestick injuries (highest HIV risk) |
| Sharps containers | Safe disposal, prevent accidental injury |
| Proper specimen handling | Prevent lab/transport exposures |
| Decontamination/sterilization | Eliminate pathogens from reusable equipment |
| Avoid HCW-patient contact with open skin | Prevent bidirectional transmission |
| PEP after exposure | Reduce risk after accidental exposure |
Sources:
- Goldman-Cecil Medicine, International Edition - HIV Prevention Strategies, p. 3702
- Campbell's Operative Orthopaedics, 15th ed. (2026) - Occupational Exposure, Box 22.2
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th ed. - CDC Infection Control Guidelines
- CDC MMWR 1988: Update - Universal Precautions
- CDC MMWR 1987: Recommendations for Prevention of HIV Transmission in Health-Care Settings
Highly active anti retroviral drugs
Finding Sources
Finding Sources
Searching the Web
HAART highly active antiretroviral therapy drug classes mechanism 2024 guidelines
Finding Sources
Finding Sources
Reading Web Page
https://www.ncbi.nlm.nih.gov/books/NBK554533
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, detailed content from multiple authoritative textbooks plus the HIV lifecycle diagram. Let me compile the complete answer.
Highly Active Antiretroviral Therapy (HAART)
What is HAART?
HAART (Highly Active Antiretroviral Therapy), also called ART or cART (combination ART), is a treatment regimen comprising three or more antiretroviral drugs from at least two different drug classes. Introduced in the mid-1990s, it transformed HIV from a fatal disease into a manageable chronic condition.
Core principle: Combining drugs that target different steps in the HIV lifecycle simultaneously - so that if the virus develops resistance to one drug, the other drugs still suppress it.
The FDA has approved drugs in 7 main classes, targeting distinct stages of viral replication.
HIV Lifecycle and Drug Target Sites
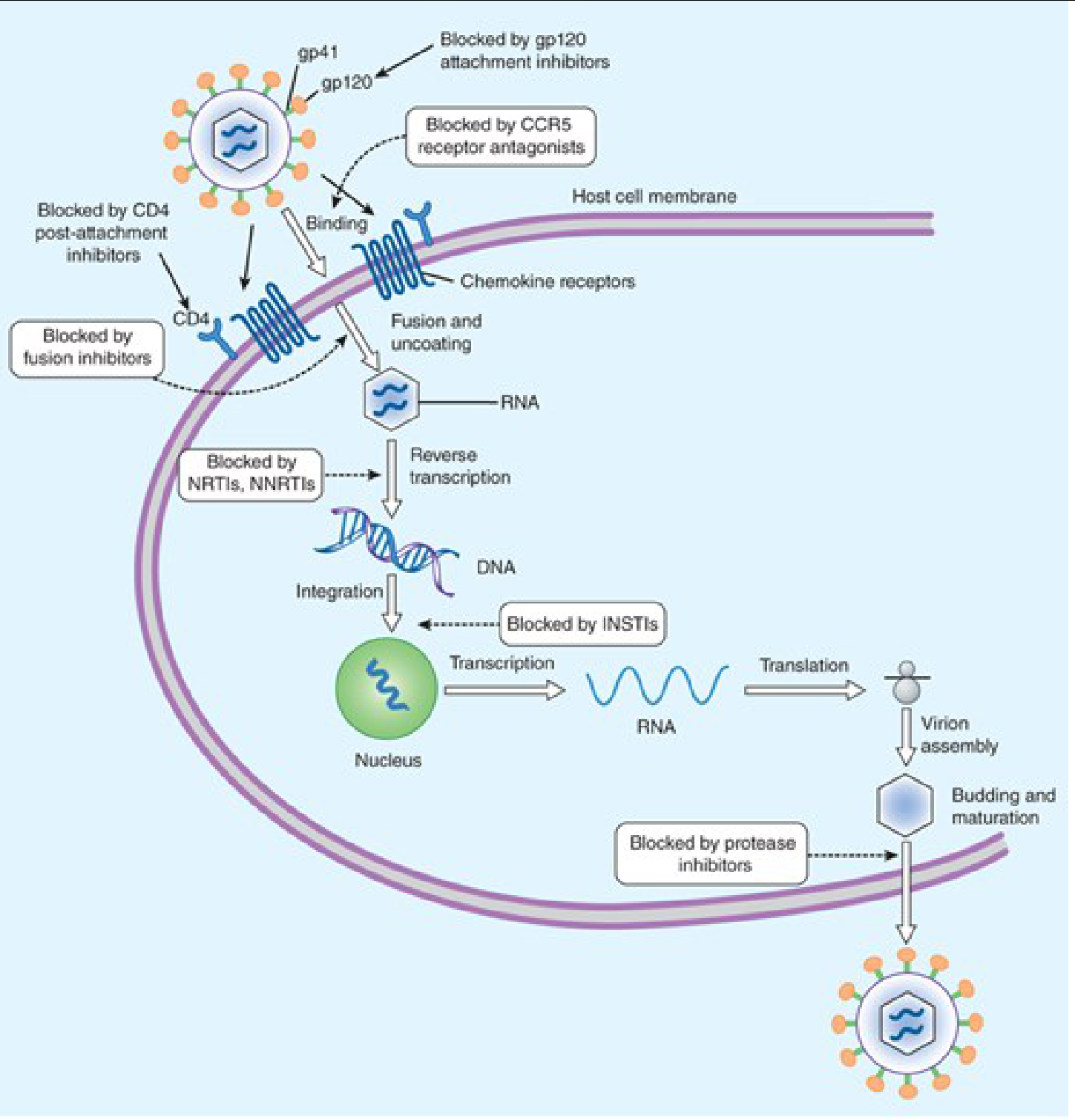
Drug Classes
1. Nucleoside/Nucleotide Reverse Transcriptase Inhibitors (NRTIs)
Mechanism: NRTIs are prodrugs that are phosphorylated intracellularly to their active triphosphate form. They act as chain terminators - they incorporate into the elongating viral DNA strand in place of natural nucleosides and, lacking a 3'-OH group, prevent further elongation. This blocks the reverse transcriptase enzyme from converting viral RNA into DNA.
Key drugs:
| Drug | Abbreviation | Trade Name | Notes |
|---|---|---|---|
| Zidovudine | ZDV / AZT | Retrovir | First antiretroviral (1987); used in PMTCT |
| Lamivudine | 3TC | Epivir | Well tolerated; also active against HBV |
| Emtricitabine | FTC | Emtriva | Similar to 3TC; long intracellular half-life |
| Tenofovir disoproxil fumarate | TDF | Viread | Nephrotoxic; causes bone mineral loss |
| Tenofovir alafenamide | TAF | Vemlidy | Newer prodrug; ~90% less plasma tenofovir; better renal/bone profile |
| Abacavir | ABC | Ziagen | Risk of fatal hypersensitivity - requires HLA-B*5701 testing before use |
Class adverse effects: Mitochondrial toxicity (lactic acidosis, lipoatrophy), hepatic steatosis, peripheral neuropathy (didanosine, stavudine), renal toxicity (TDF), bone density loss
2. Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs)
Mechanism: NNRTIs directly bind to a hydrophobic pocket on the reverse transcriptase enzyme (allosteric site, distinct from the active site). This causes a conformational change that slows/stops reverse transcription. Unlike NRTIs, they do not require intracellular phosphorylation and are not incorporated into DNA.
Key drugs:
| Drug | Abbreviation | Trade Name | Notes |
|---|---|---|---|
| Efavirenz | EFV | Sustiva | Once daily; CNS side effects (vivid dreams, dizziness), teratogenic (Category D) |
| Nevirapine | NVP | Viramune | Used in resource-limited settings; risk of severe hepatotoxicity and rash/SJS |
| Rilpivirine | RPV | Edurant | Preferred in low viral load patients; part of long-acting injectable combo |
| Etravirine | ETR | Intelence | Active against some NNRTI-resistant strains |
| Doravirine | DOR | Pifeltro | Newer; fewer CNS effects; once daily |
Class adverse effects: Rash (including Stevens-Johnson syndrome with nevirapine), hepatotoxicity, CNS effects (efavirenz), lipid changes
Key difference - NRTIs vs NNRTIs: NRTIs insert INTO the growing DNA chain; NNRTIs bind DIRECTLY to the enzyme and inhibit its function without being incorporated.
3. Protease Inhibitors (PIs)
Mechanism: HIV protease cleaves polyproteins (gag and gag-pol) into functional structural and enzymatic proteins during viral maturation. PIs block the active site of HIV protease, preventing the maturation of new virions into infectious particles. Immature, non-infectious viral particles are released.
PIs act late in the viral lifecycle - after integration and transcription have already occurred.
Key drugs:
| Drug | Abbreviation | Trade Name | Boosting |
|---|---|---|---|
| Darunavir | DRV | Prezista | + ritonavir or cobicistat (preferred PI) |
| Atazanavir | ATV | Reyataz | + ritonavir or cobicistat; causes benign indirect hyperbilirubinemia |
| Lopinavir/ritonavir | LPV/r | Kaletra | Fixed-dose co-formulation |
| Ritonavir | RTV | Norvir | Now used as a pharmacokinetic booster only (inhibits CYP3A4/2D6) |
| Saquinavir | SQV | Invirase | First PI approved |
| Tipranavir | TPV | Aptivus | For treatment-experienced patients |
Ritonavir boosting: Ritonavir strongly inhibits CYP3A4, dramatically raising plasma levels of co-administered PIs. This allows lower doses, less frequent dosing, and improved tolerability. Cobicistat is a newer CYP3A4 inhibitor used for the same purpose but with no intrinsic antiviral activity.
Class adverse effects: GI upset (nausea, diarrhea), metabolic syndrome (dyslipidemia, insulin resistance, lipodystrophy), indirect hyperbilirubinemia (atazanavir), nephrolithiasis (indinavir), hepatotoxicity
4. Integrase Strand Transfer Inhibitors (INSTIs)
Mechanism: After reverse transcription, viral DNA must integrate into the host genome via the HIV integrase enzyme. INSTIs block the strand transfer step - they chelate the Mg²+ ions at the active site of integrase, preventing the enzyme from inserting viral DNA ends into host chromosomal DNA.
INSTIs are among the most potent and best-tolerated antiretrovirals and form the backbone of current first-line regimens.
Key drugs:
| Drug | Abbreviation | Notes |
|---|---|---|
| Dolutegravir | DTG | Preferred first-line; high barrier to resistance; avoid in first trimester (neural tube defect risk) |
| Bictegravir | BIC | Only available as fixed-dose combo (BIC/TAF/FTC); high barrier to resistance |
| Raltegravir | RAL | First approved INSTI; twice daily; lower barrier to resistance |
| Elvitegravir | EVG | Requires cobicistat boosting; not recommended for CrCl <70 mL/min |
| Cabotegravir | CAB | Long-acting injectable (monthly IM with rilpivirine); also used for PrEP |
Class adverse effects: Generally well tolerated; insomnia, headache, GI symptoms; weight gain (more than NNRTIs or PIs); neural tube defects with dolutegravir (periconceptional use - caution required)
5. Entry Inhibitors
These block HIV from entering CD4+ T cells. Three sub-classes:
a. Fusion Inhibitors
- Enfuvirtide (T-20) - Binds to gp41 on the viral envelope, preventing the conformational change needed for membrane fusion. Given by subcutaneous injection twice daily. Reserved for treatment-experienced patients with drug-resistant HIV. Local injection site reactions are common.
b. CCR5 Antagonists (Co-receptor antagonists)
- Maraviroc - Binds to the human CCR5 co-receptor, blocking HIV from using it as an entry point. Only effective against CCR5-tropic virus - a co-receptor tropism assay is required before use. Not effective if patient has CXCR4-tropic or dual-tropic virus.
c. Post-attachment Inhibitors (CD4-directed)
- Ibalizumab - A monoclonal antibody binding CD4 (post-attachment; does not prevent CD4-MHC interactions); given IV every 2 weeks. First monoclonal antibody approved for HIV-1 treatment.
d. Attachment Inhibitors (gp120-directed)
- Fostemsavir - Prodrug converted to temsavir; binds to HIV gp120 directly, preventing attachment to CD4. For heavily treatment-experienced patients with multidrug-resistant HIV (approved 2020).
6. Capsid Inhibitors
-
Lenacapavir - Newest class; binds between p24 capsid subunits, disrupting multiple steps in the HIV lifecycle:
- Blocks nuclear transport of the capsid core
- Prevents capsid uncoating (disassembly)
- Interferes with capsid reassembly during viral maturation
Given by subcutaneous injection every 6 months (after oral/SC loading). Licensed for heavily treatment-experienced patients with multidrug-resistant HIV. Also in clinical trials for long-acting PrEP.
7. Pharmacokinetic Boosters (not antivirals per se)
- Ritonavir and Cobicistat - Inhibit CYP3A4 to raise plasma levels of co-administered PIs or INSTIs. Not considered antiretroviral drugs in isolation.
Current Recommended HAART Regimens
Preferred First-Line Regimen (Treatment-Naive Adults)
The current standard (IAS-USA 2024, WHO, DHHS) is:
2 NRTIs + 1 INSTI
| Preferred Regimen | Components | Form |
|---|---|---|
| Bictegravir/TAF/FTC | BIC + TAF + emtricitabine | Single tablet once daily |
| Dolutegravir/TDF/3TC | DTG + TDF + lamivudine | Global preferred (WHO) |
| Dolutegravir + lamivudine | DTG + 3TC | Two-drug option (equivalent to 3-drug in some patients) |
| Cabotegravir + rilpivirine IM | CAB + RPV | Monthly or bi-monthly injections (long-acting) |
Why INSTIs preferred: High potency, excellent tolerability, high barrier to resistance (bictegravir, dolutegravir), once-daily dosing, minimal drug interactions compared to PIs.
Fixed-Dose Combination (FDC) Products
FDCs simplify regimens and improve adherence:
| Brand Name | Components |
|---|---|
| Biktarvy | BIC/TAF/FTC (once daily) |
| Triumeq | DTG/ABC/3TC |
| Atripla | EFV/TDF/FTC |
| Descovy | TAF/FTC |
| Truvada | TDF/FTC (also for PrEP) |
| Cabenuva | Cabotegravir + rilpivirine IM |
| Kaletra | LPV/r |
Monitoring During HAART
| Parameter | Frequency |
|---|---|
| HIV RNA (viral load) | Every 3-6 months; goal: undetectable (<50 copies/mL) |
| CD4 count | Every 3-6 months (until stable) |
| Renal function (GFR, urinalysis) | At baseline, when ART started/changed; at least twice yearly |
| Lipid panel | Periodically (especially on PIs) |
| Liver enzymes | Periodically (especially on NNRTIs) |
| Genotypic resistance testing | Before starting ART (drug-resistant HIV ~17% in USA) |
Virologic failure = confirmed HIV RNA >200 copies/mL in an adherent patient. Triggers resistance testing and regimen change. Adherence of 80-85% is needed for effective viral suppression.
Special Considerations
| Situation | Key Points |
|---|---|
| Pregnancy | Dolutegravir has neural tube defect risk in first trimester; use alternative. TDF+FTC preferred. ART prevents MTCT |
| TB co-infection | Rifampin induces CYP3A4 - avoid PIs/elvitegravir; preferred: dolutegravir (at higher dose) or raltegravir |
| Renal failure | Avoid TDF; prefer TAF (down to CrCl >30); avoid cobicistat (CrCl <70) |
| Hepatitis B co-infection | Use TDF or TAF + emtricitabine (active against both HIV and HBV); stopping these can cause HBV flare |
| Post-Exposure Prophylaxis (PEP) | 2 NRTIs + 1 INSTI; start within 72 hours; continue 28 days |
| Pre-Exposure Prophylaxis (PrEP) | TDF/FTC (Truvada) or TAF/FTC (Descovy); or long-acting cabotegravir IM |
Summary: Drug Classes at a Glance
| Class | Abbreviation | Viral Target | Stage Blocked |
|---|---|---|---|
| Nucleoside/Nucleotide RTIs | NRTI | Reverse transcriptase (chain termination) | Reverse transcription |
| Non-nucleoside RTIs | NNRTI | Reverse transcriptase (allosteric binding) | Reverse transcription |
| Protease Inhibitors | PI | HIV protease enzyme | Virion maturation |
| Integrase Strand Transfer Inhibitors | INSTI | HIV integrase (Mg²+ chelation) | Integration |
| Fusion Inhibitors | FI | gp41 (viral envelope) | Membrane fusion |
| CCR5 Antagonists | Human CCR5 co-receptor | Viral entry | |
| Capsid Inhibitors | p24 capsid | Multiple steps |
Sources:
- Harrison's Principles of Internal Medicine, 22nd ed. (2025) - Chapter 208: HIV Disease
- Katzung's Basic and Clinical Pharmacology, 16th ed. - Chapter 49: Antiretroviral Agents
- Goldman-Cecil Medicine, International Edition - Table 357-1/357-3: Antiviral Drugs
- IAS-USA Panel. Antiretroviral Drugs for Treatment and Prevention of HIV in Adults: 2024 Recommendations. JAMA 2024
- StatPearls - HAART (NIH)
Widal test
Finding Sources
Finding Sources
Searching the Web
Widal test typhoid fever principle interpretation limitations
Reading File
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the full, detailed answer on the Widal test.
Widal Test (Felix-Widal Test)
Introduction
The Widal test (also called the Felix-Widal test) is a serological agglutination test used as an aid in diagnosing typhoid fever (enteric fever) caused by Salmonella typhi and paratyphoid fever caused by S. paratyphi A, B, and C.
- Introduced by Georges Ferdinand Widal in 1896
- One of the oldest serological tests still in use
- Widely used in resource-limited and endemic settings where blood culture is unavailable
- Detects agglutinating antibodies (agglutinins) against bacterial antigens in patient serum
Antigens Tested
The Widal test uses four antigen suspensions to detect antibodies:
| Antigen | Organism | Antigen Type |
|---|---|---|
| S. Typhi O (9, 12) | S. typhi | Somatic (cell wall/lipopolysaccharide) |
| S. Typhi H (d) | S. typhi | Flagellar |
| S. Paratyphi A O (1, 2, 12) | S. paratyphi A | Somatic |
| S. Paratyphi A H (a) | S. paratyphi A | Flagellar |
| S. Paratyphi B O (1, 4, 5, 12) | S. paratyphi B | Somatic |
| S. Paratyphi B H (b, phase 1) | S. paratyphi B | Flagellar |
Note: Paratyphi O antigens are often not included separately because they share factor 12 with typhoid O antigen and would cross-react.
The "O" and "H" Antigens
| Antigen | Nature | Antibody Appearance | Significance |
|---|---|---|---|
| O antigen | Somatic (LPS, heat-stable) | Day 6-8 after onset | Indicates active/current infection; more specific |
| H antigen | Flagellar (protein, heat-labile) | Day 10-12 after onset | Can persist long after infection; less specific for current disease |
| Vi antigen | Capsular polysaccharide | Variable | High titers suggest chronic carrier state |
Principle
The test is based on the agglutination reaction:
If the patient's serum contains homologous antibodies (agglutinins), they react with the corresponding antigens in the reagent to produce visible clumping (agglutination).
- The degree of agglutination is used to determine the antibody titer
- Patient serum is serially diluted and mixed with each antigen suspension
- The highest dilution at which visible agglutination occurs = the titer
Methods of Performing the Widal Test
1. Slide (Rapid) Method
- Quick, qualitative/semi-quantitative
- A drop of patient serum + drop of antigen suspension on a glass slide
- Mix and rock for 1 minute; observe for clumping
- Gives a presumptive result only; does not give precise titers
- Useful for screening
2. Tube (Widal's Tube Agglutination) Method - Standard
- Quantitative - provides actual antibody titers
- Serial two-fold dilutions of patient serum (1:20, 1:40, 1:80, 1:160, 1:320, 1:640...)
- Each dilution mixed with a standard suspension of each antigen
- Incubated at 37°C for 18-24 hours
- Read the highest dilution showing visible agglutination = the titer
- More accurate and reliable than the slide method
Timing of the Test
| Time from onset | Antibody status |
|---|---|
| Before day 6 | O antibodies absent; test may be negative |
| Day 6-8 | O antibodies begin to appear |
| Day 10-12 | H antibodies appear; O antibodies rising |
| End of 2nd week | Peak agglutinin titers; best time for single serum testing |
| Convalescence (2-3 weeks later) | Paired serum shows 4-fold rise - most significant |
- Ideal approach: Two samples - one acute (at first contact) and one convalescent (7-10 days later)
- A 4-fold rise in titer between acute and convalescent samples is the strongest evidence of active typhoid infection
Interpretation of Results
Standard Diagnostic Titers
| Antibody | Titer considered positive (single sample) |
|---|---|
| O antigen | ≥ 1:160 (or ≥ 1:320 in some references) |
| H antigen | ≥ 1:640 |
Critical caveat: These thresholds are NOT universal. Baseline titers in healthy individuals vary significantly by region due to:
- Previous subclinical infections
- Prior vaccination
- Endemicity of the area
The Widal test result must always be interpreted against locally established baseline titers for that population.
Patterns and Their Meaning
| Pattern | Interpretation |
|---|---|
| O antibodies raised, H normal | Early acute infection (O appears first) |
| Both O and H raised | Active typhoid - current or recent infection |
| H antibodies raised, O normal | Previous infection or prior vaccination (H persists longer) |
| Only Vi antibody raised (high titer) | Suggests chronic carrier state |
| No rise in titers (on paired samples) | Argues against typhoid (but doesn't exclude it) |
Causes of False Positive Results
- Previous typhoid vaccination (H antibody may persist for years)
- Previous subclinical infection (very common in endemic areas)
- Cross-reactivity with other Salmonella serotypes (share O and H antigens)
- Cross-reactions with other Enterobacteriaceae
- Malaria (Plasmodium falciparum - raises O titers)
- Rickettsial infections (typhus)
- Chronic active hepatitis / cirrhosis - dysgammaglobulinaemia
- Bacteraemia caused by other organisms
- Chronic inflammatory conditions (rheumatoid arthritis, etc.)
Causes of False Negative Results
- Test done too early in infection (before antibodies appear - first week)
- Prior antibiotic therapy blunting the antibody response (test can be negative in up to 30% of culture-proven cases)
- Immunocompromised patients with poor antibody production
- Some strains of S. typhi with poor antigenicity
Limitations of the Widal Test
- Moderate sensitivity and specificity - can miss up to 30% of confirmed cases
- Cannot distinguish between current and past infection or vaccination
- No standardized universal cut-off - thresholds vary by region and lab
- Blood culture is negative in 40-80% of cases, and culture remains the gold standard
- Single serum specimen is unreliable; paired samples are required for meaningful interpretation
- The CDC does not recommend the Widal test for diagnosis of acute typhoid because it is difficult to interpret in endemic populations and where previous infection or vaccination may give false positives
- Results may be falsely elevated in endemic populations due to background exposure
Comparison with Gold Standard and Other Tests
| Test | Sensitivity | Specificity | Notes |
|---|---|---|---|
| Blood culture | 60-80% (40% if prior antibiotics) | High | Mainstay of diagnosis |
| Bone marrow culture | >90% | High | Gold standard; positive even with prior antibiotics |
| Stool culture | Positive from 2nd-3rd week | Moderate | |
| Widal test | Moderate | Moderate | Widely available; many limitations |
| Typhidot® | Higher than Widal | Higher | Detects IgM and IgG against 50 kD antigen of S. typhi; 3 hours |
| Typhidot-M® | Good | Good | Detects only IgM (avoids false positives from past infection) |
| IDL Tubex® | Good | Good | Detects IgM anti-O9 antibodies; results in minutes |
| Dipstick test | Moderate | Moderate | IgM antibodies against LPS; rapid |
| PCR/NAAT | Variable | High | Still under investigation for routine use |
Clinical Significance
- The Widal test remains useful in resource-limited, endemic settings where blood culture is not available
- Should be interpreted always in the clinical context - fever pattern, duration, exposure history
- A rising titer on paired sera is far more meaningful than a single positive result
- In most developed countries and high-resource settings, blood culture is preferred and the Widal test is considered obsolete
- In India and the Indian subcontinent, the Widal test is still routinely performed despite its limitations
Summary Table
| Feature | Details |
|---|---|
| Type | Agglutination (serological) test |
| Introduced | 1896 by Georges Widal |
| Target | O, H (and Vi) antibodies in patient serum |
| Best time | End of 2nd week of illness; paired sera ideal |
| O antibody titer (positive) | ≥ 1:160 (region-dependent) |
| H antibody titer (positive) | ≥ 1:640 (region-dependent) |
| Most significant finding | 4-fold rise in convalescent titer |
| Gold standard for typhoid | Bone marrow culture (>90% sensitivity) |
| Main limitation | Cannot distinguish current from past infection; false positives common in endemic areas |
| Current status | Still used in developing/endemic countries; not recommended by CDC for definitive diagnosis |
Sources:
- Park's Textbook of Preventive and Social Medicine - Laboratory Diagnosis of Typhoid
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th ed. - Serologic Methods for Salmonella
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease - Typhoid Diagnosis
- Red Book 2021 - Report of the Committee on Infectious Diseases (AAP) - CDC recommendation against Widal for acute typhoid
- CDC MMWR - Universal Precautions for Bloodborne Pathogens
This is a shared conversation. Sign in to Orris to start your own chat.