I now have all the content needed. Let me compile the comprehensive answer.
ANEMIA - Complete Overview
DEFINITION
Anemia is defined as a decrease in circulating red blood cell (RBC) mass, specifically:
- Women (non-pregnant): Hemoglobin (Hgb) < 12 g/dL or Hematocrit (Hct) < 36%
- Men: Hgb < 13 g/dL or Hct < 39%
- Pregnant women: Hgb < 11 g/dL
The severity is graded as:
| Severity | Hemoglobin |
|---|
| Mild | 10-12 g/dL (women) / 10-13 g/dL (men) |
| Moderate | 8-10 g/dL |
| Severe | < 8 g/dL |
| Very severe / life-threatening | < 6.5 g/dL |
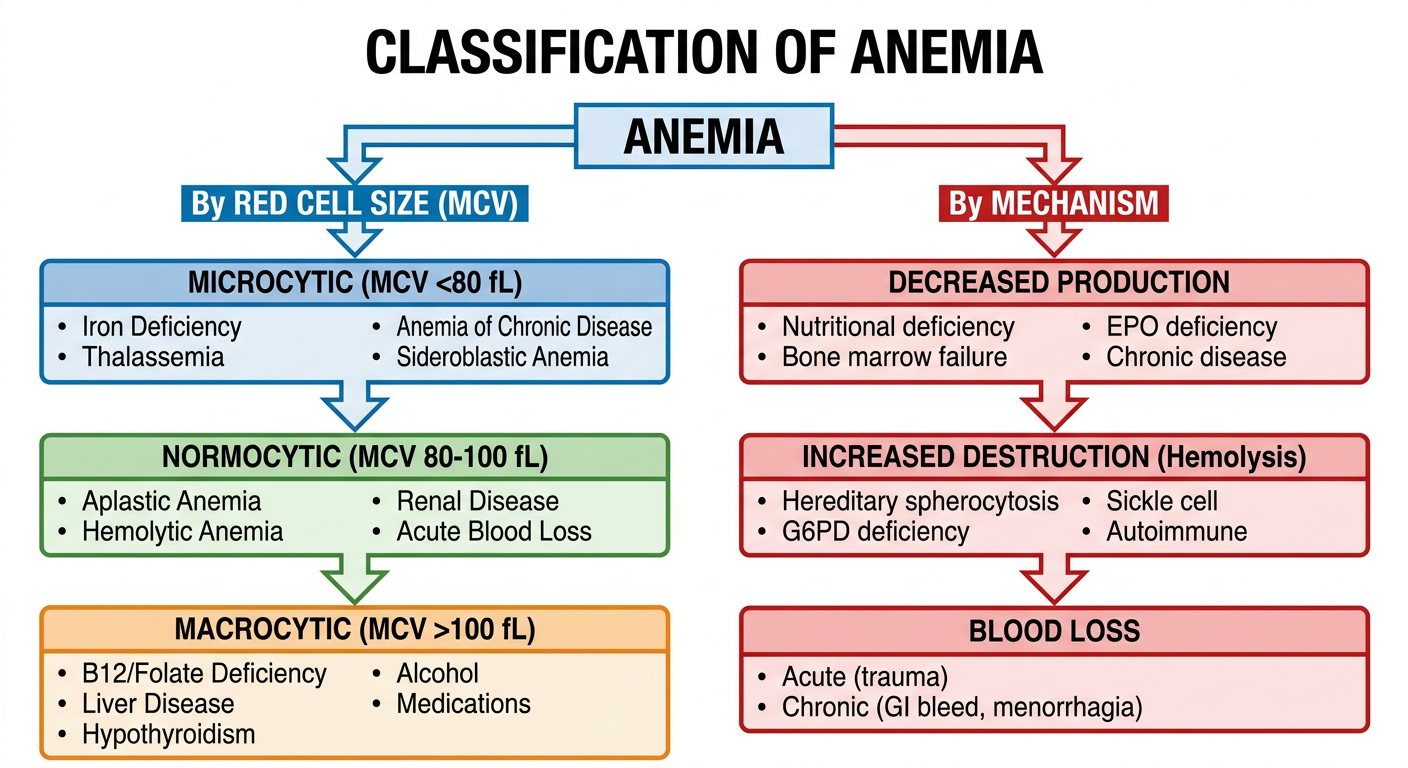
CLASSIFICATION FLOWCHART
Here is the flowchart to help you remember the classification visually:
CLASSIFICATION (Detailed)
There are two major ways to classify anemia:
1. By RED CELL SIZE (MCV-based) - Wintrobe's Classification
A. Microcytic Anemia (MCV < 80 fL)
- Any process that interferes with hemoglobin production leads to smaller red cells
- Causes (mnemonic: TAILS):
- Thalassemia - defects in globin chain synthesis
- Anemia of chronic disease (can also be normocytic)
- Iron deficiency - unable to make heme (most common cause of anemia overall)
- Lead poisoning / sideroblastic anemia - defects in heme synthesis
- Sideroblastic anemias
B. Normocytic Anemia (MCV 80-100 fL)
- Aplastic anemia
- Acute blood loss
- Hemolytic anemia (early)
- Renal disease (reduced EPO)
- Endocrinopathies (hypothyroidism early)
- Myeloma, marrow invasion
C. Macrocytic Anemia (MCV > 100 fL)
- Megaloblastic (oval macrocytes):
- Vitamin B12 deficiency
- Folate deficiency
- Medications (methotrexate, hydroxyurea, some anticonvulsants)
- Myelodysplastic syndrome
- Non-megaloblastic (round macrocytes):
- Liver disease
- Alcohol use
- Hypothyroidism
- Reticulocytosis (large reticulocytes)
- Smoking, hypoxia, dysproteinemia
2. By MECHANISM (Pathophysiologic Classification)
| Mechanism | Examples |
|---|
| Blood Loss | Acute (trauma), Chronic (GI bleed, menorrhagia) |
| Decreased RBC Production | Iron/B12/folate deficiency, aplastic anemia, EPO deficiency (renal disease), bone marrow infiltration, anemia of chronic disease |
| Increased RBC Destruction (Hemolysis) | Hereditary spherocytosis, G6PD deficiency, sickle cell, thalassemia, autoimmune hemolytic anemia, PNH, TTP/HUS, malaria |
Key tool for mechanism classification: Reticulocyte count
- Elevated reticulocytes → increased loss or destruction (blood loss or hemolysis) - the marrow is responding
- Low reticulocytes → decreased production - the marrow is failing
CAUSES
Most Common Causes by Type
| Type | Most Common Cause |
|---|
| Overall | Iron deficiency (most common worldwide) |
| Microcytic | Iron deficiency > Thalassemia trait |
| Macrocytic | B12/Folate deficiency, Alcohol, Liver disease |
| Normocytic | Anemia of chronic disease, Renal disease |
| Hemolytic | G6PD deficiency (most common inherited), Hereditary spherocytosis |
Causes of Iron Deficiency (most common anemia):
- Blood loss: Menstrual bleeding (most common in women), GI blood loss (most common in men - consider occult malignancy)
- Decreased absorption: Achlorhydria, celiac disease, bariatric surgery, H. pylori infection
- Increased requirement: Pregnancy, growth spurts, infancy
CLINICAL FEATURES
Clinical features depend on severity, chronicity, and rate of onset. Mild anemia is often asymptomatic; gradual onset allows physiologic adaptation.
Symptoms:
- Fatigue, weakness, loss of stamina
- Dyspnea on exertion
- Dizziness, tinnitus, headache
- Decreased cognitive ability, poor concentration
- Palpitations, chest pain
- Cold intolerance (especially iron deficiency)
- Pica (eating ice, clay, starch) - in ~25% of chronic iron deficiency cases
- Restless leg syndrome
Signs:
| Sign | Note |
|---|
| Pallor | Of skin, conjunctivae, palmar creases, nail beds, mucous membranes |
| Tachycardia | Compensatory |
| Wide pulse pressure | Increased stroke volume |
| Systolic flow murmur | High-output state |
| Hypotension | In severe/acute cases |
| Koilonychia (spoon nails) | Iron deficiency specifically |
| Angular cheilosis, atrophic glossitis, brittle nails | Severe, long-standing iron deficiency |
| Jaundice + splenomegaly | Hemolytic anemia |
| High-output heart failure | Severe chronic anemia |
MANAGEMENT
Step 1: Diagnosis
- CBC + peripheral smear + reticulocyte count - first-line investigation
- MCV directs the workup
- Ferritin, serum iron, TIBC, transferrin saturation (for iron deficiency)
- Vitamin B12 and folate levels (for macrocytic)
- Reticulocyte index (RI) - assesses bone marrow response
- Bone marrow biopsy if diagnosis unclear
Step 2: Treat the Underlying Cause
This is always the primary goal.
| Type | Specific Treatment |
|---|
| Iron Deficiency | Oral ferrous sulfate 325 mg TDS (best absorbed on empty stomach with vitamin C); IV iron if oral not tolerated/absorbed; treat underlying cause (GI workup if no obvious blood loss) |
| B12 Deficiency | IM cyanocobalamin (1000 mcg/day x 7 days, then weekly x 4 weeks, then monthly); or high-dose oral B12 if dietary deficiency |
| Folate Deficiency | Oral folic acid 1-5 mg/day |
| Anemia of Chronic Disease | Treat underlying disease; EPO/darbepoetin if CKD-related |
| Aplastic Anemia | Bone marrow transplant (young); antithymocyte globulin + cyclosporin (older); supportive transfusions |
| Hemolytic Anemia | Remove/treat trigger; steroids for autoimmune; splenectomy in some hereditary cases |
| Thalassemia | Transfusion + iron chelation; hydroxyurea; bone marrow transplant |
Step 3: Supportive / Symptomatic
- Blood transfusion: Reserved for severe symptomatic anemia (Hgb < 7-8 g/dL), active bleeding, cardiovascular compromise, or pre-operative optimization. Goal is not to normalize Hgb but to relieve symptoms.
- Erythropoiesis-stimulating agents (ESA): Epoetin alfa, darbepoetin - for CKD-related anemia, chemotherapy-induced anemia
- Dietary advice: Increase dietary iron (red meat, leafy greens), B12 (animal products), folate (legumes, leafy greens)
Quick Memory Aid - ANEMIA Mnemonic for Causes
| Letter | Cause |
|---|
| A | Aplastic / Autoimmune |
| N | Nutritional (Iron, B12, Folate) |
| E | Erythropoietin deficiency (Renal disease) |
| M | Malignancy / Marrow infiltration |
| I | Infection / Inflammation (chronic disease) |
| A | Acute blood loss / Hemolysis |
Sources: Washington Manual of Medical Therapeutics; Harrison's Principles of Internal Medicine 22E; Robbins & Cotran Pathologic Basis of Disease; Frameworks for Internal Medicine; Tintinalli's Emergency Medicine