Mechanism of action of ozomet vg2 in type 2 diabetes
Searching the Web
Ozomet VG2 type 2 diabetes mechanism of action
Reading File
Searching the Web
Ozomet VG2 tablet composition voglibose glimepiride metformin
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading Web Page
https://journals.lww.com/jodb/fulltext/2022/13020/expert_con…
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have all the information needed for a complete, textbook-supported answer. Here it is:
Ozomet VG2 - Mechanism of Action in Type 2 Diabetes
Ozomet VG2 is a fixed-dose combination (FDC) tablet containing three antidiabetic agents:
| Component | Class | Dose (SR formulation) |
|---|---|---|
| Glimepiride | Sulfonylurea | 2 mg |
| Metformin HCl | Biguanide | 500 mg (sustained release) |
| Voglibose | Alpha-glucosidase inhibitor | 0.2 mg |
It is approved as third-line therapy for type 2 diabetes when diet, exercise, and dual-drug therapy fail to achieve adequate glycemic control.
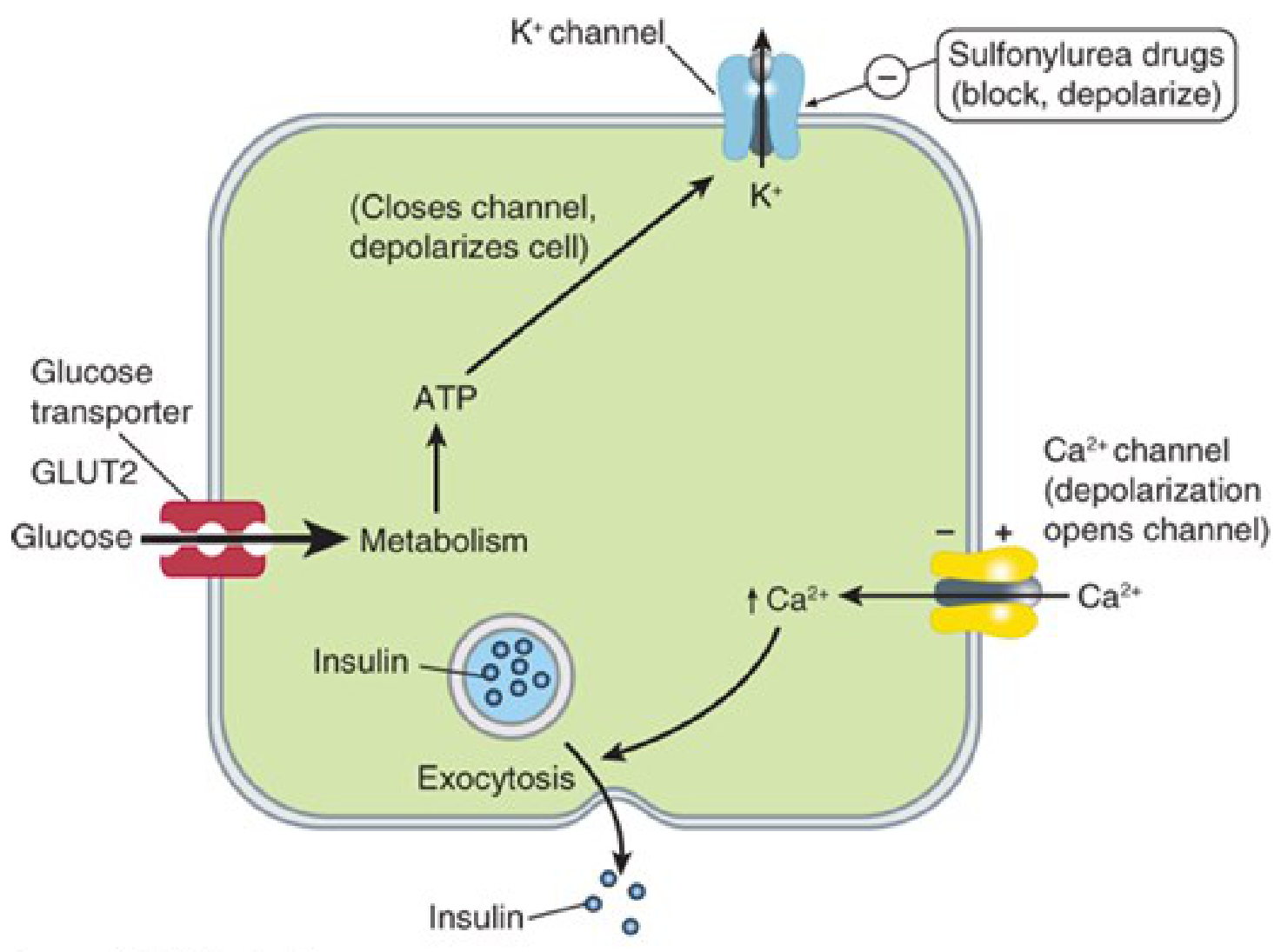
1. Glimepiride (Sulfonylurea) - Insulin Secretagogue
Target: ATP-sensitive K⁺ channels (K_ATP) on pancreatic beta cells
Mechanism:
Glimepiride binds to the SUR1 subunit of K_ATP channels on the beta cell membrane. This blocks potassium efflux, causing membrane depolarization. Depolarization opens voltage-gated Ca²⁺ channels, allowing Ca²⁺ to rush in. The resulting rise in intracellular calcium triggers exocytosis of insulin-containing granules.
Additional actions of glimepiride (beyond other sulfonylureas):
- Reduces hepatic glucose production
- Increases peripheral insulin sensitivity to a modest degree
- Has a lower hypoglycemia risk compared to older sulfonylureas (e.g., glibenclamide) because it dissociates more quickly from the SUR1 receptor
Net effect: Increases both basal and meal-stimulated insulin secretion; primarily lowers fasting blood glucose.
2. Metformin (Biguanide) - Insulin Sensitizer / Anti-gluconeogenic
Target: Mitochondrial complex I, AMPK pathway, hepatocytes
Mechanism:
- Reduces hepatic gluconeogenesis - this is its primary and most clinically significant action. Metformin inhibits mitochondrial complex I, altering the AMP:ATP ratio and activating AMP-activated protein kinase (AMPK). AMPK activation suppresses gluconeogenic gene expression (PEPCK, G6Pase), directly cutting liver glucose output - the dominant driver of fasting hyperglycemia in type 2 diabetes.
- Improves peripheral insulin sensitivity - increases glucose uptake and utilization in skeletal muscle via AMPK-mediated GLUT4 translocation.
- Slows intestinal glucose absorption - inhibits mitochondrial glycerophosphate dehydrogenase (mGPD) in enterocytes, reducing intestinal glucose uptake.
- Does NOT stimulate insulin secretion - therefore carries no independent risk of hypoglycemia.
- Additional benefits: modestly increases GLP-1 levels, promotes weight loss or stability, improves lipid profile (lowers LDL).
"The main mechanism of action of metformin is reduction of hepatic gluconeogenesis... Metformin also slows intestinal absorption of sugars and improves peripheral glucose uptake and utilization." - Lippincott Illustrated Reviews: Pharmacology
3. Voglibose (Alpha-glucosidase Inhibitor) - Postprandial Glucose Controller
Target: Alpha-glucosidase enzymes in the small intestinal brush border
Mechanism:
Voglibose competitively and reversibly inhibits the brush-border enzymes - glucoamylase, sucrase, maltase, and isomaltase - that are responsible for breaking down complex carbohydrates and disaccharides into absorbable monosaccharides. This delays hydrolysis and absorption of dietary carbohydrates, blunting postprandial glucose spikes without affecting fasting glucose significantly.
Compared to acarbose (another alpha-glucosidase inhibitor), voglibose is more selective and potent for sucrase/maltase, with fewer GI side effects.
Net effect: Primarily reduces postprandial hyperglycemia; modest effect on HbA1c.
Synergy of the Triple Combination
The three drugs act at complementary and non-overlapping points in glucose homeostasis:
| Drug | Primary Target | Blood Glucose Effect |
|---|---|---|
| Metformin | Liver (fasting glucose) | Reduces basal hyperglycemia |
| Glimepiride | Pancreatic beta cell | Boosts insulin secretion (fasting + postprandial) |
| Voglibose | Small intestinal brush border | Blunts postprandial glucose spikes |
Together they address all three key defects in type 2 diabetes:
- Hepatic insulin resistance / excess glucose output (metformin)
- Impaired beta-cell insulin secretion (glimepiride)
- Excessive postprandial carbohydrate absorption (voglibose)
Key Clinical Points
- Hypoglycemia risk: Present due to glimepiride; metformin and voglibose alone do not cause it.
- Main side effects: GI disturbance (metformin + voglibose: nausea, bloating, flatulence, diarrhea); weight gain possible from glimepiride.
- Contraindications: Renal impairment (eGFR <30 mL/min - metformin risk of lactic acidosis); inflammatory bowel disease (voglibose).
- Indication: 3rd-line FDC when dual therapy (e.g., metformin + sulfonylurea or metformin + alpha-glucosidase inhibitor) is insufficient.
Sources: Katzung's Basic & Clinical Pharmacology (16th Ed.); Lippincott Illustrated Reviews: Pharmacology; Sanofi Amaryl MV prescribing information (same FDC composition); CDSCO FDC approval 2020.

Screenshot_20260614_181259.jpg
Explain Karo Hinglish me easy
Autonomic Nervous System (ANS) - Hinglish mein Samjho! 🧠
ANS kya hota hai?
ANS = Autonomic Nervous System - yeh woh system hai jo apne aap kaam karta hai, bina tumhari marzi ke. Jaise dil dhak-dhak karna, saans lena, khana digest karna - yeh sab tum consciously nahi karte, ANS karta hai automatically!
"ANS functions largely below the level of consciousness" - matlab yeh background mein silently kaam karta rehta hai.
ANS ke 3 Parts hote hain:
| Part | Kaam |
|---|---|
| Afferents | Body se brain ko signal bhejte hain (sensory) |
| Centre | Brain/spinal cord mein processing hoti hai |
| Efferents | Brain se body ko command dete hain (motor) |
Somatic vs Autonomic - Kya Farak hai?
Imagine karo do alag delivery systems:
| Feature | Somatic NS | Autonomic NS |
|---|---|---|
| Organ supply | Skeletal muscles (jo tum hilate ho) | Baaki sab organs - heart, gut, lungs |
| Synapse kahan? | CNS ke andar | CNS ke bahar (ganglia mein) |
| Nerve fibres | Myelinated (fast) | Pre-gang = myelinated, Post-gang = non-myelinated |
| Peripheral plexus | Nahi hota | Hota hai |
| Main transmitter | Sirf Acetylcholine | Acetylcholine + Noradrenaline dono |
| Nerve kaat do toh? | Paralysis + atrophy | Activity maintain rehti hai, atrophy nahi |
ANS ke Centres kahan hain?
Hypothalamus sabse important center hai ANS ka:
- Posterior + Lateral nuclei = Sympathetic control karta hai
- Anterior + Medial nuclei = Parasympathetic control karta hai
Aur mid-brain + medulla mein bhi autonomic centres hote hain jaise:
- Pupillary (aankhon ki pupil)
- Vagal (heart rate)
- Respiratory (saans)
Autonomic Efferents - 2 Teams!
ANS ki motor side 2 teams mein banti hai:
ANS Efferents
├── Sympathetic ("Fight or Flight" - danger mein kaam aata hai)
└── Parasympathetic ("Rest and Digest" - relaxed hote time kaam aata hai)
- Zyaadatar organs ko dono ka innervation milta hai
- Yeh dono functionally antagonistic hain - matlab ek accelerate karta hai toh doosra brake lagata hai!
Easy Trick to Remember:
Somatic = Voluntary (tum control karte ho - haath uthana, paon chalana) Autonomic = Involuntary (body khud control karti hai - heartbeat, digestion, BP)
Is chapter ka main point yeh hai ki ANS ek automatic background system hai jo zindagi ke zaroori functions chalata hai, aur iska pharmacology samajhna zaroori hai kyunki drugs acting on ANS bahut saari diseases mein use hote hain - BP, asthma, heart problems, aankh ki bimariyan, etc.
Atophy? Myelinated?
Atrophy aur Myelinated - Super Simple Explanation! 😄
1. ATROPHY kya hota hai? 💪➡️😟
Atrophy = Shrink ho jaana / Kamzor ho jaana
Real life example:
Socho kisi ka haath plaster mein 2 mahine ke liye bandh kar diya. Plaster kholne ke baad woh haath patla aur kamzor ho gaya hoga - yahi hai ATROPHY!
Jab muscle ya organ ko kaam nahi karna padta toh woh dheere dheere chhota aur weak ho jaata hai.
ANS mein kyon important hai?
| Nervous System | Nerve kaat do toh? |
|---|---|
| Somatic (voluntary) | Muscle paralyzed + atrophy ho jaati hai - sookh jaati hai 😢 |
| Autonomic | Organ chalता rehta hai, atrophy nahi hoti ✅ |
Kyun? Kyunki autonomic organs (heart, gut) ke paas apna local system hota hai - woh independent hain!
2. MYELINATED kya hota hai? ⚡
Pehle samjho - Nerve fibre kya hai?
Nerve ek wire ki tarah hoti hai jo signal carry karti hai.
Myelin = Wire ka plastic cover! 🔌
Bijli wali wire dekhi hai? Uske upar plastic insulation hoti hai na?
Waise hi nerve fibre ke upar ek fatty covering hoti hai - usse kehte hain MYELIN SHEATH
Myelinated nerve:
[====|====|====|====] ← Signal "jump" karta hai (fast! ⚡)
Non-myelinated nerve:
[~~~~~~~~~~~~~~~~] ← Signal slowly crawl karta hai (slow 🐢)
Speed ka fark:
| Type | Speed | Example |
|---|---|---|
| Myelinated | Bahut fast (120 m/s tak!) | Somatic nerves - haath hatao, foran hata lete ho |
| Non-myelinated | Slow (2 m/s tak) | Autonomic post-ganglionic nerves |
ANS mein Myelinated ka scene:
Brain
|
| ← Pre-ganglionic fibre (MYELINATED = fast) ⚡
|
GANGLION (relay station)
|
| ← Post-ganglionic fibre (NON-MYELINATED = slow) 🐢
|
Heart/Gut/etc.
Pre-ganglionic = Brain se ganglion tak = Myelinated (insulated wire)
Post-ganglionic = Ganglion se organ tak = Non-myelinated (bare wire)
Quick Recap in 2 lines:
🔴 Atrophy = Use nahi kiya toh sookh/kamzor ho jaata hai organ ya muscle 🔵 Myelinated = Nerve ke upar plastic cover hai, signal fast jaata hai
Samajh aaya? 😊
Post ganglion pre ganglion?
Pre-ganglionic vs Post-ganglionic - Ekdum Simple! 🚉
Pehle samjho - GANGLION kya hai?
Ganglion = Railway Junction / Relay Station
Jaise Mumbai se Delhi jaana ho toh beech mein koi station pe train change hoti hai...
Waise hi Brain se Organ tak signal directly nahi jaata - beech mein ek STOP hota hai = GANGLION
Picture karo yeh scene:
🧠 BRAIN/SPINAL CORD
|
| ← Yeh hai PRE-GANGLIONIC fibre
| (Station aane SE PEHLE ka track)
|
🔴 GANGLION
(Relay Station)
|
| ← Yeh hai POST-GANGLIONIC fibre
| (Station ke BAAD ka track)
|
❤️ ORGAN
(Heart/Gut/Eye)
Naam se hi yaad karo!
| Word | Matlab |
|---|---|
| PRE = Pehle | Ganglion se PEHLE |
| POST = Baad mein | Ganglion ke BAAD |
| GANGLIONIC | Ganglion se related |
PRE-ganglionic = Brain ➡️ Ganglion tak POST-ganglionic = Ganglion ➡️ Organ tak
Train wala example 🚂
DELHI (Brain)
|
| 🚂 Pre-ganglionic train
|
NAGPUR (Ganglion) ← yahaan train badalni padti hai!
|
| 🚂 Post-ganglionic train
|
MUMBAI (Heart/Lungs/Gut)
- Delhi to Nagpur = Pre-ganglionic
- Nagpur to Mumbai = Post-ganglionic
- Nagpur = Ganglion (relay station)
Dono ka fark yaad karo:
| Feature | Pre-ganglionic | Post-ganglionic |
|---|---|---|
| Kahan se? | Brain/Spinal cord | Ganglion |
| Kahan tak? | Ganglion | Organ |
| Myelin? | ✅ Myelinated (fast) | ❌ Non-myelinated (slow) |
| Length | Chhoti hoti hai | Lambi hoti hai |
| Transmitter | Acetylcholine | Sympathetic = Noradrenaline, Parasympathetic = Acetylcholine |
Ek aur easy trick 🧠
"PRE = Pehle aata hai, POST = Peeche aata hai"
Ganglion ek bouncer ki tarah hai jo signal ko check karke aage bhejta hai! 😄
Real Body mein kahan hote hain Ganglia?
SYMPATHETIC ganglia:
Spinal cord ke paas hote hain
(isliye pre-ganglionic = chhoti)
(post-ganglionic = lambi, organ door hota hai)
PARASYMPATHETIC ganglia:
Organ ke paas hote hain
(isliye pre-ganglionic = lambi)
(post-ganglionic = bahut chhoti!)
Summary - 1 line mein:
🔴 Pre-ganglionic = Brain se Ganglion tak ki wire 🔵 Post-ganglionic = Ganglion se Organ tak ki wire 🟡 Ganglion = Beech ka relay station jahan signal "switch" hota hai
Ab clear hai? 😊
Neurotransmitters (Acetylcholine, Noradrenaline) kya hote hain?
Neurotransmitters - Ekdum Mast Explanation! 💬
Neurotransmitter kya hota hai?
Socho yeh scene: 📱
Tum apne dost ko WhatsApp message bhejte ho. Tumhara phone = Nerve cell (neuron) Message = Signal WhatsApp = Neurotransmitter!
Neurotransmitter = Chemical messenger jo ek nerve se doosri nerve ko (ya organ ko) message deliver karta hai!
Problem kya hai directly?
Ek nerve doosri nerve ko directly touch nahi karti!
Dono ke beech ek tiny gap hota hai jise kehte hain SYNAPSE 🕳️
NERVE 1 GAP NERVE 2
| (Synapse) |
|------> 💊💊💊💊 ---------->|
Neurotransmitters
gap cross karte hain!
Yeh chemical gap cross karke message deliver karta hai - yahi kaam hai neurotransmitter ka!
Ab dono ko samjho:
1. 🟢 ACETYLCHOLINE (ACh)
Nickname: "The Gentle Messenger"
Kahan milta hai?
✅ SAARE Pre-ganglionic fibres mein
(Sympathetic + Parasympathetic dono)
✅ SAARE Parasympathetic post-ganglionic fibres mein
✅ Somatic nerves mein (skeletal muscle ke liye)
✅ Sweat glands mein (special case!)
Kya karta hai?
Parasympathetic system ka main messenger hai -
"Rest and Digest" promote karta hai:
| Body Part | ACh ka effect |
|---|---|
| ❤️ Heart | Rate slow karta hai |
| 👁️ Eye | Pupil chhoti karti hai |
| 🫁 Lungs | Airways narrow karta hai |
| 🍽️ Gut | Digestion badhaata hai |
| 💧 Glands | Secretion badhaata hai |
Easy yaad karo:
ACh = "Aaram Chaho" = Rest and Digest! 😴
2. 🔴 NORADRENALINE (NA) / Norepinephrine
Nickname: "The Fighter Messenger"
Kahan milta hai?
✅ Sympathetic POST-ganglionic fibres mein
(mostly)
❌ Parasympathetic mein NAHI hota
Kya karta hai?
Sympathetic system ka main messenger -
"Fight or Flight" promote karta hai:
| Body Part | NA ka effect |
|---|---|
| ❤️ Heart | Rate fast karta hai |
| 👁️ Eye | Pupil badi karti hai |
| 🫁 Lungs | Airways khulti hain (breathe easy) |
| 💪 Muscles | Blood flow badhta hai |
| 🍽️ Gut | Digestion slow hoti hai |
Easy yaad karo:
NA = "Nahin Aaram" = Fight and Flight! 😤⚡
Dono ka Comparison - Side by Side:
| Feature | Acetylcholine 🟢 | Noradrenaline 🔴 |
|---|---|---|
| System | Parasympathetic (mainly) | Sympathetic (mainly) |
| Mood | Chill, relaxed 😴 | Alert, excited 😤 |
| Heart rate | ⬇️ Slow | ⬆️ Fast |
| Pupils | ⬇️ Chhoti | ⬆️ Badi |
| Digestion | ⬆️ Better | ⬇️ Slow |
| Breakdown by | Acetylcholinesterase enzyme | MAO + COMT enzymes |
SUPER EASY TRICK - Dono yaad karo! 🎯
Situation 1: Exam hall mein tension 😰
Sympathetic activate ➡️ NORADRENALINE release
- Dil tez dhak dhak 💓
- Aankhein khuli khuli 👀
- Paet mein butterflies 🦋
- Haath thoda kaanpna
Situation 2: Sunday dopahar - khana khaake sofa pe 😴
Parasympathetic activate ➡️ ACETYLCHOLINE release
- Dil slow aur steady 💤
- Aankhein chhoti 😌
- Khana digest ho raha hai 🍽️
- Full relax mode
Where exactly does release happen?
🧠 Brain
|
| ACh released here
↓
🔴 GANGLION
|
|-- Parasympathetic ➡️ ACh released at organ
|
|-- Sympathetic ➡️ NA released at organ
↓
❤️🫁🍽️ ORGANS
Drugs ka connection (important for pharma!) 💊
Yahi wajah hai kyun itne drugs ANS pe kaam karte hain:
| Drug type | Kya karta hai |
|---|---|
| Beta blockers (atenolol) | NA ka effect block karta hai - BP kam karta hai |
| Atropine | ACh ka effect block karta hai - Heart fast karta hai |
| Neostigmine | ACh ko zyada time tak rakhhta hai - muscles strong karta hai |
1 Line Summary:
🟢 Acetylcholine = "Aaram Chaho" chemical - Rest & Digest, sab slow karo 🔴 Noradrenaline = "Nahin Aaram" chemical - Fight & Flight, sab fast karo 💬 Dono chemicals hain jo nerve ke gap (synapse) mein jump karke message deliver karte hain!
Kuch aur poochna hai? 😊
Autonomic nervous system ke receptors (alpha, beta, muscarinic, nicotinic) explain karo
ANS Receptors - Hinglish mein Mast Explanation! 🎯
Pehle Samjho - Receptor kya hota hai?
Lock and Key 🔑
Neurotransmitter ek CHABI hai Receptor ek TAALA haiJab sahi chabi sahi taale mein lage - DOOR KHULTI HAI = Effect hota hai!
Noradrenaline 🔑 + Alpha Receptor 🔒 = Effect! ✅
Acetylcholine 🔑 + Muscarinic 🔒 = Effect! ✅
Wrong key 🔑 + Wrong lock 🔒 = Kuch nahi ❌
Receptors ka Family Tree 🌳
ANS RECEPTORS
│
├── 🔴 ADRENERGIC (Noradrenaline/Adrenaline ke liye)
│ ├── Alpha (α) receptors
│ │ ├── α1
│ │ └── α2
│ └── Beta (β) receptors
│ ├── β1
│ ├── β2
│ └── β3
│
└── 🟢 CHOLINERGIC (Acetylcholine ke liye)
├── Muscarinic (M) receptors
│ ├── M1, M2, M3...
└── Nicotinic (N) receptors
├── Nn (Neural)
└── Nm (Muscle)
🔴 ADRENERGIC RECEPTORS
(Noradrenaline/Adrenaline wale)
ALPHA (α) Receptors
α1 Receptor
Location: Blood vessels ki walls mein (smooth muscle)
Effect: CONTRACTION = Tightening
NA ➡️ α1 receptor ➡️ Blood vessel TIGHT ho jaati hai
➡️ BP BADHTA HAI ⬆️
Yaad karo:
α1 = "Aao Blood pressure Badhao" - vessels squeeze karo!
Real examples:
| Organ | α1 effect |
|---|---|
| 🩸 Blood vessels | Contract - BP up |
| 👁️ Pupil (iris) | Dilate - badi pupil |
| 🚽 Bladder neck | Contract - urine rok lo |
| 🏃 Naak ki vessels | Contract - naak band |
α2 Receptor
Location: Pre-synaptic nerve endings pe (feedback system!)
Effect: Noradrenaline release ROKTA hai - braking system!
Bahut zyada NA release hua
↓
α2 receptor activate
↓
"Bas karo! Bahut ho gaya!"
↓
NA release BAND 🛑
Yaad karo:
α2 = "Arre Ruko" receptor - Auto-braking system!
BETA (β) Receptors
β1 Receptor
Location: ❤️ HEART mein mainly!
Effect: Heart pe sab kuch BADHATA hai
NA/Adrenaline ➡️ β1 ➡️ Heart rate ⬆️ (tachycardia)
➡️ Heart force ⬆️ (strong beats)
➡️ Conduction speed ⬆️
Yaad karo:
β1 = "Be-1 = Beat-1" - Heart BEAT badhao! 💓
Clinically important:
Beta blockers (atenolol, metoprolol) = β1 block karte hain = Heart slow karte hain = BP kam karte hain!
β2 Receptor
Location: 🫁 Lungs (bronchi), uterus, blood vessels of muscles
Effect: RELAXATION = Khulna
Adrenaline ➡️ β2 ➡️ Bronchi KHULTI hai ⬆️ (bronchodilation)
➡️ Uterus relax hoti hai
➡️ Muscle vessels dilate
Yaad karo:
β2 = "Breathe-2" = Saas lo aasaan se! 🌬️
Clinically important:
Salbutamol (Asthalin) = β2 agonist = Asthma mein bronchi kholta hai!
β3 Receptor
Location: 🧈 Fat cells (adipose tissue), Bladder
Effect: Fat breakdown (lipolysis), Bladder relax
Mostly research mein important, clinically less discussed abhi
Alpha vs Beta - Quick Comparison:
| Alpha (α) | Beta (β) | |
|---|---|---|
| Main action | CONTRACTION | RELAXATION (mostly) |
| Blood vessels | Tight karta hai | Kholta hai (β2) |
| Heart | Less effect | Tez karta hai (β1) |
| Lungs | Less | Kholta hai (β2) |
| Drug example | Phenylephrine | Salbutamol, Atenolol |
🟢 CHOLINERGIC RECEPTORS
(Acetylcholine wale)
ACh ke 2 types ke receptors hain - naam plants se aaya hai! 🌿
MUSCARINIC Receptors 🍄
Naam kahan se aaya?
Muscarine = Ek mushroom (Amanita muscaria) ka poison hai Woh poison inhib karta tha... aur researchers ne socha - "Yeh toh ACh jaisa kaam kar raha hai kuch jagah!" Toh un receptors ka naam rakha Muscarinic 🍄
Location:
✅ Saare PARASYMPATHETIC post-ganglionic target organs
✅ Sweat glands (sympathetic hain but ACh use karte hain!)
✅ Brain mein bhi
Types (M1, M2, M3):
| Type | Location | Effect |
|---|---|---|
| M1 | Brain, stomach | Memory, gastric acid |
| M2 | ❤️ Heart | Heart rate SLOW ⬇️ |
| M3 | Glands, smooth muscle, eye | Secretions, contraction, pupil chhoti |
Effects yaad karo - "SLUDD" trick! 🧠
S - Salivation (laala zyada)
L - Lacrimation (aansu zyada)
U - Urination (peshab zyada)
D - Defecation (potty zyada)
D - Digestion (gut movement zyada)
SLUDD = Parasympathetic = Muscarinic = ACh ka effect!
Clinically important:
| Drug | Kya karta hai |
|---|---|
| Atropine | Muscarinic BLOCK karta hai - heart tez, pupil badi, dry mouth |
| Pilocarpine | Muscarinic activate - glaucoma mein pupil chhoti |
| Organophosphate (pesticide) | Muscarinic bahut zyada activate - SLUDD overdose = poisoning! |
NICOTINIC Receptors 🚬
Naam kahan se aaya?
Nicotine = Cigarette ka chemical Nicotine inhib karta tha... aur researchers ne socha same cheez! Toh naam rakha Nicotinic 🚬
Location:
✅ SAARE Ganglia mein
(Sympathetic + Parasympathetic dono ke!)
✅ Neuromuscular Junction
(Nerve se skeletal muscle ka connection!)
✅ Adrenal medulla mein
2 Types:
| Type | Full name | Location | Effect |
|---|---|---|---|
| Nn | Nicotinic Neural | Ganglia | Signal ganglia se aage bhejo |
| Nm | Nicotinic Muscle | Neuromuscular junction | Muscle contract karo! |
Kaise kaam karta hai?
ACh ➡️ Nicotinic receptor ➡️ Ion channel KHULTA hai
➡️ Na+ andar aata hai
➡️ DEPOLARIZATION
➡️ Action potential
➡️ EFFECT!
Nicotinic = Fast acting (ion channel direct khulta hai!) Muscarinic = Slow acting (G-protein pathway se)
Clinically important:
| Drug | Kya karta hai |
|---|---|
| Succinylcholine | Nm block - surgery mein muscle relax |
| Tubocurarine | Nm block - paralysis for surgery |
| Hexamethonium | Nn block - ganglionic blocker |
| Nicotine patch | Nn stimulate - smoking cessation |
MASTER TABLE - Sabka Summary! 📊
| Receptor | Neurotransmitter | Location | Main Effect | Important Drug |
|---|---|---|---|---|
| α1 | Noradrenaline | Blood vessels | Vasoconstriction, BP ⬆️ | Phenylephrine |
| α2 | Noradrenaline | Pre-synaptic | NA release rokna 🛑 | Clonidine |
| β1 | Noradrenaline | ❤️ Heart | HR ⬆️, Force ⬆️ | Atenolol (blocker) |
| β2 | Adrenaline | 🫁 Lungs | Bronchodilation | Salbutamol |
| M (Muscarinic) | Acetylcholine | Organs (parasympathetic) | SLUDD effects | Atropine (blocker) |
| Nn (Nicotinic) | Acetylcholine | Ganglia | Signal transmission | Hexamethonium |
| Nm (Nicotinic) | Acetylcholine | Muscle | Contraction | Succinylcholine |
FINAL SUPER TRICK 🎯
SYMPATHETIC = ADRENERGIC receptors
= Alpha (vessels tight) + Beta (heart & lungs)
= "NA/Adrenaline ke taale"
PARASYMPATHETIC = CHOLINERGIC receptors
= Muscarinic (organs pe SLUDD)
= "ACh ke taale"
GANGLIA = Nicotinic receptors
= DONO systems mein same!
= "Common relay station ka taala"
🔴 Alpha = Squeeze/tighten (mainly vessels) 🔴 Beta = Heart tez (β1) + Lungs kholo (β2) 🟢 Muscarinic = Parasympathetic effects (SLUDD + heart slow) 🟢 Nicotinic = Ganglia + Muscles (fast ion channel)
Koi specific receptor aur detail mein samjhna hai? 😊
This is a shared conversation. Sign in to Orris to start your own chat.