Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
I now have all the core content needed. Let me compile the comprehensive answer.
Growth Hormone: Secretion, Actions, Regulation, and IGF-1
1. Source and Chemistry
Growth hormone (GH), also called somatotropin, is a 191-amino acid single-chain polypeptide with two internal disulfide bridges. It is synthesized and secreted by somatotrophs scattered throughout the anterior pituitary. The GH gene resides on chromosome 17 and is a member of a gene family that includes prolactin (16% homology) and human placental lactogen (80% homology). GH exists in at least three molecular forms; the predominant circulating form is the 22-kDa monomer.
- Costanzo Physiology 7th ed., p. 411
- Medical Physiology (Boron & Boulpaep), p. 1458
2. Pulsatile Secretion
GH is secreted in a pulsatile pattern, with secretory bursts occurring approximately every 2 hours throughout the day. The largest and most consistent burst occurs within the first hour of slow-wave sleep (stages III and IV). Between pulses, basal GH levels are very low or undetectable.
Graph - GH secretion over 24 hours:
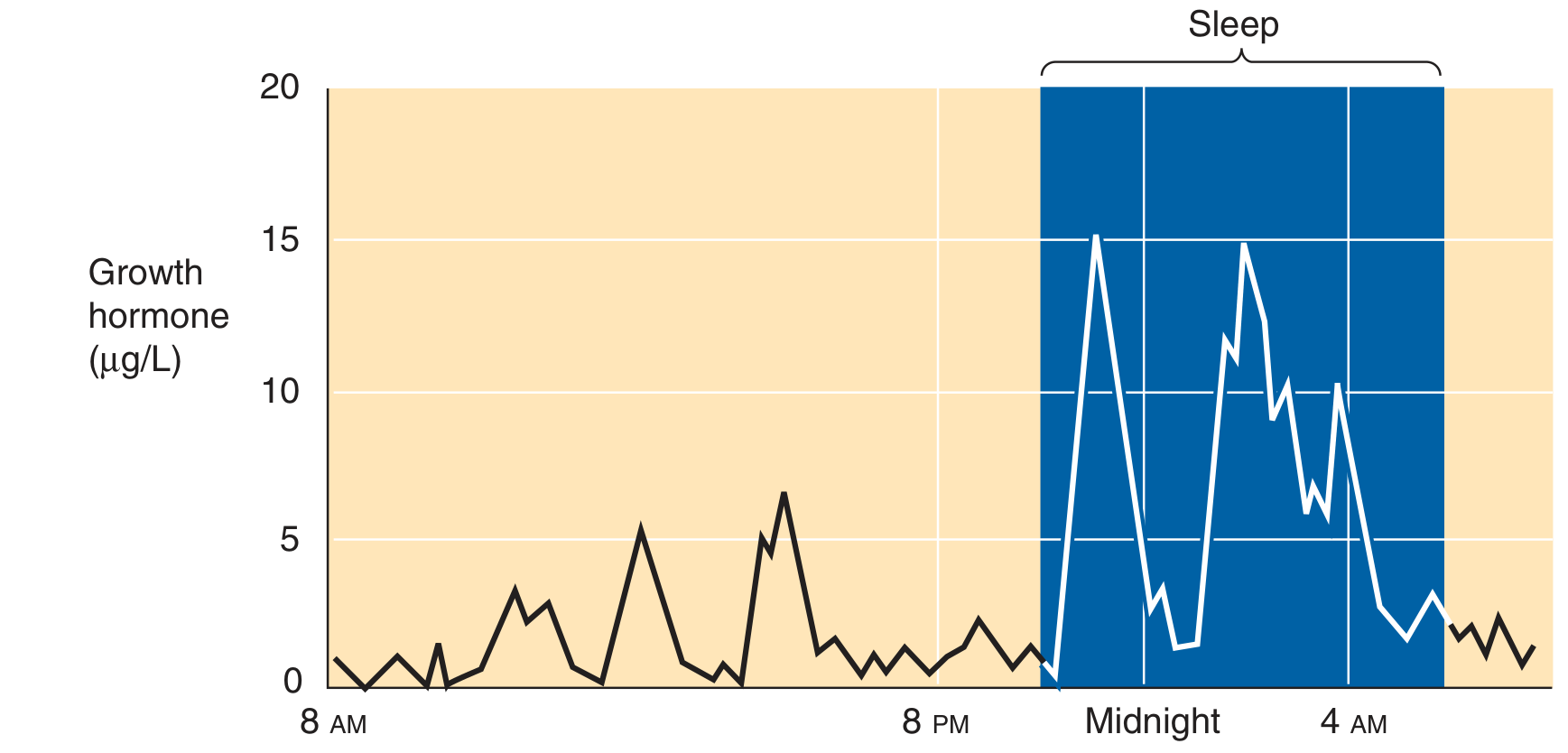
The graph shows low, irregular GH pulses during daytime waking hours, with dramatically elevated, high-amplitude secretory bursts during the sleep period (shaded blue). The highest peaks occur around midnight to 2 AM (slow-wave sleep).
- Medical Physiology, p. 1460
3. Regulation of Secretion
GH secretion is governed by the interplay of three hypothalamic/peripheral regulators and multiple feedback loops.
3a. GHRH (Growth Hormone-Releasing Hormone)
- Produced exclusively in neurons of the arcuate nucleus of the hypothalamus
- A 40- or 44-amino acid peptide (full biological activity in first 29 amino acids)
- Binds specific receptors on somatotrophs; signals via Gs protein → adenylyl cyclase (↑cAMP) and phospholipase C (↑IP3/Ca²+)
- Net effect: stimulates both synthesis and secretion of GH
3b. Somatostatin (SRIF - Somatotropin Release-Inhibiting Factor)
- Also released from the hypothalamus (periventricular nucleus)
- Binds its own receptor on somatotrophs, coupled to Gi protein → ↓cAMP
- Blocks the action of GHRH on somatotrophs, inhibiting GH secretion
- The pulsatile pattern of GH reflects the alternating dominance of GHRH surges vs. somatostatin withdrawal
3c. Ghrelin
- A 28-amino acid peptide produced mainly by oxyntic (P/D1) cells of the stomach
- The endogenous ligand for the GH secretagogue (GHS) receptor on pituitary somatotrophs and hypothalamic neurons
- Potently stimulates GH release, stimulates appetite, and regulates glucose metabolism
- Its physiological interaction with GHRH and somatostatin is complex; it acts synergistically with GHRH
| Stimulatory | Inhibitory |
|---|---|
| Hypoglycemia (↓blood glucose) | Hyperglycemia (↑blood glucose) |
| ↑Amino acids (e.g., arginine) | ↑Free fatty acids |
| Fasting / starvation | Obesity |
| Exercise | Somatostatin |
| Stress (trauma, fever) | Somatomedins (IGF-1) |
| Slow-wave sleep (III & IV) | GH itself (short-loop) |
| Puberty (estrogen, testosterone) | Senescence |
| α-Adrenergic agonists | β-Adrenergic agonists |
- Costanzo Physiology 7th ed., p. 413; Basic Medical Biochemistry 6e, p. 1482
4. GH-IGF-1 Axis Flowchart
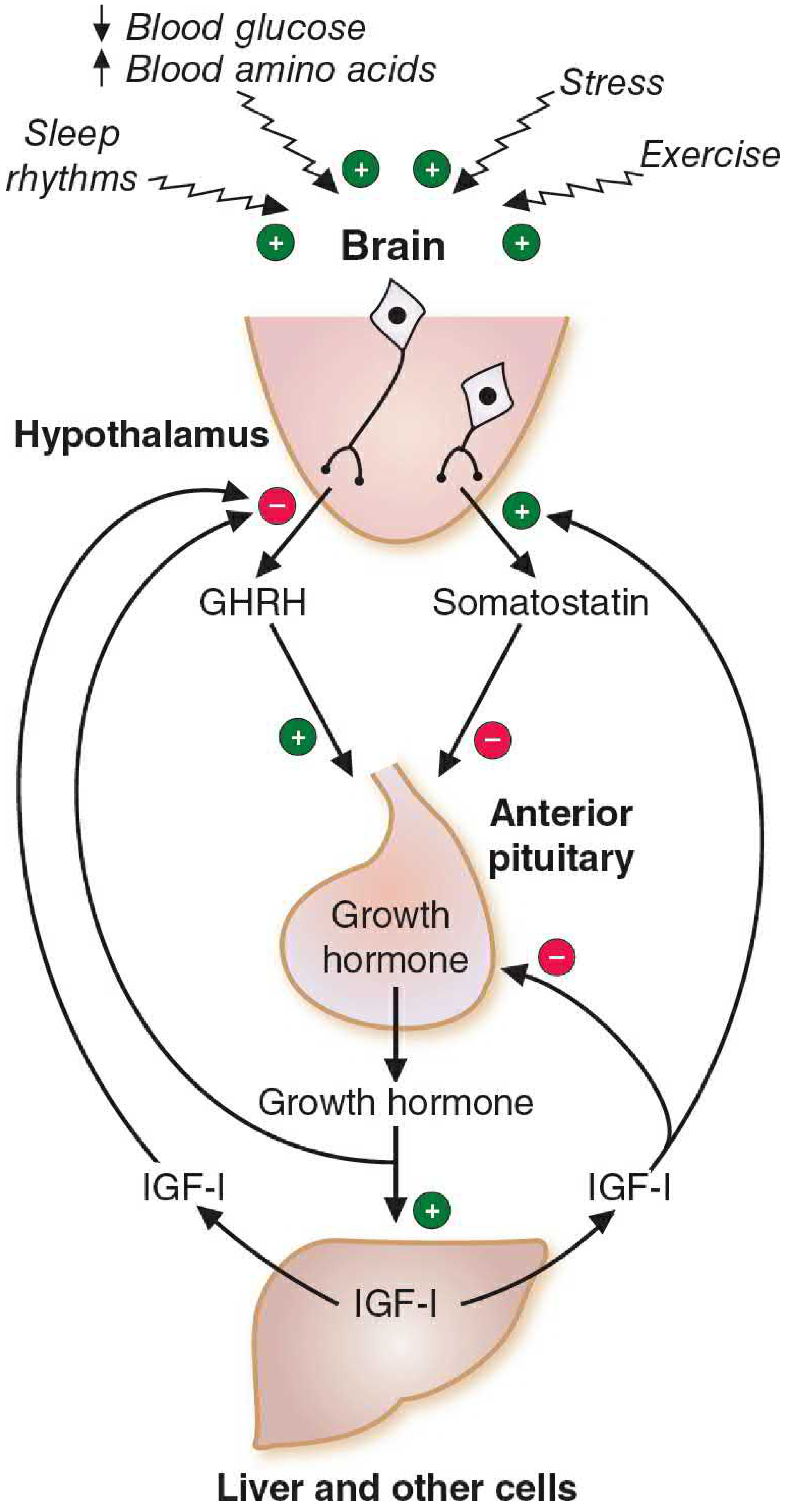
The diagram shows: stimuli (↓blood glucose, ↑amino acids, sleep, stress, exercise) → brain → hypothalamus releases GHRH (+) and somatostatin (-) → anterior pituitary somatotrophs release GH → GH stimulates liver and other cells to produce IGF-I → IGF-I feeds back negatively to inhibit both GHRH (at hypothalamus) and GH release (at pituitary), and stimulates somatostatin release.
5. Feedback Regulation
Three feedback loops control GH secretion (all negative):
- Ultrashort loop: GHRH inhibits its own release from the hypothalamus
- Short loop: GH itself inhibits somatotrophs directly (short-loop feedback), and stimulates somatostatin secretion from the hypothalamus
- Long loop (IGF-1-mediated):
- Circulating IGF-1 acts directly on somatotrophs to suppress GH secretion (via tyrosine kinase receptor, independent of cAMP)
- IGF-1 suppresses GHRH release from the hypothalamus
- IGF-1 increases somatostatin secretion from the hypothalamus
The net result: any rise in GH → rises in IGF-1 → shut down further GH secretion at both pituitary and hypothalamic levels.
- Medical Physiology, p. 1641-1643; Costanzo Physiology, p. 415
6. Actions of Growth Hormone
GH has both direct (short-term, acute) and indirect (long-term, growth-promoting via IGF-1) actions.
6a. Direct Metabolic Actions (Anti-Insulin / "Diabetogenic")
GH acts via a tyrosine kinase-associated receptor (JAK2 family) - a type I cytokine receptor. One GH molecule bridges two GHR monomers, causing dimerization and JAK2 activation → STAT transcription factors + MAP kinase/AKT pathways.
| Target Tissue | Direct Effect |
|---|---|
| Muscle | ↓ Glucose uptake; ↑ amino acid transport; ↑ lean mass; ↑ N₂ retention |
| Adipose | ↑ Lipolysis; ↑ hormone-sensitive lipase; ↓ lipogenesis; ↓ glucose transport |
| Liver | ↑ Gluconeogenesis; insulin resistance |
| Overall | Insulin resistance ("diabetogenic effect") |
Chronic GH excess (e.g., acromegaly) → frank diabetes mellitus via persistent insulin resistance.
6b. Growth-Promoting Actions via IGF-1
Long-term growth-promoting effects of GH are largely indirect, mediated by IGF-1 (somatomedin C). GH stimulates hepatocytes and other tissues to synthesize and secrete IGF-1.
IGF-1 then acts on target tissues (bone, cartilage, muscle, viscera) through IGF-1 receptors (structurally similar to the insulin receptor; intrinsic tyrosine kinase activity with autophosphorylation).
Key growth-promoting effects:
-
Stimulates chondrocyte proliferation at epiphyseal growth plates → linear bone growth (only before epiphyseal closure)
-
After epiphyseal closure → periosteal bone thickening (as in acromegaly)
-
Stimulates protein synthesis and positive nitrogen balance
-
Promotes organ growth (muscle, heart, liver, kidneys, GI tract)
-
Cell proliferation and differentiation (autocrine/paracrine)
-
Costanzo Physiology, p. 415-416; Medical Physiology, p. 1658
7. Age-Related Changes in GH Secretion
| Life Stage | GH Secretion |
|---|---|
| Birth | Normal size; GH not essential in utero |
| Infancy-childhood | Gradually increases; required for linear growth |
| Puberty | Enormous surge (estrogen in females, testosterone in males → increased pulse frequency + amplitude) → pubertal growth spurt |
| Adulthood | Declines to stable lower level |
| Senescence | Further decline; lowest levels; ↓ pulse frequency and magnitude (somatopause) |
GH deficiency from birth → pituitary dwarfism. GH excess from childhood → gigantism. GH excess after epiphyseal closure → acromegaly (no lengthening of long bones, but coarsening of features, enlargement of hands/feet, joint deformity, hypertension, cardiomegaly).
8. Note on IGF-1 (Insulin-Like Growth Factor-1)
Structure: IGF-1 (somatomedin C) is a 70-amino acid single-chain polypeptide structurally homologous to proinsulin, with three domains (A, B, C) - unlike insulin, the C-domain is not cleaved from IGF-1. It also has a unique D-domain.
Source: The liver is the primary source of circulating IGF-1 (endocrine actions). IGF-1 is also produced locally in bone, muscle, kidney, and cartilage (autocrine/paracrine actions).
Regulation of synthesis: GH is the principal driver of IGF-1 synthesis. Because GH is secreted pulsatilely, IGF-1 integrates and smooths GH secretion over time - plasma IGF-1 levels are therefore more stable than GH and serve as a better marker of overall GH status. IGF-1 levels also depend on nutritional state (fall in malnutrition even with normal GH).
Transport: >95% of circulating IGF-1 is bound to IGF-binding proteins (IGFBPs), especially IGFBP-3. IGFBP-3 itself is GH-dependent. This greatly prolongs the half-life of IGF-1 (hours vs. minutes for free GH).
Actions of IGF-1:
- Growth promotion: chondrocyte and osteoblast proliferation, linear growth
- Protein anabolism: ↑ amino acid uptake and protein synthesis
- Metabolic: acute insulin-like effects (glucose uptake, anti-lipolysis) - can cause hypoglycemia at high doses
- Feedback: inhibits GH secretion (both at pituitary and hypothalamus, as above)
- Stimulates organ growth throughout the body
Clinical relevance: IGF-1 measurement is used clinically as a screening test for acromegaly (elevated) and GH deficiency (low). The IGF-1 level reflects mean 24-hour GH secretion far more accurately than a single random GH level (which could be at a nadir).
- Medical Physiology (Boron & Boulpaep), p. 1658-1675
- Costanzo Physiology 7th ed., p. 414-416
- Basic Medical Biochemistry 6e, p. 1481-1485
- Henry's Clinical Diagnosis, p. 610-612
This is a shared conversation. Sign in to Orris to start your own chat.