Surface marking of lung
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Excellent content retrieved. Here is a complete, well-organized answer:
Surface Markings of the Lung
Surface markings allow clinicians to project the boundaries of the lungs, pleura, and their lobes onto the body surface using palpable landmarks.
Apex
The apex of each lung projects 2.5 cm above the medial third of the clavicle (or up to the level of the neck of the first rib), extending into the root of the neck. The parietal pleura projects above the first costal cartilage superiorly.
Anterior Border
- Right lung: Passes from the apex downward to the sternoclavicular joint, then descends vertically close to the midline, behind the sternum, reaching the level of the 6th costal cartilage.
- Left lung: Follows a similar course down to the 4th costal cartilage, where it deviates laterally to form the cardiac notch (because the heart bulges into the left pleural cavity). It then curves back medially and reaches the 6th costal cartilage. This creates the costomediastinal recess on the left.
Inferior Border (Lung Margin)
In quiet respiration, the lower margin of the lung follows a VI, VIII, X contour:
| Reference Line | Rib Level |
|---|---|
| Midclavicular line | Rib VI |
| Midaxillary line | Rib VIII |
| Posterior (paravertebral) | Vertebra TX |
Note: The parietal pleura (costodiaphragmatic recess) lies two rib spaces below the lung margin at each reference line (VIII, X, XII), forming a potential space for fluid collection.
Posterior Border
Both lungs extend posteriorly close to the vertebral column, from the apex down to the 10th thoracic vertebra (TX). The parietal pleura descends to vertebra TXII posteriorly.
Fissures and Lobes
Oblique Fissure (Both Lungs)
The oblique fissure is present in both right and left lungs. Its surface marking:
- Posteriorly: Begins at the spinous process of T4 (TIV) in the midline
- Courses inferolaterally, crossing the 4th and 5th intercostal spaces
- Laterally: Crosses rib V at the midaxillary line
- Anteriorly: Follows the contour of rib VI and its costal cartilage
Practical tip: When the patient raises their arms with hands behind their head, the medial border of the scapula parallels the oblique fissure - a useful bedside guide.
For the left lung, the oblique fissure is slightly more oblique, beginning between the spinous processes of TIII and TIV.
Horizontal Fissure (Right Lung Only)
The horizontal fissure separates the upper lobe from the middle lobe:
- Follows the 4th intercostal space from the sternum anteriorly
- Meets the oblique fissure where it crosses rib V laterally
- In the anterior view, it follows the contour of rib IV and its costal cartilage
Summary Table
| Feature | Surface Marking |
|---|---|
| Apex | 2.5 cm above medial clavicle |
| Inferior border (MCL) | Rib VI |
| Inferior border (MAL) | Rib VIII |
| Inferior border (posterior) | T10 |
| Pleural reflection (MCL) | Rib VIII |
| Pleural reflection (MAL) | Rib X |
| Pleural reflection (posterior) | T12 |
| Oblique fissure (posterior start) | T4 spine |
| Oblique fissure (lateral) | Rib V at midaxillary line |
| Oblique fissure (anterior end) | Rib VI / 6th costal cartilage |
| Horizontal fissure (anterior) | 4th intercostal space / rib IV |
| Horizontal fissure (lateral) | Rib V at midaxillary line |
Anterior and Posterior Views
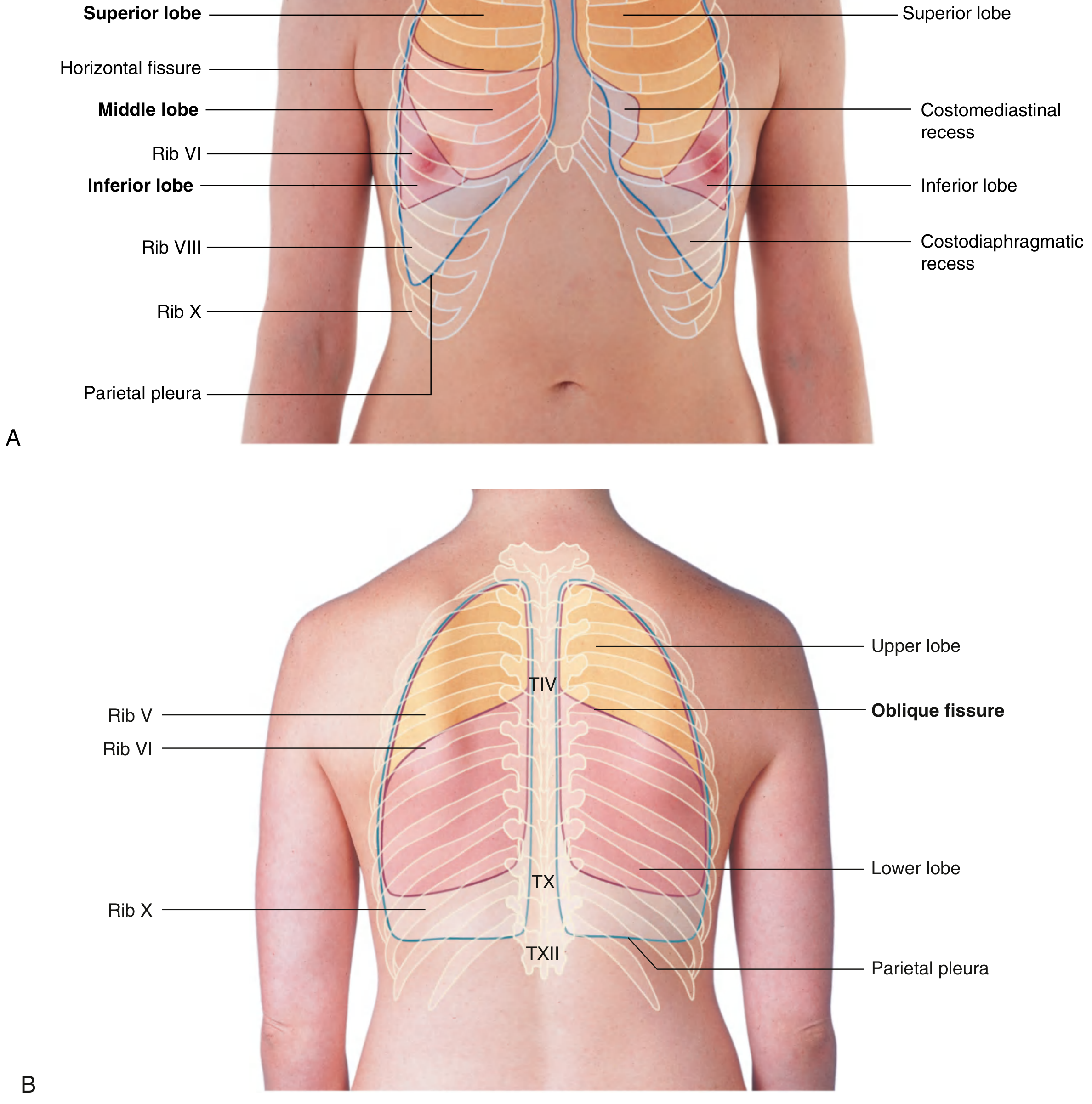
Fig. 3.114 - Anterior view (A) showing right superior, middle, and inferior lobes with horizontal fissure at rib VI, inferior lobe reaching rib VIII/X; Posterior view (B) showing upper and lower lobes separated by oblique fissure at TIV, lower margin at TX/TXII.
Lateral and Posterior Views with Arm Abducted
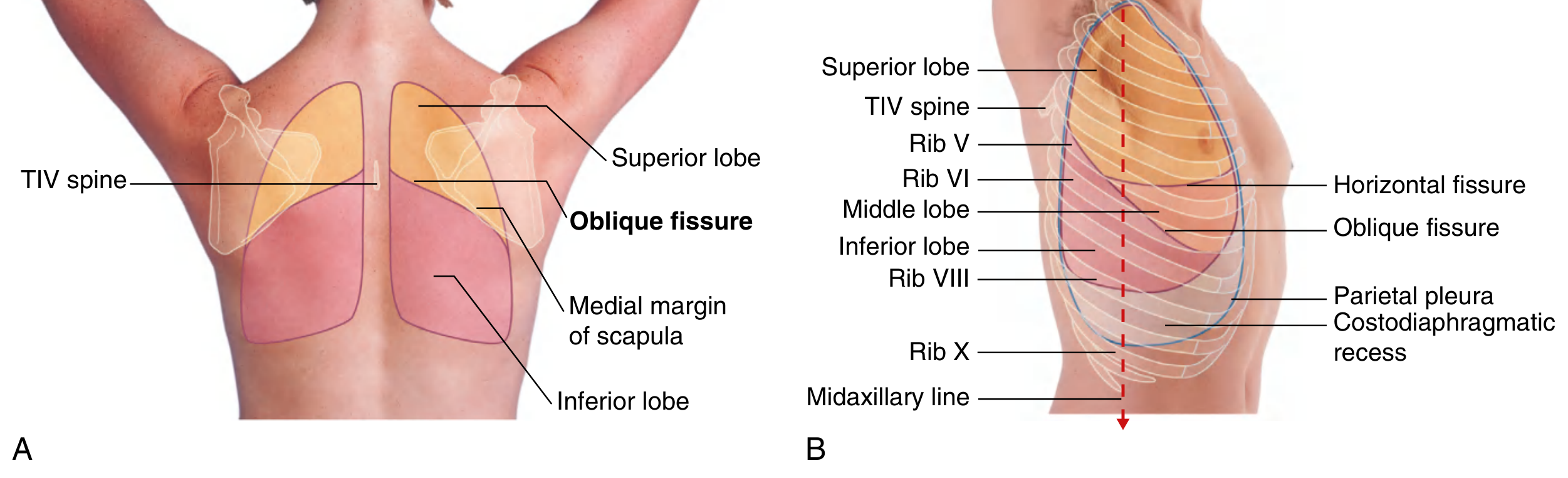
Fig. 3.115 - (A) Posterior view with arms raised: the medial border of the scapula parallels the oblique fissure. (B) Lateral view showing the complete course of both fissures.
Clinical Relevance
- The costodiaphragmatic recess (between lung margin and pleural reflection) is the lowest potential space - pleural effusions collect here first and can be detected by dullness on percussion below the lung's inferior margin.
- The costomediastinal recess is present anteriorly on the left due to the cardiac notch.
- Because the posterior surface is largely lower lobe, auscultation over the back mainly samples the lower lobe (both sides). The upper lobes are best heard anteriorly and apically.
- The middle lobe of the right lung lies mainly adjacent to the lower anterior chest wall and is heard best in the right axilla and right lower anterior chest.
- Gray's Anatomy for Students, pp. 205-206, 277-279
Retry
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Surface Markings of the Lung
Surface markings project the lung boundaries and their lobes onto the body surface using palpable bony landmarks.
Lungs - Basic Structure
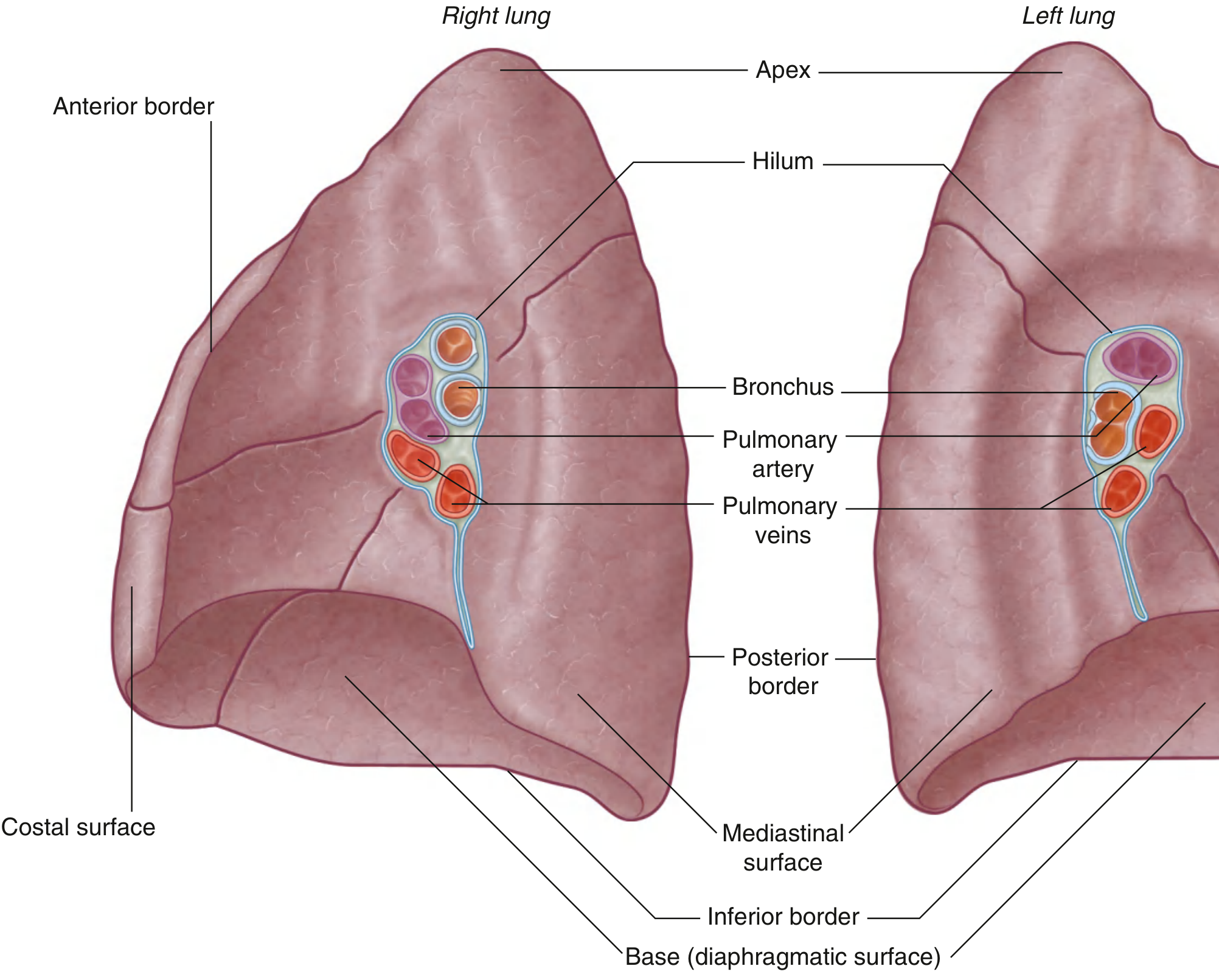
Fig. 3.44 - The right and left lungs showing their borders and surfaces.
1. Apex
- Projects 2.5 cm above the medial third of the clavicle into the root of the neck
- Corresponds to the level of the neck of the 1st rib
- The parietal pleura (cervical pleura) also projects superiorly above the first costal cartilage at this point
2. Anterior Border
Right lung:
- Descends from the apex to the sternoclavicular joint
- Runs vertically downward close to the midline, posterior to the sternum
- Reaches the 6th costal cartilage where it turns to become the inferior border
Left lung:
- Follows the same course as the right down to the 4th costal cartilage
- Then deviates laterally to form the cardiac notch (due to the heart bulging into the left pleural cavity)
- Curves back medially as the lingula and meets the inferior border at the 6th costal cartilage
- This deviation creates the costomediastinal recess anteriorly on the left
3. Inferior Border (Lung Margin)
In quiet respiration, the inferior margin follows a VI - VIII - X pattern:
| Reference Line | Lung Inferior Border |
|---|---|
| Midclavicular line (MCL) | Rib VI |
| Midaxillary line (MAL) | Rib VIII |
| Posterior / paravertebral | Vertebra TX (T10) |
4. Posterior Border
- Runs vertically close to the vertebral column on each side
- Extends from the apex down to the level of vertebra TX posteriorly
5. Pleural Reflection (vs. Lung Margin)
The parietal pleura extends two rib spaces below the lung margin, forming the costodiaphragmatic recess:
| Reference Line | Pleural Reflection |
|---|---|
| Midclavicular line | Rib VIII |
| Midaxillary line | Rib X |
| Posterior | Vertebra TXII (T12) |
The gap between the lung inferior border and the pleural reflection is the costodiaphragmatic recess - where pleural fluid accumulates first.
6. Fissures and Lobes
Oblique Fissure - Both Lungs
Present in both lungs, separating the upper/superior lobe from the lower/inferior lobe (and also from the middle lobe on the right):
- Posteriorly: Begins at the spinous process of T4 (TIV) in the midline
- Laterally: Descends, crossing the 4th and 5th intercostal spaces, reaching rib V at the midaxillary line
- Anteriorly: Follows the contour of rib VI and its costal cartilage
The left oblique fissure starts slightly higher - between the spinous processes of TIII and TIV - and is slightly more oblique than the right.
Bedside tip: With arms raised (hands behind head), the medial border of the scapula parallels the oblique fissure - useful for estimating its position.
Horizontal Fissure - Right Lung Only
Separates the upper (superior) lobe from the middle lobe of the right lung:
- Anteriorly: Follows the 4th intercostal space from the sternum to the midaxillary line
- Laterally: Crosses rib V at the midaxillary line, where it meets the oblique fissure
- In the anterior view, follows the contour of rib IV and its costal cartilage
Anterior and Posterior Views
Fig. 3.114 - (A) Anterior view: right side shows superior, middle, and inferior lobes separated by horizontal fissure (rib VI) and oblique fissure; left side shows superior and inferior lobes. (B) Posterior view: oblique fissure at TIV, lower margin at TX, pleural reflection at TXII.
Posterior and Lateral Views
Fig. 3.115 - (A) Posterior view with arms abducted: medial border of the scapula parallels the oblique fissure. (B) Lateral view: oblique fissure starts at TIV spine, crosses ribs IV-V, ends at rib VI anteriorly; horizontal fissure crosses rib V at midaxillary line and follows rib IV to the sternum.
Quick Reference Summary Table
| Landmark | Right Lung | Left Lung |
|---|---|---|
| Apex | 2.5 cm above medial clavicle | 2.5 cm above medial clavicle |
| Anterior border deviation | None - runs straight to 6th CC | Deviates laterally at 4th CC (cardiac notch) |
| Inferior border (MCL) | Rib VI | Rib VI |
| Inferior border (MAL) | Rib VIII | Rib VIII |
| Inferior border (posterior) | T10 | T10 |
| Pleural reflection (MCL) | Rib VIII | Rib VIII |
| Pleural reflection (MAL) | Rib X | Rib X |
| Pleural reflection (posterior) | T12 | T12 |
| Oblique fissure (starts) | T4 spine | T3-T4 spine |
| Oblique fissure (lateral) | Rib V at MAL | Rib V at MAL |
| Oblique fissure (ends) | Rib VI anteriorly | Rib VI anteriorly |
| Horizontal fissure (anterior) | 4th ICS / rib IV | Absent |
| Horizontal fissure (lateral) | Rib V at MAL | Absent |
| Lobes | 3 (upper, middle, lower) | 2 (upper, lower) |
Clinical Relevance
- Auscultation: The posterior chest wall overlies mainly the lower lobes of both lungs. The upper lobes are best heard anteriorly and at the apices. The right middle lobe is best heard at the right lower anterior chest and right axilla.
- Pleural effusion: Fluid collects first in the costodiaphragmatic recess. Dullness to percussion below the lung margin (between rib VI and rib VIII at MCL) suggests an effusion.
- Pleural tap (thoracocentesis): Performed above the rib margin between the lung's inferior border and the pleural reflection (typically around the 8th-9th rib space at the posterior chest wall) to avoid the lung and neurovascular bundle.
- Pneumothorax: Air rises to the apex; absent breath sounds and hyper-resonance over the upper chest anteriorly.
- Gray's Anatomy for Students, pp. 205-207, 243-245, 277-279
This is a shared conversation. Sign in to Orris to start your own chat.