Teach Tfcc repair with diagram
Reading File
Finding Sources
Finding Sources
Generating Image
Medical diagram showing TFCC (Triangular Fibrocartilage Complex) anatomy and repair. Label all key structures: triangular fibrocartilage disc, dorsal radioulnar ligament, volar radioulnar ligament, ulnocarpal ligaments (ulnolunate and ulnotriquetral), meniscus homologue, extensor carpi ulnaris tendon sheath, distal radioulnar joint (DRUJ), lunate, triquetrum, ulnar styloid, sigmoid notch of radius. Show both intact anatomy and the arthroscopic repair technique with sutures. Include cross-section view. Clean educational style with color-coded structures and clear labels.
Searching the Web
TFCC repair surgical technique arthroscopic outside-in inside-out 2024
Reading File
Reading File
I now have excellent content from Campbell's for a complete teaching answer. Here is the full comprehensive lesson on TFCC repair:
TFCC Repair - Complete Teaching Guide
The Diagram
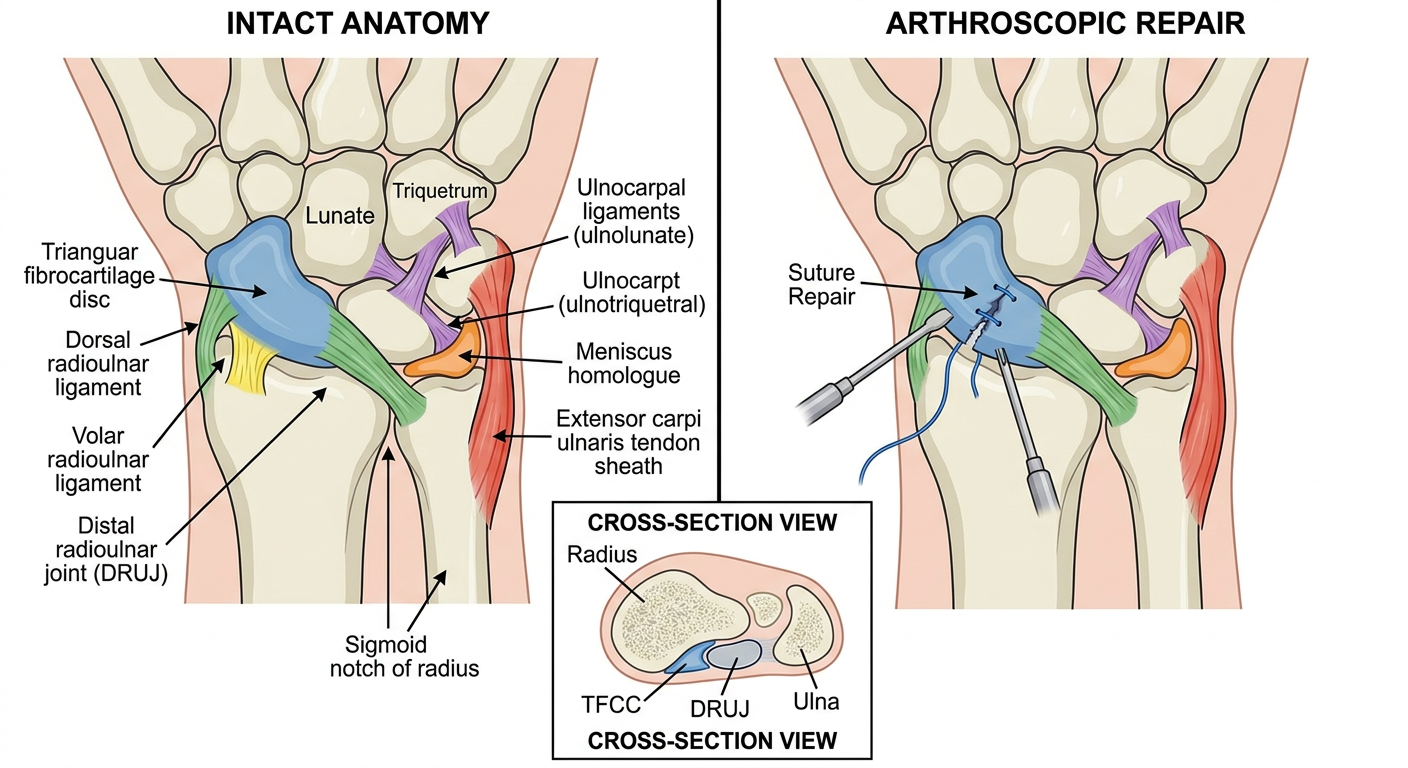
1. Anatomy of the TFCC
The Triangular Fibrocartilage Complex (TFCC) is the primary stabilizer of the distal radioulnar joint (DRUJ) and the ulnocarpal joint. It consists of:
| Component | Function |
|---|---|
| Articular disc (TFC disc) | Central fibrocartilage; load transmission from carpus to ulna |
| Dorsal radioulnar ligament | DRUJ stability in pronation |
| Volar (palmar) radioulnar ligament | DRUJ stability in supination |
| Ulnolunate ligament | Ulnocarpal stability |
| Ulnotriquetral ligament | Ulnocarpal stability |
| Meniscus homologue | Fills the prestyloid recess |
| ECU tendon sheath floor | Forms the ulnar border |
Vascularity note: The peripheral 15-20% of the TFCC has a good blood supply (from the ulnar artery and dorsal/palmar radiocarpal branches) and is therefore repairable. The central 80% is avascular and is only debrideable, not repairable.
2. Palmer Classification (Essential for Choosing Treatment)
CLASS 1 - TRAUMATIC
1A Central disc perforation
1B Peripheral (ulnar) detachment ← Most common repairable tear
1C Distal detachment (ulnocarpal ligament avulsion)
1D Radial-sided detachment (from sigmoid notch)
CLASS 2 - DEGENERATIVE (Ulnocarpal Abutment)
2A → 2E Progressive degeneration
Atzei Classification refines Type 1B further:
- Atzei 1-2: Superficial/partial peripheral tear - arthroscopic repair
- Atzei 3: Deep foveal tear - foveal reattachment (suture anchor or bone tunnel)
- Atzei 4-5: Irreparable - reconstruction
3. Indications for Repair
- Palmer 1B (peripheral ulnar tears) - primary indication
- Palmer 1D (radial-sided/sigmoid notch tears)
- Failed 3-6 months of conservative treatment (splinting, corticosteroid injection)
- DRUJ instability on clinical exam
- Positive "trampoline test" and "hook test" at arthroscopy
4. Pre-operative Assessment
Clinical tests:
- Fovea sign: Tenderness in the soft spot between ulnar styloid and FCU tendon
- DRUJ stress test: Anteroposterior translation with wrist in neutral, pronation, supination
- Press test: Patient presses on chair arm; reproduces ulnar wrist pain
- Piano key sign: Prominent ulnar head displaces dorsally, reduces with pressure
Imaging:
- MRI arthrogram - gold standard (80-90% sensitivity for peripheral tears)
- Plain X-ray: ulnar variance measurement
5. Arthroscopic Anatomy - Portal Placement
DORSAL PORTALS (most commonly used):
3-4 portal ← Standard viewing portal (between EPL and EDC)
4-5 portal ← Alternative viewing/working
6R portal ← Main working portal (radial to ECU)
6U portal ← Working portal (ulnar to ECU)
DRUJ portal ← Direct DRUJ inspection (1 cm proximal to 6R)
6. Surgical Techniques
Technique A: Arthroscopic Outside-In Repair (Palmer 1B, Atzei 1-2)
Step-by-step (Campbell's Technique 74.25, modified):
-
Setup: Patient supine, arm on hand table, traction tower with 10-15 lbs finger-trap traction. Arthroscope in 3-4 portal.
-
Diagnosis confirmation: Use probe via 6R portal.
- Trampoline test: Normal TFCC has firm rebound; torn TFCC is lax
- Hook test: Hook probe under TFCC edge; tears allow >1 cm displacement
-
Synovectomy: Insert full-radius shaver via 6R portal; debride to allow visualization.
-
Tear identification: Locate peripheral avulsion from ulnar capsule/fovea.
-
Bed preparation: Lightly abrade the ulnar capsule to promote healing response.
-
Suture passage (outside-in):
- Place 18-gauge spinal needles percutaneously from ulnar side through capsule and TFCC
- Pass PDS or 2-0 FiberStick suture through each needle
- Retrieve sutures arthroscopically via 6R portal
- Tie sutures together to form a horizontal mattress configuration
-
Knot tying: Tie knots over ulnar capsule through a small (1-2 cm) dorsal-ulnar incision (between ECU and FCU), protecting dorsal sensory branch of ulnar nerve.
-
DRUJ check: Confirm stability with anteroposterior stress under arthroscopic vision.
Technique B: Arthroscopic Repair of Class 1D (Sigmoid Notch Avulsion)
(Campbell's Technique 74.27 - Sagerman, Short, Trumble, Jantea)
-
Arthroscope in 3-4 portal; probe in 6R portal to confirm tear from sigmoid notch margin.
-
Via 6R portal, debride the distal rim of the sigmoid notch down to bleeding bone (motorized burr or shaver) - this is critical for healing.
-
Probe TFCC to determine best suture placement locations.
-
Drill suture holes:
- Make small incision between ECU and flexor carpi ulnaris
- Use 0.045-inch K-wire or drill to create 2-3 transosseous bone tunnels through the radial sigmoid notch
- Holes spaced 3-4 mm apart
-
Pass sutures: Thread 2-0 PDS or non-absorbable suture through bone tunnels and through TFCC substance using suture needle/lasso.
-
Tie sutures with TFCC reduced firmly to the radius sigmoid notch.
-
Confirm DRUJ stability.
Technique C: Open Repair (Class 1D, retracted tears, failed arthroscopy)
(Campbell's Figure 74.62 technique)
-
Approach: Longitudinal dorsal incision over DRUJ; develop between EDC and EDQ tendons.
-
Reflect: Elevate dorsal radioulnar ligament and periosteum over lunate fossa.
-
Expose TFCC: Identify the radial avulsion site.
-
Prepare bed: Decorticate sigmoid notch edge with curette.
-
Repair options:
- Transosseous sutures: Drill 2 bone tunnels through radius; pass sutures through TFCC and tie over bone bridge
- Suture anchors: Place anchors in radial sigmoid notch; tie down TFCC
-
Close: Repair extensor retinaculum; skin closure.
Technique D: Foveal Reattachment (Atzei 3 - Deep tears, DRUJ instability)
Newer "over-the-top" (OTT) technique (Mayo Clinic, 2025):
- Arthroscope placed in DRUJ directly for visualization.
- Foveal footprint debrided to bleeding bone.
- Sutures placed over the top through TFCC and into bone (avoids tunnel drilling in ulna, reducing fracture risk).
- Faster, less radiation exposure than traditional bone-tunnel techniques.
7. Postoperative Care
| Phase | Time | Protocol |
|---|---|---|
| Immobilization | 0-6 weeks | Above-elbow cast, forearm in neutral rotation |
| Early mobilization | 6-8 weeks | Below-elbow splint; begin gentle ROM |
| Strengthening | 8-12 weeks | Progressive grip and forearm rotation exercises |
| Return to activity | 3-6 months | Full activity, contact sports |
8. Outcomes
- Arthroscopic repair of Palmer 1B tears: 85-90% good/excellent results at 2-year follow-up
- DRUJ stability restored in >90% of peripheral repairs
- Smaller pronator quadratus cross-sectional area on pre-op MRI is an independent predictor of poorer outcomes
- Knotless suture-lasso techniques reduce knot irritation complications vs. classic outside-in (0% vs. 28.6% knot prominence, per 2023 JOSR study)
9. Key Pitfalls to Avoid
- Protect the dorsal sensory branch of the ulnar nerve during all ulnar-side incisions (runs between ECU and FCU)
- Do not debride more than 2/3 of central disc - preserves peripheral rim and DRUJ stability
- Check ulnar variance pre-op - ulnar-positive patients may need simultaneous ulnar shortening osteotomy
- If TFCC is retracted >5 mm, primary repair may fail - consider extensor retinaculum reconstruction
- Always test DRUJ stability at end of procedure before closing
Campbell's Operative Orthopaedics 15th Ed 2026, Techniques 74.23, 74.25, 74.27 and Figure 74.62
This is a shared conversation. Sign in to Orris to start your own chat.