Explain angina in detail
Reading File
Finding Sources
Finding Sources
Searching PubMed
"angina pectoris"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Searching Images
angina pectoris coronary artery disease ischemia diagram
I now have comprehensive data from multiple authoritative textbooks. Let me compile a thorough, well-organized response.
Angina Pectoris — A Detailed Overview
Definition
Angina pectoris is intermittent chest discomfort or pain caused by transient, reversible myocardial ischemia that is insufficient to cause myocyte necrosis. The term derives from the Latin for "strangling of the chest." It results from an imbalance between myocardial oxygen supply and demand — when demand exceeds what stenotic or spastic coronary arteries can deliver, the myocardium becomes ischemic and releases adenosine, bradykinin, and other pain-mediating molecules that stimulate cardiac autonomic afferents.
(Robbins & Kumar Basic Pathology; Goldman-Cecil Medicine)
Epidemiology
- Nearly 10 million Americans have angina pectoris; coronary heart disease affects over 17 million adults
- Males constitute ~70% of patients with angina; those under age 50 are predominantly male
- Among adults aged 60–79, ~25% of men and 16% of women have coronary heart disease; over age 80, these figures rise to 37% and 23%
- Women tend to be protected during reproductive years; after menopause, risk rises sharply with declining estrogen
- Coronary atherosclerosis can begin before age 20 and may remain silent for decades
(Goldman-Cecil Medicine; Harrison's 22E)
Pathophysiology
Supply–Demand Mismatch
Two major mechanisms cause ischemia:
| Mechanism | Cause | Example |
|---|---|---|
| Demand angina | Increased O₂ requirements | Exercise, emotion, fever, thyrotoxicosis, anemia, tachycardia |
| Supply angina | Reduced O₂ delivery | Coronary stenosis, vasospasm, microvascular dysfunction, thrombosis |
In stable atherosclerotic disease, the fixed plaque limits maximal coronary flow. At rest, flow may be adequate, but any increase in demand (e.g., exercise increasing heart rate, blood pressure, and contractility → raised LV wall tension) cannot be met → ischemia → pain.
Underlying Causes
- Obstructive epicardial coronary artery disease (CAD) — most common; atherosclerotic plaque narrows the vessel lumen
- Vasospasm — dynamic constriction of an epicardial artery (Prinzmetal angina), can affect normal vessels
- Microvascular dysfunction — abnormal resistance in small intramyocardial arterioles (especially common in women); normal epicardial arteries on angiography
- Nonvascular causes — derangements in myocardial energy supply, abnormal blood rheology, extravascular microcirculatory compression, amyloid deposition, vasculitis, sickle cell disease
Pain Generation
Ischemia triggers release of adenosine, bradykinin, and substance P → stimulate cardiac sympathetic afferents C4–T12 → referred pain to chest, arm, jaw, teeth, epigastrium.
Types of Angina
1. Stable (Typical) Angina
- Predictable, episodic chest discomfort reproducibly triggered by a fixed level of exertion or emotion
- Relieved by rest (reducing demand) or nitroglycerin (vasodilation)
- Underlying substrate: fixed atherosclerotic stenosis
- CCS Class I–II on the grading scale
2. Unstable Angina
- Increasingly frequent pain precipitated by progressively less exertion, or occurring at rest
- Signifies plaque disruption + superimposed thrombosis, distal embolization, and/or vasospasm
- Most cases show evidence of myocyte injury (troponin elevation) → aggressive management required
- CCS Class III–IV
3. Prinzmetal (Variant) Angina
- Occurs at rest, caused by coronary artery vasospasm
- Can affect both atherosclerotic and completely healthy vessels
- Responds promptly to vasodilators (nitroglycerin, calcium channel blockers)
- Beta-blockers are contraindicated in pure vasospasm without fixed stenosis
4. Microvascular Angina (Cardiac Syndrome X)
- Angina + ischemic ECG changes with normal epicardial coronaries on angiography
- Due to small-vessel (microvascular) dysfunction
- More common in women post-menopause
- Managed with beta-blockers, ACE inhibitors, and statins
Canadian Cardiovascular Society (CCS) Grading Scale
| Class | Description |
|---|---|
| I | Angina only with strenuous/prolonged physical activity; ordinary activity does not cause angina |
| II | Slight limitation of ordinary activity; angina with walking >2 blocks on level or climbing >1 flight of stairs |
| III | Marked limitation; angina with walking 1–2 blocks on level or climbing 1 flight of stairs |
| IV | Inability to perform any activity without angina, or angina at rest |
(Goldman-Cecil Medicine)
Clinical Features
Typical Presentation
- Location: Substernal, central — patient often places a clenched fist over sternum (Levine's sign)
- Character: Heaviness, pressure, squeezing, smothering, choking — rarely described as "sharp" or "stabbing"
- Radiation: Left shoulder, both arms (especially ulnar forearm/hand), jaw, teeth, neck, interscapular region, epigastrium
- Duration: Typically 2–5 minutes; crescendo-decrescendo in character
- Triggers: Exertion, hurrying, sexual activity, cold weather, emotional stress, large meals, tachycardia
- Relief: Rest, nitroglycerin (within minutes)
Important Negatives
- Angina is rarely below the umbilicus or above the mandible
- Does NOT radiate to the trapezius (pericarditis does)
- Not positional or reproducibly triggered by palpation (musculoskeletal pain)
Nocturnal Angina (Angina Decubitus)
May be due to episodic tachycardia during sleep, reduced oxygenation from changing respiratory patterns, or expansion of intrathoracic blood volume causing increased preload.
Women and Atypical Presentations
Women more commonly present with atypical features — fatigue, dyspnea, nausea, epigastric discomfort — without classic chest pressure. Microvascular angina is disproportionately common in women.
(Harrison's Principles of Internal Medicine 22E)
Diagnosis
History & Physical Exam
- History is paramount; typical features have high diagnostic value
- Physical exam often normal; may show signs of heart failure, hypertension, or atherosclerosis elsewhere
Investigations
| Test | Role |
|---|---|
| ECG (resting) | May be normal; ST depression or T-wave changes during pain |
| Exercise stress test (EST) | Provokes ischemia; ST depression ≥1 mm = positive; determines functional capacity in METs |
| Echocardiography | LV function, wall motion abnormalities |
| Coronary CT Angiography (CTA) | Non-invasive; rules out obstructive CAD; also assesses plaque burden and calcification |
| Coronary Artery Calcium (CAC) score | Adjunctive risk stratification; NOT primary screening or isolated basis for treatment decisions |
| Stress imaging (nuclear/echo/CMR) | Detects reversible ischemia; guides revascularization |
| Invasive coronary angiography | Gold standard; quantifies stenosis; guides PCI or CABG |
| Cardiac biomarkers | Troponin elevation distinguishes NSTEMI from unstable angina |
Differential Diagnosis
- Esophageal spasm (non-exertional, meal-related, relieved by antacids)
- Aortic dissection
- Pulmonary embolism
- Pericarditis (positional, trapezius radiation, friction rub)
- Musculoskeletal pain (reproducible by palpation)
- GERD / peptic ulcer
Management
1. Risk Factor Modification
- Smoking cessation — accelerates atherosclerosis, increases thrombosis risk, aggravates angina by both raising demand and reducing supply
- Lipid control — statins reduce plaque burden and stabilize plaques
- Hypertension control — reduces cardiac workload
- Diabetes management
- Weight loss and regular isotonic exercise — up to 80% of the heart rate associated with ischemia on stress testing
- Diet — low saturated and trans-unsaturated fats, reduced calories for optimal body weight
2. Anti-Ischemic Pharmacotherapy
Nitrates
- Mechanism: Converted to nitric oxide (NO) → increases cGMP → relaxes vascular smooth muscle → venodilation reduces preload; arterial dilation reduces afterload and increases coronary perfusion
- Also have antithrombotic activity via NO-dependent platelet guanylyl cyclase activation
- Sublingual nitroglycerin (0.4–0.6 mg): acute relief; absorbed rapidly via mucous membranes; take 5 min before precipitating activities
- Long-acting nitrates: prevent attacks; a nitrate-free interval of 8–10 hours/day is required to prevent tolerance
- Effective in stable angina, unstable angina, and vasospastic (Prinzmetal) angina
Beta-Blockers (First-Line for Stable Angina)
- Mechanism: Block sympathetic stimulation → reduce heart rate, blood pressure, and contractility → decrease myocardial O₂ demand
- Especially effective for exertional angina
- Contraindicated in pure vasospastic angina (can worsen spasm)
- Examples: metoprolol, atenolol, bisoprolol, carvedilol
Calcium Channel Blockers (CCBs)
| Class | Examples | Key Notes |
|---|---|---|
| Dihydropyridines | Amlodipine, nifedipine, felodipine | Vasodilation (arterial), less cardiac depression |
| Non-dihydropyridines | Diltiazem, verapamil | Reduce HR and contractility; more cardiac suppression |
- Drug of choice for Prinzmetal angina (vasospasm)
- Alternative when beta-blockers are contraindicated or ineffective
- Nifedipine immediate-release associated with increased mortality risk in acute MI
Ranolazine
- Inhibits late sodium current → reduces intracellular calcium overload → antianginal without significant hemodynamic effects
- Useful add-on when other agents are insufficient
3. Antiplatelet and Anticoagulant Therapy
- Aspirin (75–100 mg/day): mandatory in all patients without contraindications
- P2Y12 inhibitors (clopidogrel, ticagrelor): used in ACS/post-stenting
- Heparin/LMWH: used in unstable angina/NSTEMI
4. Revascularization
| Procedure | Indication |
|---|---|
| PCI (stenting) | Single/double vessel disease, symptoms refractory to medical therapy |
| CABG | Triple-vessel disease, left main stenosis, reduced LVEF, diabetes with multivessel disease |
Revascularization improves symptoms and quality of life; in specific high-risk groups, it reduces mortality. Medical therapy alone remains appropriate for many stable angina patients.
(Harrison's 22E; Goldman-Cecil Medicine; Katzung's Pharmacology)
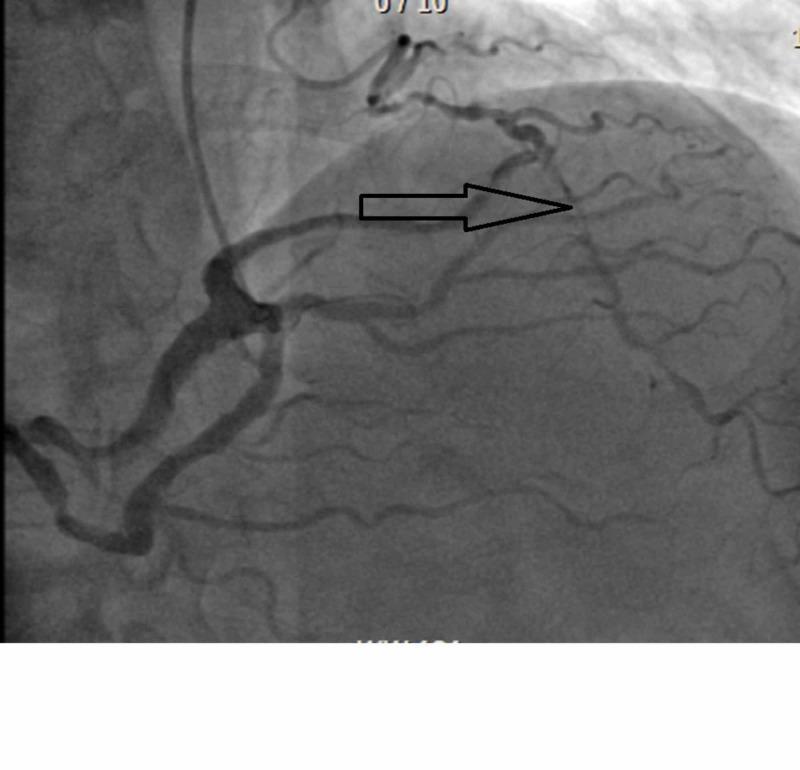
Illustrative Images
Coronary artery stenosis on angiography — the classic substrate for angina:
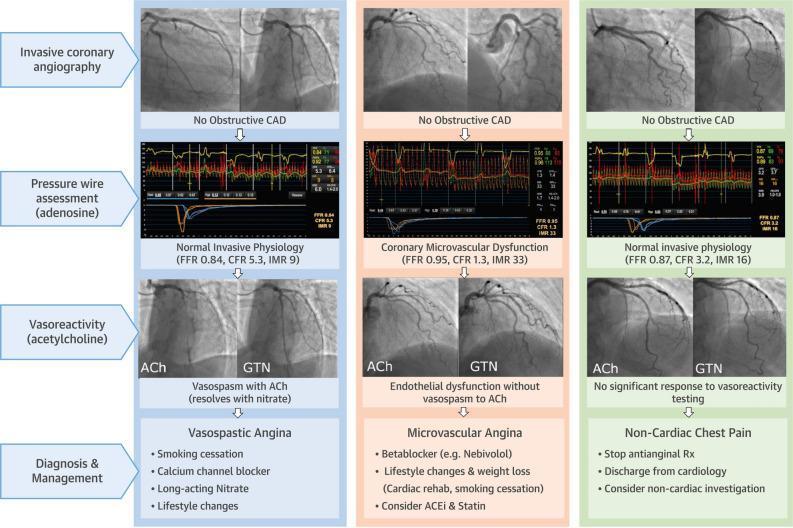
INOCA diagnostic pathway — vasospastic vs. microvascular angina vs. non-cardiac chest pain:
Summary Table
| Feature | Stable Angina | Unstable Angina | Prinzmetal Angina |
|---|---|---|---|
| Trigger | Exertion/emotion | Rest or minimal exertion | Rest (often nocturnal) |
| Cause | Fixed atherosclerotic stenosis | Plaque rupture + thrombosis | Coronary artery vasospasm |
| ECG during episode | ST depression | ST depression / T changes | ST elevation (transient) |
| Troponin | Negative | Often mildly positive | Usually negative |
| Response to nitrates | Yes | Yes | Yes (excellent) |
| Beta-blockers | First-line | Used (with caution) | Avoid (can worsen spasm) |
| CCBs | Useful | Useful | Drug of choice |
Key sources: Robbins & Kumar Basic Pathology; Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine; Katzung's Basic and Clinical Pharmacology 16E
This is a shared conversation. Sign in to Orris to start your own chat.