Hydrocephalus
"hydrocephalus"[MeSH Terms]
Hydrocephalus
CSF Physiology - The Foundation
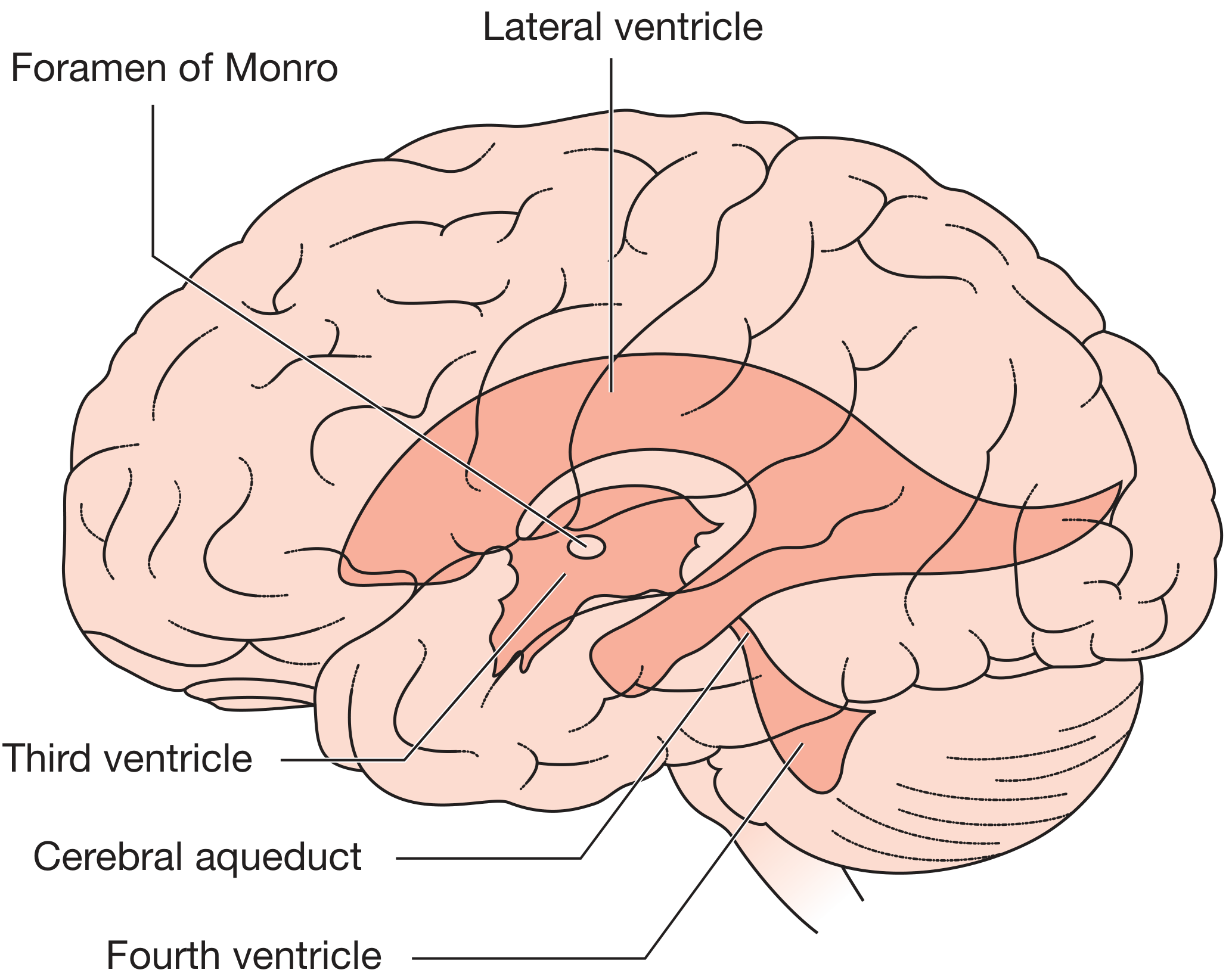
Classification
1. Non-communicating (Obstructive) Hydrocephalus
- The blockage is within the ventricular system itself.
- CSF cannot flow from the ventricles to the subarachnoid space.
- Only the ventricles proximal to the obstruction enlarge.
- Common sites: cerebral aqueduct, foramen of Monro, fourth ventricle outflow.
- Causes: aqueductal stenosis/gliosis, tumors, hemorrhage, Chiari II malformation, colloid cyst of the 3rd ventricle.
2. Communicating (Extra-ventricular Obstructive) Hydrocephalus
- The obstruction is outside the ventricular system - in the subarachnoid space or at the arachnoid granulations.
- The entire ventricular system enlarges.
- Causes: subarachnoid hemorrhage (post-SAH scarring), meningitis (bacterial, TB, fungal, syphilis), leptomeningeal carcinomatosis, choroid plexus papilloma (rarely - CSF overproduction).
3. Hydrocephalus Ex Vacuo
-
Compensatory increase in CSF volume secondary to loss of brain parenchyma (infarction, neurodegenerative disease).
-
Not a true hydrocephalus - no elevation of ICP.
-
Does not benefit from shunting.
-
Robbins & Kumar Basic Pathology, p. 821
Causes by Age Group
Neonates and Infants (pre-suture closure, < 2 years)
- Congenital aqueductal stenosis/gliosis (most common - often post in utero infection)
- Post-hemorrhagic hydrocephalus - intraventricular hemorrhage (IVH) in premature infants < 1500g; ~25% develop progressive ventricular enlargement; 5% ultimately require shunting.
- Chiari II malformation - associated with lumbosacral myelomeningocele; fourth ventricular outlet foramina displaced below the foramen magnum.
- Dandy-Walker malformation - cystic dilatation of the fourth ventricle.
- Post-infective - meningitis causing scarring and closure of the cerebral aqueduct or foramina of Magendie/Luschka.
- Vein of Galen malformation (raised intracranial venous pressure).
Older Children (post-suture closure)
- Posterior fossa neoplasms (most common) - compress the cerebral aqueduct/fourth ventricle.
- Aqueductal stenosis (developmental or acquired).
- Meningitis.
Adults
-
Acute: Cerebellar hemorrhage or infarction compressing the aqueduct; subarachnoid hemorrhage; colloid cyst of third ventricle (ball-valve mechanism causing intermittent symptoms), intraventricular ependymoma, cysticercosis (racemose form).
-
Chronic/communicating: Post-SAH, post-meningitis, leptomeningeal disease, idiopathic.
-
Normal Pressure Hydrocephalus (NPH): Idiopathic (or secondary to prior SAH/trauma/meningitis).
-
Bradley and Daroff's Neurology, pp. 1854-1856; Grainger & Allison's Diagnostic Radiology
Clinical Features
Infants (sutures still open)
| Feature | Detail |
|---|---|
| Progressive macrocephaly | Most reliable sign; head circumference crossing centile lines |
| Frontal bossing | Prominent forehead |
| Bulging anterior fontanelle | Present even at rest (tense) |
| Sutural diastasis | Separation of skull sutures |
| Enlarged scalp veins | From venous obstruction |
| "Setting-sun" sign | Downward deviation of eyes (Parinaud syndrome); failure of upward gaze |
| Lateral rectus palsy | 6th nerve "false localizing" sign |
| Leg spasticity | Stretching of corticospinal tracts around enlarged ventricles |
| McEwen sign | "Cracked-pot" sound on skull percussion |
| Irritability, poor feeding, lethargy | Non-specific but common |
Older Children and Adults (fused sutures)
- Headache - classically early morning, made worse by lying flat/coughing (increased ICP)
- Nausea and vomiting - early morning vomiting is characteristic
- Papilloedema - on fundoscopy
- Diplopia - 6th nerve palsy (false localizing sign)
- Altered consciousness - drowsiness, confusion, coma with severe cases
- Gait disturbance - wide-based, ataxic
- Sudden death may occur with severe acute ICP elevation
Normal Pressure Hydrocephalus (NPH)
- Gait apraxia - "magnetic gait," wide-based, shuffling (earliest and most prominent)
- Dementia/cognitive impairment - subacute onset
- Urinary incontinence
- Bradley and Daroff's Neurology, pp. 1855-1857
Pathophysiology of Acute Hydrocephalus
- 80% of maximal ventricular enlargement occurs within the first 6 hours (continued CSF production despite elevated pressure).
- A slower phase of enlargement follows.
- Fluid accumulates in periventricular white matter → interstitial (transependymal) edema.
- As it becomes chronic, CSF pressure may normalize ("normal pressure" phase), but long-term ICP monitoring still shows intermittent elevations.
- Long-standing hydrocephalus causes white matter atrophy, periventricular demyelination.
Imaging
CT / MRI Findings - Active (Obstructive) Hydrocephalus
- Temporal horn dilatation disproportionate to overall lateral ventricular enlargement (most sensitive early sign)
- Inferior convexity of the third ventricular floor and enlargement of its anterior and posterior recesses
- Transependymal (periventricular interstitial) edema - periventricular hypodensity on CT, T2/FLAIR hyperintensity on MRI
- Sulcal effacement - sulci, major fissures, and basal cisterns are small or obliterated (distinguishes true hydrocephalus from ex vacuo)
- Bulging of fontanelles in infants
Differentiating Hydrocephalus from Ex Vacuo
| Feature | True Hydrocephalus | Ex Vacuo |
|---|---|---|
| Sulci/fissures | Effaced, small | Widened, prominent |
| Basal cisterns | Small | Normal or large |
| ICP | Elevated | Normal |
| Transependymal edema | Present | Absent |
| Head circumference | May increase (infants) | Normal |
Aqueductal Stenosis on MRI
-
Focal narrowing at the superior colliculi or intercollicular sulcus on sagittal MRI.
-
Lateral and third ventricles dilated; fourth ventricle normal size.
-
Grainger & Allison's Diagnostic Radiology, pp. 2028-2029
Treatment
Underlying Cause
CSF Diversion
| Procedure | Description |
|---|---|
| Ventriculoperitoneal (VP) shunt | Gold standard; one-way pressure-sensitive valve; CSF drained into peritoneal cavity |
| Ventriculoatrial (VA) shunt | Drain into right atrium; used when peritoneal cavity is unsuitable |
| Endoscopic Third Ventriculostomy (ETV) | Surgical fenestration of the third ventricle floor; CSF drains into suprasellar cistern; preferred in aqueductal stenosis and children > 6 months; avoids a foreign body |
| External Ventricular Drain (EVD) | Temporary; used in acute hydrocephalus (e.g., post-SAH, cerebellar hemorrhage) to emergently decompress and monitor ICP |
Shunt Complications
- Shunt obstruction (most common) - choroid plexus or glial tissue blocks the catheter; presents with recurrence of hydrocephalus symptoms.
- Shunt infection - presents with fever, meningism; requires shunt removal + antibiotics.
- Shunt overdrainage - subdural hygroma/hematoma; slit-ventricle syndrome.
- Shunt disconnection - detectable on plain skull-to-abdomen X-ray; calcification may be seen at fracture ends.
- Revisions are frequently required in children as they grow.
NPH - Shunting
Special Situations
Post-SAH Hydrocephalus
Choroid Plexus Papilloma
Raised Intracranial Venous Pressure
Occult Spinal Lesions
Summary Table
| Feature | Non-communicating | Communicating | NPH |
|---|---|---|---|
| Obstruction site | Within ventricles | Subarachnoid space | Arachnoid granulations (impaired absorption) |
| Ventricles affected | Partial (proximal only) | All ventricles | All ventricles |
| Common causes | Aqueductal stenosis, tumors, Chiari II | SAH, meningitis | Idiopathic (elderly) |
| Presentation | Acute ICP features | Subacute ICP features | Hakim triad (gait, dementia, incontinence) |
| Treatment | ETV or VP shunt | Treat cause + VP shunt | VP shunt (if tap test positive) |
Make a diagram showing obstructive vs communicating hydrocephalus pathways
Medical educational diagram comparing obstructive (non-communicating) vs communicating hydrocephalus CSF pathways. Split into two side-by-side panels on a clean white background. LEFT PANEL - "Obstructive (Non-Communicating) Hydrocephalus": - Labeled sagittal brain cross-section showing the ventricular system - Lateral ventricle and third ventricle shown enlarged/dilated (colored in blue, darker shade) - Cerebral aqueduct blocked with a red X or red barrier symbol - Fourth ventricle shown as normal size (lighter blue) - Subarachnoid space shown as normal - Arrow showing CSF flow blocked at aqueduct - Text labels: "Lateral ventricle (DILATED)", "Third ventricle (DILATED)", "Cerebral aqueduct (BLOCKED)", "Fourth ventricle (normal)", "Subarachnoid space (normal)" - Common causes listed below: "Causes: Aqueductal stenosis, Posterior fossa tumor, Colloid cyst, Chiari II malformation" RIGHT PANEL - "Communicating Hydrocephalus": - Labeled sagittal brain cross-section showing the ventricular system - All four ventricles shown enlarged/dilated (all in blue, darker shade) - Cerebral aqueduct shown as patent/open (no blockage) - Subarachnoid space shown as thickened/blocked with red X at the arachnoid granulations along superior sagittal sinus - Arrow showing CSF flows freely through ventricles but is blocked at absorption point - Text labels: "Lateral ventricle (DILATED)", "Third ventricle (DILATED)", "Cerebral aqueduct (PATENT)", "Fourth ventricle (DILATED)", "Arachnoid granulations (IMPAIRED ABSORPTION)" with red X - Common causes listed below: "Causes: Subarachnoid hemorrhage, Meningitis, Leptomeningeal carcinomatosis" Shared CSF pathway legend at the bottom: blue arrows showing normal flow direction from lateral ventricles → foramen of Monro → third ventricle → cerebral aqueduct → fourth ventricle → foramina of Magendie & Luschka → subarachnoid space → arachnoid granulations → superior sagittal sinus Clean medical textbook illustration style, clear anatomical labels, professional and educational
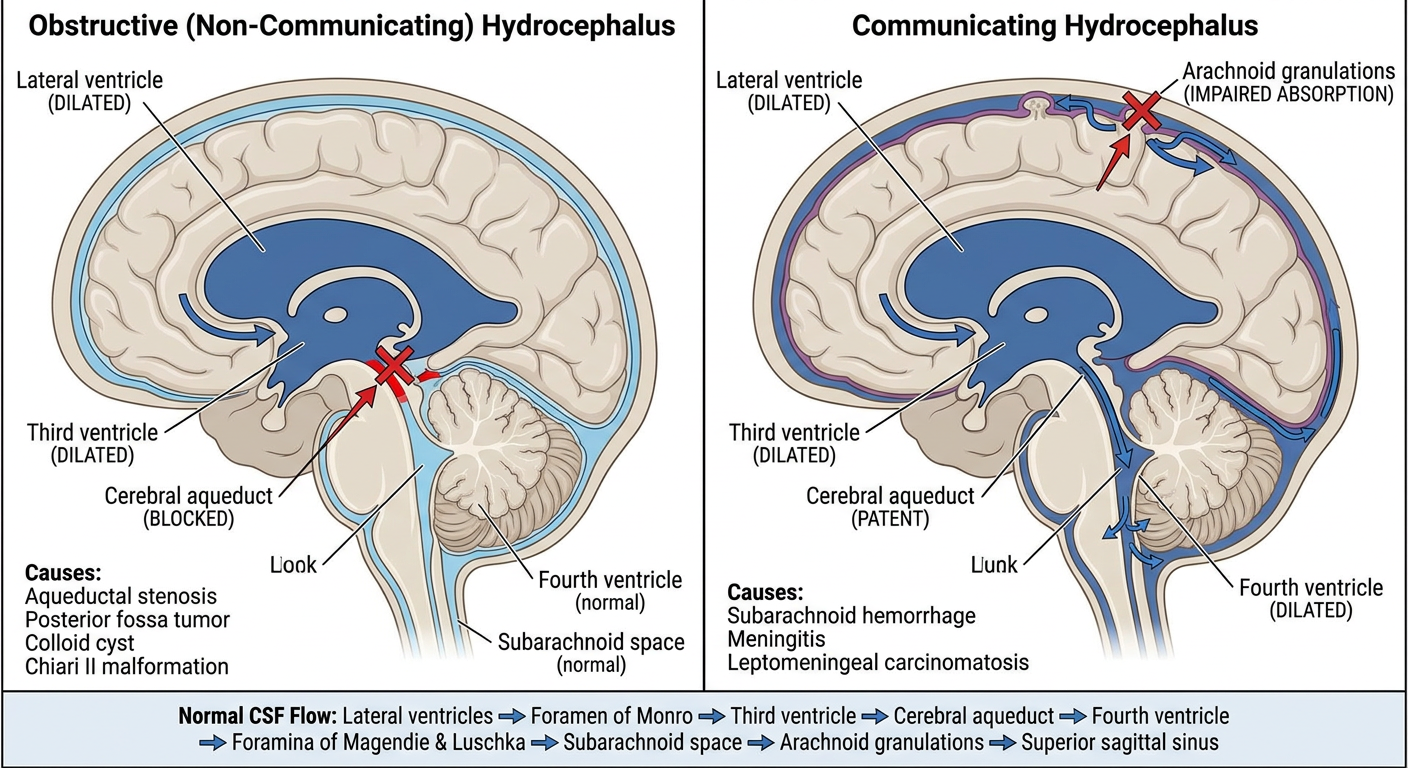
- Only the ventricles proximal to the block are enlarged (lateral + third ventricles)
- Blockage at the cerebral aqueduct (most common site)
- Fourth ventricle and subarachnoid space remain normal
- CSF cannot exit the ventricular system
- All four ventricles are dilated because CSF flows freely through them
- The block is at the level of the arachnoid granulations (impaired absorption)
- Causes like SAH and meningitis leave fibrous scarring in the subarachnoid space, preventing reabsorption into the superior sagittal sinus