Compliance
Asking for Preferences
Lung compliance
Reading File
Finding Sources
Searching the Web
lung compliance physiology definition measurement clinical significance
Searching PubMed
"lung compliance" physiology
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
Lung Compliance
Definition
Lung compliance is the measure of the lung's ability to stretch and expand. It is defined as the change in volume per unit change in pressure:
C = ΔV / ΔP
A high compliance means the lung distends easily; a low compliance means it is stiff and resists expansion. Compliance is the inverse of elastance (recoil):
Elastance = 1 / Compliance
- Costanzo Physiology 7th Edition, p. 205
Normal Values
| Component | Compliance |
|---|---|
| Lung alone | ~150-220 mL/cmH₂O |
| Chest wall alone | ~200 mL/cmH₂O |
| Total respiratory system (lung + chest wall in series) | ~85-130 mL/cmH₂O |
Because the lung and chest wall are arranged in series, total compliance is calculated as:
1/C_RS = 1/C_L + 1/C_W
- Murray & Nadel's Textbook of Respiratory Medicine, p. 207
Static vs. Dynamic Compliance
- Static compliance - measured when there is no airflow; reflects the pure elastic properties of the lung and chest wall. It is measured at points of zero flow (end-inspiration and end-expiration).
- Dynamic compliance - measured during breathing, when air is moving. It is influenced by both elastic properties AND airway resistance. Dynamic compliance will be lower than static compliance when airway resistance is increased (e.g., asthma, COPD).
Pressure-Volume Curve and Hysteresis
The compliance curve of an air-filled lung shows hysteresis - the inspiration and expiration limbs follow different paths:
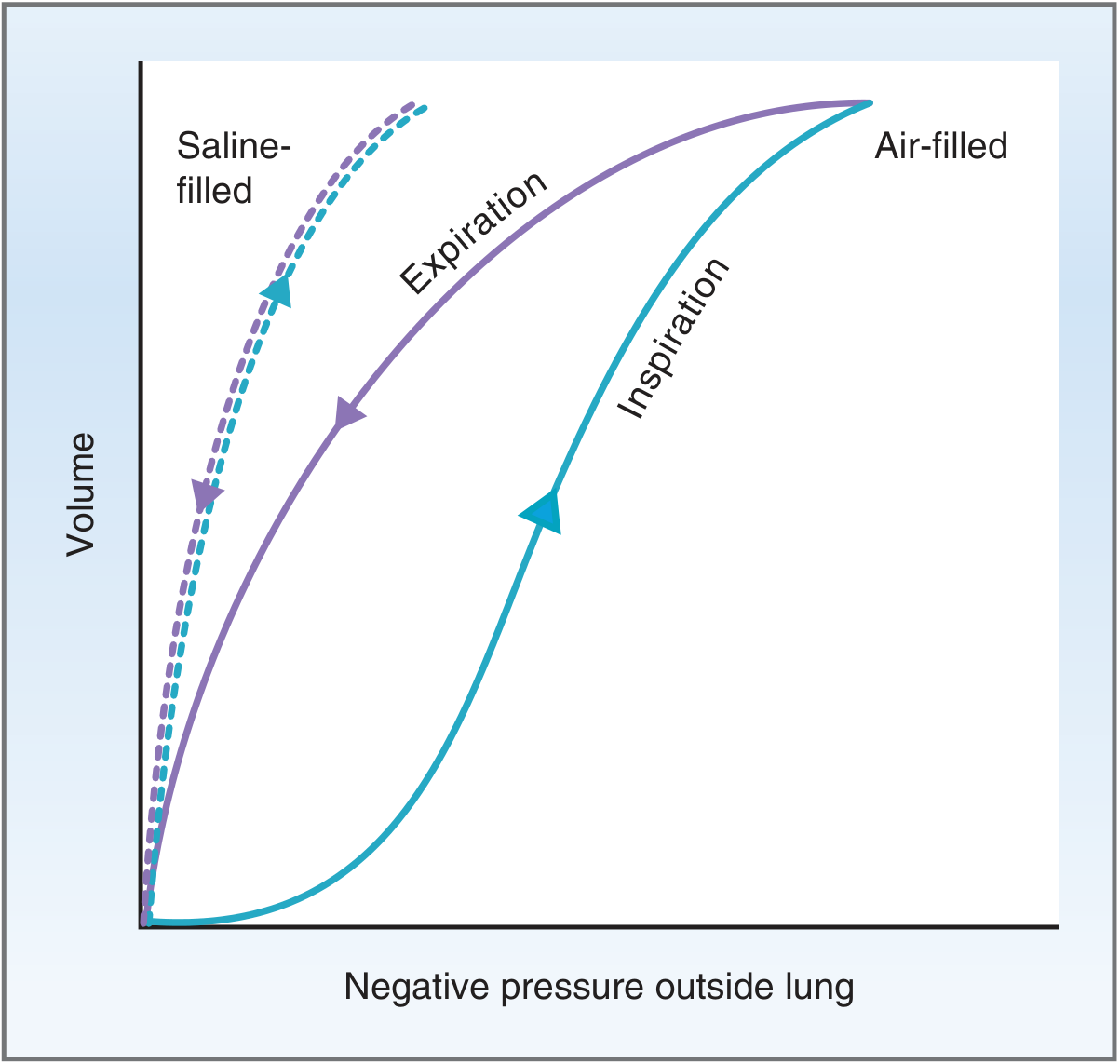
Fig. 5.7 from Costanzo Physiology: Compliance of the lung. The air-filled lung shows different inspiration and expiration curves (hysteresis), while the saline-filled lung does not.
Key observations:
-
For a given pressure, lung volume is greater during expiration than inspiration (expiration limb is steeper = higher compliance)
-
The saline-filled lung has a single, steeper curve (no hysteresis) because saline eliminates the liquid-air surface tension responsible for hysteresis
-
The comparison proves that surface tension, not elastic tissue, is the primary cause of hysteresis
-
Costanzo Physiology 7th Edition, p. 205-206
Surface Tension and the Law of Laplace
Alveoli are lined with a thin fluid film. The liquid molecules attract each other (surface tension), generating a collapsing pressure described by the Law of Laplace:
P = 2T / r
Where:
- P = collapsing pressure on the alveolus
- T = surface tension
- r = radius of the alveolus
This has an important implication: smaller alveoli have higher collapsing pressures. Without a mechanism to counter this, small alveoli would empty into larger ones (alveolar instability). This is where surfactant comes in.
Role of Surfactant
Surfactant is a phospholipid mixture produced by type II alveolar cells. Its key component is dipalmitoylphosphatidylcholine (DPPC).
Surfactant works by:
- Reducing surface tension - DPPC molecules align at the alveolar surface, with hydrophobic ends attracted to each other and hydrophilic ends repelled, breaking up water-water intermolecular forces
- Preventing alveolar collapse - by reducing T in the Laplace equation, small alveoli no longer have dangerously high collapsing pressures
- Increasing lung compliance - lower surface tension = less force needed to expand the lung = easier breathing = reduced work of breathing
Surfactant synthesis begins around gestational week 24 and is reliably present by week 35. Premature infants born before week 24 will lack surfactant entirely.
- Costanzo Physiology 7th Edition, p. 210
Diseases Affecting Lung Compliance
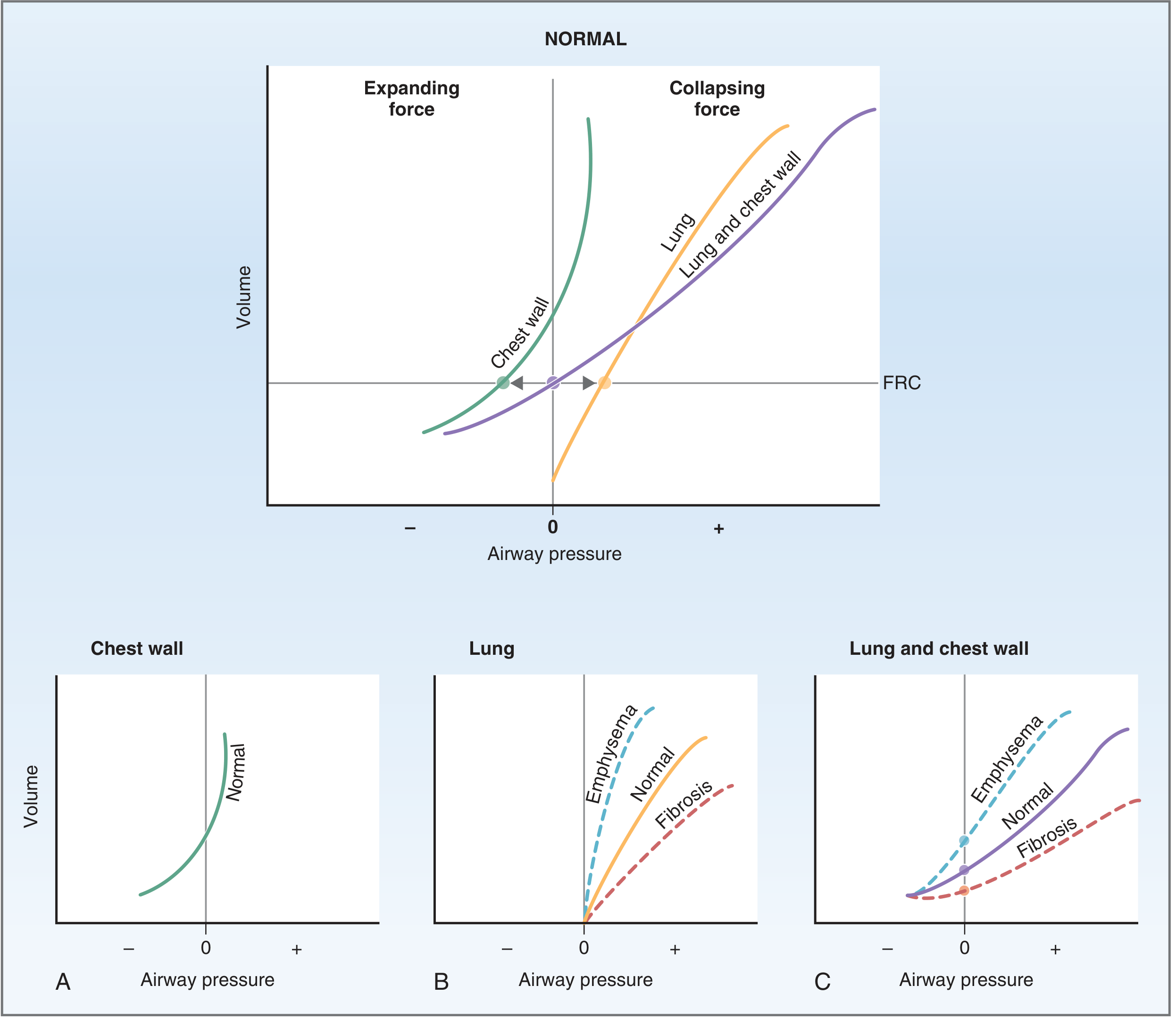
Fig. 5.11 from Costanzo Physiology: Changes in lung compliance and FRC in emphysema (increased compliance) vs. fibrosis (decreased compliance).
Increased Compliance (Floppy Lung)
| Condition | Mechanism | Effect on FRC |
|---|---|---|
| Emphysema | Loss of elastic fibers | Increased FRC ("barrel chest") |
| Aging | Loss of elastic tissue | Mildly increased |
- In emphysema, the lungs' elastic recoil is reduced. At any given volume, the collapsing force of the lung is less than the expanding force of the chest wall. The system reaches a new equilibrium at a higher FRC - the patient breathes at higher lung volumes.
Decreased Compliance (Stiff Lung)
| Condition | Mechanism | Effect on FRC |
|---|---|---|
| Pulmonary fibrosis | Stiffening of lung tissue (fibrotic scarring) | Decreased FRC |
| Neonatal RDS | Surfactant deficiency; atelectasis | Decreased |
| Pulmonary edema | Fluid replaces air; alveolar flooding | Decreased |
| Acute Lung Injury / ARDS | Surfactant dysfunction; inflammation | Decreased |
| Obesity | Reduced FRC; abdominal loading | Decreased |
| Pneumothorax | Loss of transmural pressure | Lungs collapse |
-
In fibrosis, lung stiffness means the collapsing force at the original FRC is now greater than the chest wall's expanding force. The system seeks a new lower FRC - the patient breathes at lower lung volumes.
-
Costanzo Physiology 7th Edition, p. 208
Compliance vs. Age
Lung compliance changes across the lifespan (Miller's Anesthesia, 10th ed.):
- At birth: Low compliance - alveolar precursors have thick walls, decreased elastin, and potentially deficient surfactant
- Childhood to adulthood: Compliance increases as alveolar structure matures
- Old age: Compliance increases again (emphysema-like changes from elastic fiber loss), but dynamic compliance falls due to small airway collapse
Clinical Measurement
In mechanically ventilated patients, static compliance is directly measurable:
- Record end-expiratory pressure (PEEP) and end-inspiratory plateau pressure (P_plat)
- C_static = Tidal Volume / (P_plat - PEEP)
- Normal: ~50-80 mL/cmH₂O on mechanical ventilation
- Falling compliance is an early sign of worsening lung pathology (ARDS, pneumothorax, mucus plugging)
Compliance monitoring guides PEEP titration - a recent meta-analysis (PMID 39825438) confirmed that individualized PEEP titration guided by lung compliance during one-lung ventilation improves oxygenation compared to fixed PEEP strategies.
Summary
| Parameter | Low Compliance | High Compliance |
|---|---|---|
| Lung stiffness | High (stiff) | Low (floppy) |
| Work of breathing | Increased | Decreased (but gas trapping ↑) |
| FRC | Decreased | Increased |
| Examples | Fibrosis, RDS, ARDS, edema | Emphysema, aging |
| Pressure-volume slope | Flat | Steep |
This is a shared conversation. Sign in to Orris to start your own chat.