ADEM
Reading File
search_medical_text
acute disseminated encephalomyelitis ADEM etiology pathophysiology diagnosis clinical features
search_medical_text
ADEM treatment management prognosis MRI findings differential diagnosis
search_medical_image
ADEM acute disseminated encephalomyelitis MRI brain lesions
GradeResponse
GradeResponse
GradeResponse
Acute Disseminated Encephalomyelitis (ADEM)
Overview
ADEM is an immune-mediated inflammatory demyelinating disorder of the CNS characterized by a typically monophasic course with widespread perivenular inflammation and demyelination affecting both white and grey matter (Harrison's, p. 12630).
Etiology & Pathophysiology
| Trigger | Details |
|---|---|
| Postinfectious (~95%) | Most common; follows viral/bacterial illness |
| Postvaccinal (~5%) | Historical association with older rabies, smallpox vaccines; rare with modern vaccines |
| Idiopathic | No identifiable trigger in some cases |
Key pathogens linked to ADEM: measles, rubella, varicella-zoster, EBV, CMV, HSV, Mycoplasma pneumoniae
Pathophysiology: Molecular mimicry is the leading hypothesis — host immune response to an infectious antigen cross-reacts with myelin antigens (e.g., MBP, MOG), triggering perivenular T-cell infiltration and demyelination. MOG-IgG (anti-MOG antibodies) are detected in a significant subset, particularly children.
Epidemiology
- Far more common in children than adults (Harrison's, p. 12630)
- Incidence: ~0.3–0.6 per 100,000/year
- Peak age: 5–8 years
- No clear sex predominance in children; slight male predominance in adults
- Typically follows infection by 1–3 weeks
Clinical Features
Onset: Acute to subacute (days to weeks after triggering event)
| Feature | Description |
|---|---|
| Encephalopathy | Hallmark — confusion, lethargy, behavioral changes (required in most diagnostic criteria) |
| Fever | Common at onset |
| Multifocal neurological deficits | Motor weakness, ataxia, cranial nerve palsies, sensory changes |
| Seizures | ~13–35%, especially in children |
| Optic neuritis | Unilateral or bilateral |
| Meningismus | Headache, neck stiffness |
| Spinal cord involvement | Transverse myelitis features (weakness, bowel/bladder dysfunction) |
MRI Findings
The cornerstone of diagnosis.
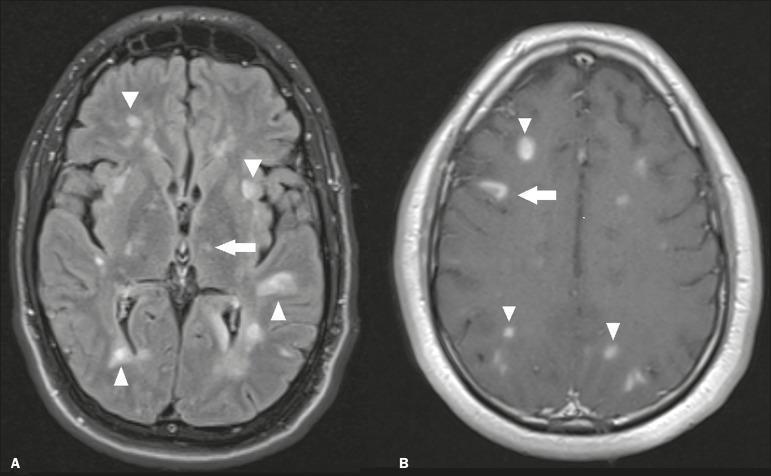
Axial FLAIR (left): Multiple poorly defined hyperintense lesions in bilateral subcortical and deep white matter (arrowheads) with left thalamic involvement (arrow). Contrast T1 (right): Nodular and open-ring (annular) enhancement of active lesions — classic for ADEM.
| MRI Feature | ADEM |
|---|---|
| Lesion distribution | Bilateral, asymmetric, multifocal |
| Location | Subcortical & deep white matter, thalami, basal ganglia, brainstem, cerebellum, spinal cord |
| Lesion character | Large, poorly marginated, "fluffy" |
| T2/FLAIR | Hyperintense |
| Enhancement | Variable; nodular or open-ring pattern in active lesions |
| Grey matter involvement | Yes (thalamus, basal ganglia) — key distinction from MS |
| Periventricular lesions | Less prominent than in MS; lacks Dawson's fingers |
Diagnosis
No single gold-standard test. Diagnosis is clinical + radiological.
IPMSSG 2013 Diagnostic Criteria (for children):
- First polyfocal clinical CNS event of presumed inflammatory demyelinating cause
- Encephalopathy not explained by fever
- MRI abnormalities consistent with ADEM
- No new clinical/MRI features after 3 months
- Abnormalities not better explained by another diagnosis
Investigations:
- MRI brain + spine with contrast — essential
- CSF: Pleocytosis (lymphocytic, 10–200 cells/µL), elevated protein; oligoclonal bands usually absent (unlike MS)
- MOG-IgG antibody — positive in ~40–60% of children; important prognostic marker
- AQP4-IgG (NMO-IgG) — rule out NMOSD
- EEG — if seizures suspected
- Infectious workup — blood cultures, viral PCR, serology
Differential Diagnosis
| Condition | Key Distinguishing Features |
|---|---|
| Multiple Sclerosis | No encephalopathy; periventricular lesions (Dawson's fingers); OCBs in CSF; relapses |
| NMOSD | AQP4-IgG+; severe optic neuritis + longitudinally extensive transverse myelitis |
| MOG-antibody disease (MOGAD) | MOG-IgG+; can overlap with ADEM; may relapse |
| Viral encephalitis | No demyelination; positive PCR (HSV); temporal lobe predilection |
| CNS vasculitis | Stroke-like lesions; angiography abnormalities |
| Metabolic/toxic leukodystrophy | Symmetric lesions; no inflammation; gradual onset |
| CNS lymphoma | Periventricular lesions; immunocompromised host; biopsy needed |
Management
Acute Phase (first-line)
- IV Methylprednisolone 20–30 mg/kg/day (max 1 g/day) × 3–5 days → oral prednisone taper over 4–6 weeks
- Rapid taper is associated with relapse; a slow taper is recommended
Refractory Cases (second-line)
- IVIg 2 g/kg over 2–5 days
- Plasma exchange (PLEX) — especially if steroid-refractory or severe
Supportive Care
- Seizure management (AEDs if needed)
- ICP management if cerebral edema present
- Rehabilitation (physiotherapy, speech therapy, neuropsychological support)
Acute Hemorrhagic Leukoencephalitis (AHLE / Hurst Disease)
The most severe variant of ADEM. Features:
- Vasculitic, hemorrhagic lesions
- Hyperacute, devastating clinical course
- High mortality without aggressive treatment
- Treatment: high-dose steroids, cyclophosphamide, PLEX
Prognosis
| Outcome | Details |
|---|---|
| Most children | Full or near-full recovery (~70–90%) |
| Mortality | ~1–3% in children; higher in adults and AHLE |
| Residual deficits | Cognitive/behavioral issues, motor deficits in ~10–30% |
| Relapse | Monophasic in most; ~20–30% later reclassified as MS, MOGAD, or NMOSD |
| MOG-IgG+ ADEM | More likely to relapse; warrants close follow-up |
Key Points for Clinical Practice
- Encephalopathy is required — distinguishes ADEM from other demyelinating syndromes
- MOG-IgG testing is recommended in all cases — guides prognosis and surveillance
- Slow steroid taper reduces relapse risk
- Follow-up MRI at 3–6 months — new lesions would suggest MS or MOGAD, not monophasic ADEM
- Adults with apparent ADEM have a higher rate of eventual MS diagnosis than children (Harrison's, p. 12630)
This is a shared conversation. Sign in to Orris to start your own chat.