Ovarian tumors
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
"ovarian cancer" AND "treatment"
Loading Image
I now have comprehensive material from Robbins Pathology (pathology/classification), Schwartz's Surgery (staging/treatment), and Bailey & Love (clinical features/investigations). Here is the complete structured answer.
Ovarian Tumors
Overview
About 80% of ovarian tumors are benign, occurring mostly in women aged 20-45 years. Borderline tumors appear at slightly older ages. Malignant tumors peak between ages 45-65. Ovarian cancer accounts for 3% of female cancers and is the 5th most common cause of cancer death in women, with ~70% presenting at advanced stage due to nonspecific early symptoms.
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, p. 940
- Schwartz's Principles of Surgery, p. 1843
Classification (WHO)
Three tissues of origin form the basis:
| Category | Origin | Key Tumors |
|---|---|---|
| Surface Epithelial-Stromal | Müllerian/surface epithelium | Serous, mucinous, endometrioid, clear cell, Brenner |
| Sex Cord-Stromal | Stromal/sex cords | Granulosa cell, thecoma, fibroma, Sertoli-Leydig |
| Germ Cell | Migratory yolk-sac germ cells | Teratoma (mature/immature), dysgerminoma, yolk sac tumor |
| Metastatic | Non-ovarian primary | Gastric (Krukenberg), colorectal, breast, pancreatic |
Each group is further divided into benign, borderline (low malignant potential), and malignant.
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, p. 940 (Table 22.3)
Frequency of Major Tumor Types
| Type | % of Malignant Ovarian Tumors | % Bilateral |
|---|---|---|
| Serous (all grades) | 47% | Benign 25%, Malignant 65% |
| Endometrioid carcinoma | 20% | 40% |
| Undifferentiated carcinoma | 10% | -- |
| Clear cell carcinoma | 6% | 40% |
| Granulosa cell tumor | 5% | 5% |
| Mucinous | 3% | <5% malignant |
| Teratoma | 1% | Rare |
| Metastatic | 5% | >50% |
- Robbins, Cotran & Kumar - Pathologic Basis of Disease, p. 941 (Table 22.4)
1. Surface Epithelial Tumors (~65-70% of all ovarian tumors)
Most primary ovarian neoplasms arise from müllerian epithelium. These are classified by:
- Cell type: serous, mucinous, endometrioid, clear cell, Brenner
- Degree of proliferation: benign / borderline / malignant
Type I vs. Type II Epithelial Cancers
| Feature | Type I | Type II |
|---|---|---|
| Histology | LG serous, LG endometrioid, clear cell, mucinous | HG serous (70%), HG endometrioid, carcinosarcoma |
| Key mutations | KRAS, BRAF, PTEN, PIK3CA, ARID1A | TP53 (hallmark) |
| Behavior | Slow-growing, often caught earlier | Aggressive, majority present advanced |
| Risk factors | Endometriosis, hormonal factors | BRCA1/2 germline mutations |
- Schwartz's Principles of Surgery, p. 1843
Serous Tumors (most common epithelial type)
- Benign serous cystadenoma: Smooth-walled, unilocular or bilocular cyst lined by fallopian tube-type ciliated columnar epithelium. 25% bilateral.
- Borderline serous tumor: Epithelial proliferation without stromal invasion. 30% bilateral. Can implant on peritoneum but favorable prognosis.
- Malignant serous adenocarcinoma: The most common ovarian malignancy overall. Psammoma bodies (laminated calcifications) are characteristic. High-grade form has ubiquitous TP53 mutations. 65% bilateral.
Mucinous Tumors
- Large, multilocular cysts filled with mucin. Can grow enormous (>25 kg).
- Lined by endocervical-type or intestinal-type epithelium.
- Pseudomyxoma peritonei: Extensive mucinous ascites from rupture - usually from appendiceal primary with ovarian spread.
- Rarely bilateral (<5% malignant mucinous).
Endometrioid Tumors
- Associated with endometriosis (in ~15-20% of cases the ipsilateral ovary has endometriosis).
- 20% of co-existing endometrial carcinoma - consider synchronous primaries.
- 40% bilateral when malignant.
Clear Cell Carcinoma
- Large cells with abundant clear cytoplasm; hobnail cells lining cysts.
- Often arises in endometriosis; resistant to platinum-based chemotherapy.
Brenner Tumors
- Nests of transitional (urothelial-type) cells in dense fibrous stroma.
- Usually benign, small, and asymptomatic. May produce estrogen (thecomatous stroma).
2. Germ Cell Tumors (~15-20%)
Mainly in women under 30 years. Tumor markers are key.
| Tumor | Marker(s) | Key Features |
|---|---|---|
| Mature cystic teratoma (dermoid cyst) | None | Most common benign ovarian tumor overall. Contains ectoderm (hair, teeth, skin). Mostly unilateral. |
| Immature teratoma | AFP (may be elevated) | Malignant. Contains immature neuroepithelium. Grade 1-3 by amount of immature tissue. |
| Dysgerminoma | LDH, β-hCG (rarely) | Most common malignant GCT. Equivalent of testicular seminoma. Very radiosensitive and chemosensitive. |
| Yolk sac tumor (endodermal sinus tumor) | AFP | Highly malignant. Schiller-Duval bodies pathognomonic. |
| Choriocarcinoma | β-hCG | Rare; highly malignant; gestational vs. nongestational forms |
| Struma ovarii | Thyroid hormones (rarely) | Monodermal teratoma - predominantly thyroid tissue |
For women <40 with suspected complex ovarian mass: measure LDH, AFP, inhibin, β-hCG to exclude germ cell tumors. - Bailey and Love's, p. 1614
3. Sex Cord-Stromal Tumors (~5-10%)
Functionally active tumors that produce hormones.
| Tumor | Hormone | Clinical Effect |
|---|---|---|
| Granulosa cell tumor | Estrogen | Precocious puberty (children); postmenopausal bleeding; Call-Exner bodies on histology; risk of endometrial carcinoma. Low-grade malignant potential. |
| Thecoma/fibrothecoma | Estrogen | Usually benign; estrogenic effects; associated with Meigs' syndrome (fibroma + ascites + pleural effusion). |
| Fibroma | None | Purely fibrous; associated with Meigs' syndrome (benign fibroma + ascites + pleural effusion). Basal cell nevus syndrome. |
| Sertoli-Leydig cell tumor (androblastoma) | Androgens | Virilization, hirsutism, amenorrhea. Usually benign or low-grade malignant. |
4. Metastatic Tumors to Ovary (~5%)
- Krukenberg tumor: Bilateral ovarian metastases from gastric cancer (or colorectal, breast). Signet-ring cells secreting mucin within ovarian stroma. Both ovaries enlarged but retain their shape.
- Other primaries: appendiceal, pancreaticobiliary, colorectal, breast.
Clinical Presentation
Symptoms are generally nonspecific:
- Abdominal distension, bloating
- Pelvic or abdominal pain
- Difficulty eating/early satiety
- Urinary urgency/frequency
- Weight gain/increased girth (ascites)
- Pelvic mass ± ascites
Over half initially present to a non-gynecology specialist with vague symptoms of metastatic disease (shortness of breath, GI disturbance, change in bowel habit).
Pelvic mass + ascites = ovarian cancer until proved otherwise (but exclude Meigs' syndrome).
- Bailey and Love's Short Practice of Surgery, p. 1613-1614
Risk Factors
- Increases risk: nulliparity, early menarche, late menopause, infertility, BRCA1/2 mutations (lifetime risk 20-45% for BRCA1, 10-20% for BRCA2), family history of ovarian/breast cancer, Lynch syndrome
- Decreases risk: oral contraceptive use (protection persists up to 30 years after cessation), tubal ligation, hysterectomy, breastfeeding, salpingectomy
Up to 18-24% of ovarian carcinomas arise with a hereditary predisposition. NCCN recommends genetic testing for all women diagnosed with ovarian cancer.
Investigations
Tumor Markers
| Marker | Tumor Type |
|---|---|
| CA-125 | Epithelial ovarian cancer (elevated in 50% stage I, >90% advanced) |
| AFP | Yolk sac tumor, immature teratoma |
| β-hCG | Dysgerminoma, choriocarcinoma |
| LDH | Dysgerminoma |
| Inhibin | Granulosa cell tumor, mucinous tumors |
| CEA, CA 19-9 | Mucinous tumors |
CA-125 is non-specific - also elevated in endometriosis, PID, liver disease, other cancers, menstruation, and ascites. Normal cut-off: 35 U/mL.
Imaging
Ultrasound is first-line. The IOTA group B-rules (benign) and M-rules (malignant) guide assessment:
| Benign features (B-rules) | Malignant features (M-rules) |
|---|---|
| Unilocular cyst | Irregular solid tumor |
| Solid components <7mm | Ascites |
| Acoustic shadowing | ≥4 papillary structures |
| Smooth multilocular <100mm | Irregular multilocular ≥100mm |
| No blood flow | Blood flow present |
CT or MRI for staging prior to surgery. CT is preferred for evaluating upper abdominal disease resectability.
Risk of Malignancy Index (RMI)
RMI = U × M × CA-125
-
U = ultrasound score (1 point each for: multilocular, solid components, metastases, ascites, bilateral) - score 0, 1, or 3
-
M = menopausal status (1 = premenopausal; 3 = postmenopausal)
-
CA-125 in U/mL
-
Bailey and Love's Short Practice of Surgery, p. 1614
FIGO Staging (2014) - Epithelial Ovarian Cancer
| Stage | Description |
|---|---|
| I | Confined to ovaries/fallopian tubes |
| IA | One ovary, capsule intact, no surface tumor, negative washings |
| IB | Both ovaries, capsule intact, no surface tumor |
| IC | One/both ovaries with surgical spill (IC1), ruptured capsule/surface tumor (IC2), or malignant cells in ascites/washings (IC3) |
| II | Pelvic extension (below pelvic brim) |
| IIA | Extension to uterus/tubes/ovaries |
| IIB | Extension to other pelvic tissues |
| III | Peritoneal spread outside pelvis and/or retroperitoneal nodes |
| IIIA1 | Positive retroperitoneal nodes only |
| IIIA2 | Microscopic extrapelvic peritoneal involvement |
| IIIB | Macroscopic peritoneal metastases ≤2cm |
| IIIC | Macroscopic peritoneal metastases >2cm |
| IV | Distant metastasis |
| IVA | Pleural effusion with positive cytology |
| IVB | Extra-abdominal organ metastases |
- Schwartz's Principles of Surgery, p. 1844
Treatment
Early-Stage (I-II)
- Stage IA/IB, low-grade: Complete surgical staging - total hysterectomy, bilateral salpingo-oophorectomy (BSO), omentectomy, peritoneal biopsies, node sampling. Cure rate ~90-95%. No adjuvant chemotherapy needed for grade 1-2.
- Stage IC, grade 3, all clear cell: 3-6 cycles adjuvant platinum + taxane chemotherapy.
- Fertility-sparing surgery possible for early-stage disease in young women.
Advanced-Stage (III-IV)
Surgery goals: (1) histologic diagnosis, (2) complete staging, (3) cytoreduction (debulking).
- Optimal cytoreduction: residual tumor ≤1 cm (historically); contemporary data favor no gross residual disease as the most favorable prognostic endpoint.
- Primary debulking surgery (PDS) followed by platinum/taxane chemotherapy remains standard.
- Neoadjuvant chemotherapy (NACT) followed by interval debulking: used for medically compromised patients or where complete primary cytoreduction is unlikely. Two RCTs showed equivalent survival to PDS.
Chemotherapy
- First-line: Carboplatin + paclitaxel (6 cycles). Bevacizumab may be added for high-risk patients.
- PARP inhibitors (olaparib, niraparib, rucaparib): maintenance therapy after first-line chemotherapy, especially in BRCA1/2-mutated or HRD-positive tumors. A 2025 meta-analysis (PMID: 41191357) confirms PFS benefit with PARP inhibitor maintenance in advanced epithelial ovarian cancer.
- 2025 ASCO guideline update (PMID: 39841949): NACT is an appropriate alternative to PDS for advanced ovarian cancer, with select criteria for patient selection.
Germ Cell Tumors
- Highly chemosensitive: BEP regimen (bleomycin, etoposide, cisplatin).
- Dysgerminoma is also radiosensitive.
- Fertility-sparing surgery is the norm for young patients with unilateral disease.
Sex Cord-Stromal Tumors
- Surgery is primary treatment (unilateral oophorectomy if fertility desired).
- Granulosa cell tumors: monitor with inhibin levels. BEP or taxane-platinum for recurrence.
Prevention and Screening
- No national screening program exists (no mortality benefit demonstrated for CA-125 or ultrasound screening in general population).
- Risk-reducing salpingo-oophorectomy: reduces lifetime HGSC risk to <3% in BRCA mutation carriers.
- Opportunistic salpingectomy at the time of other pelvic surgery is now recommended as a cancer prevention strategy, given fallopian tube origin of most high-grade serous cancers.
Intraoperative View
Below is an intraoperative view of ovarian cystectomy:
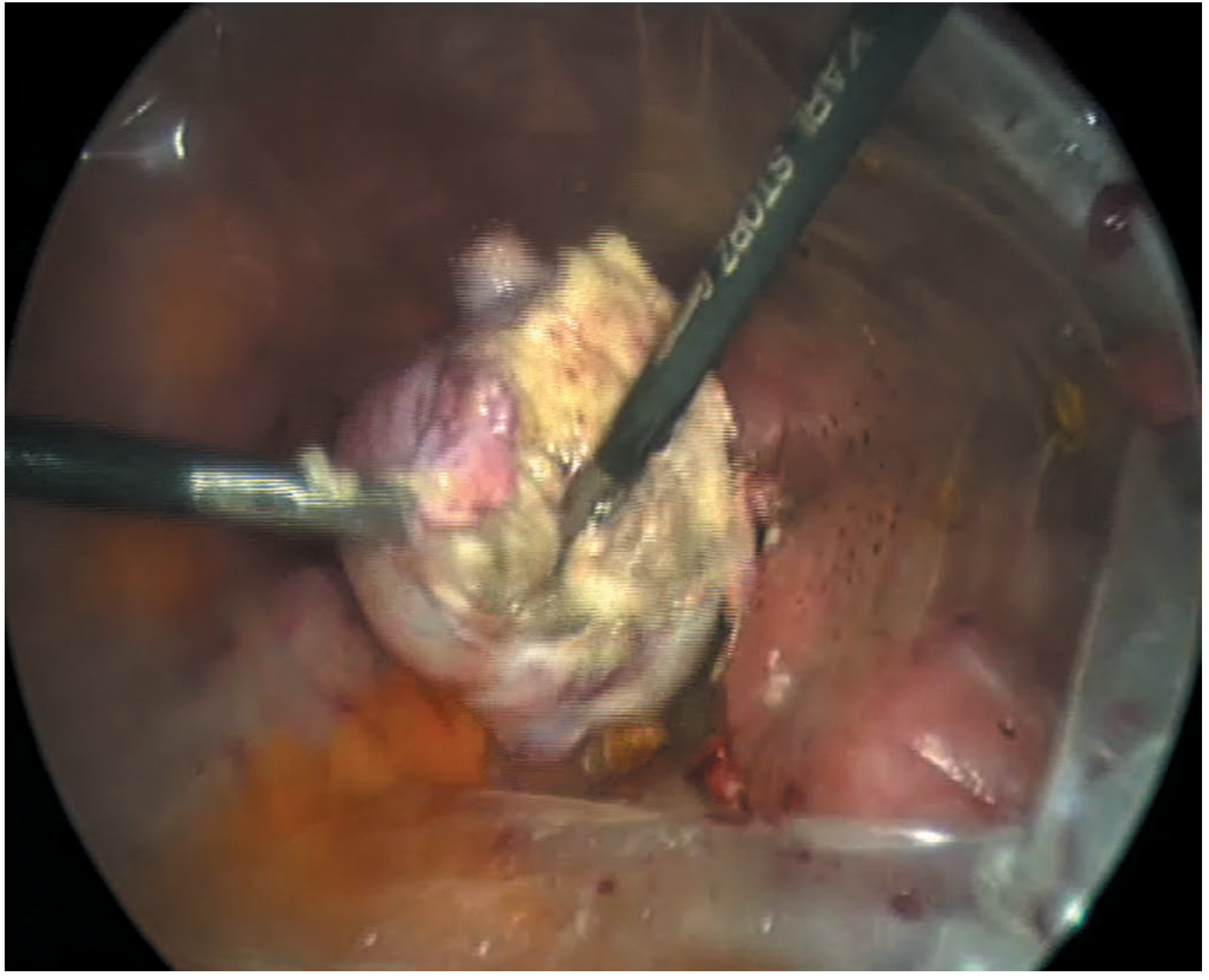
Bailey and Love's Short Practice of Surgery - Figure 87.24: Ovarian cystectomy
Key Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (p. 940-944) | Schwartz's Principles of Surgery, 11th Ed. (p. 1843-1845) | Bailey and Love's Short Practice of Surgery, 28th Ed. (p. 1613-1614)
Ovarian tumors
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Searching PubMed
"ovarian cancer" AND "treatment"
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the content needed for a comprehensive, richly illustrated answer. Here is the full response:
Ovarian Tumors
Overview
About 80% of ovarian tumors are benign, occurring mostly in women aged 20-45. Borderline tumors appear at slightly older ages. Malignant tumors are most common between 45-65. Ovarian cancer accounts for 3% of all female cancers and is the 5th most common cause of cancer death in women - yet it kills more women than any other gynecologic malignancy because ~70% present at advanced stage.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 940
Classification (WHO)
Ovarian tumors arise from one of three tissue components:
| Category | Tissue of Origin | Examples |
|---|---|---|
| Surface Epithelial-Stromal (~65%) | Müllerian/surface epithelium, endometriosis | Serous, mucinous, endometrioid, clear cell, Brenner |
| Germ Cell (~15-20%) | Pluripotent germ cells migrating from yolk sac | Teratoma, dysgerminoma, yolk sac tumor, choriocarcinoma |
| Sex Cord-Stromal (~5-10%) | Embryonic sex cords and gonadal mesenchyme | Granulosa cell, thecoma, fibroma, Sertoli-Leydig |
| Metastatic (~5%) | Non-ovarian primary | Gastric/colorectal (Krukenberg), breast, appendiceal |
Each category is further divided into benign, borderline (low malignant potential), and malignant.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 940 (Table 22.3)
Frequency of Major Types
| Type | % of Malignant Tumors | % Bilateral |
|---|---|---|
| Serous (all) | 47% | Benign 25%, Malignant 65% |
| Endometrioid carcinoma | 20% | 40% |
| Undifferentiated carcinoma | 10% | - |
| Clear cell carcinoma | 6% | 40% |
| Granulosa cell tumor | 5% | 5% |
| Mucinous | 3% | <5% (malignant) |
| Teratoma | 1% | Rare |
| Metastatic | 5% | >50% |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 941 (Table 22.4)
1. Surface Epithelial Tumors
Most primary ovarian neoplasms arise from müllerian epithelium. All subtypes are classified as benign, borderline, or malignant.
Type I vs. Type II Epithelial Cancer - Key Distinction
| Feature | Type I (Low-Grade) | Type II (High-Grade) |
|---|---|---|
| Histology | LG serous, LG endometrioid, clear cell, mucinous | HG serous (70%), HG endometrioid, carcinosarcoma |
| Driver mutations | KRAS, BRAF, PTEN, PIK3CA, ARID1A | TP53 (hallmark; rare in Type I) |
| Precursor | Borderline tumor / endometriosis | STIC (serous tubal intraepithelial carcinoma) |
| Behavior | Slow-growing, often confined | Aggressive, majority present advanced |
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 941
a. Serous Tumors (most common - 50% of all ovarian cancers)
- Benign serous cystadenoma: Smooth-walled, unilocular or bilocular cyst lined by fallopian tube-type ciliated columnar epithelium. Most common in women 20-45. 25% bilateral.
- Borderline serous tumor: Epithelial proliferation without stromal invasion. 30% bilateral. Good prognosis even with peritoneal implants.
- Low-grade serous carcinoma: Arises from borderline tumors. KRAS/BRAF mutations.
- High-grade serous carcinoma (HGSC): Most common and most lethal ovarian malignancy. Arises from STIC in fallopian tube fimbriae. TP53 mutations ubiquitous. Psammoma bodies (laminated calcific concretions) are characteristic. 65% bilateral. Strongly linked to BRCA1/2 mutations.
Pathogenesis diagram (Type I vs Type II pathway - Robbins Fig. 22.29):
Type I tumors progress: benign cystadenoma → borderline tumor → low-grade carcinoma (KRAS/BRAF/PTEN mutations). Type II tumors arise from STIC/inclusion cysts with TP53 mutation → high-grade serous carcinoma.
b. Mucinous Tumors
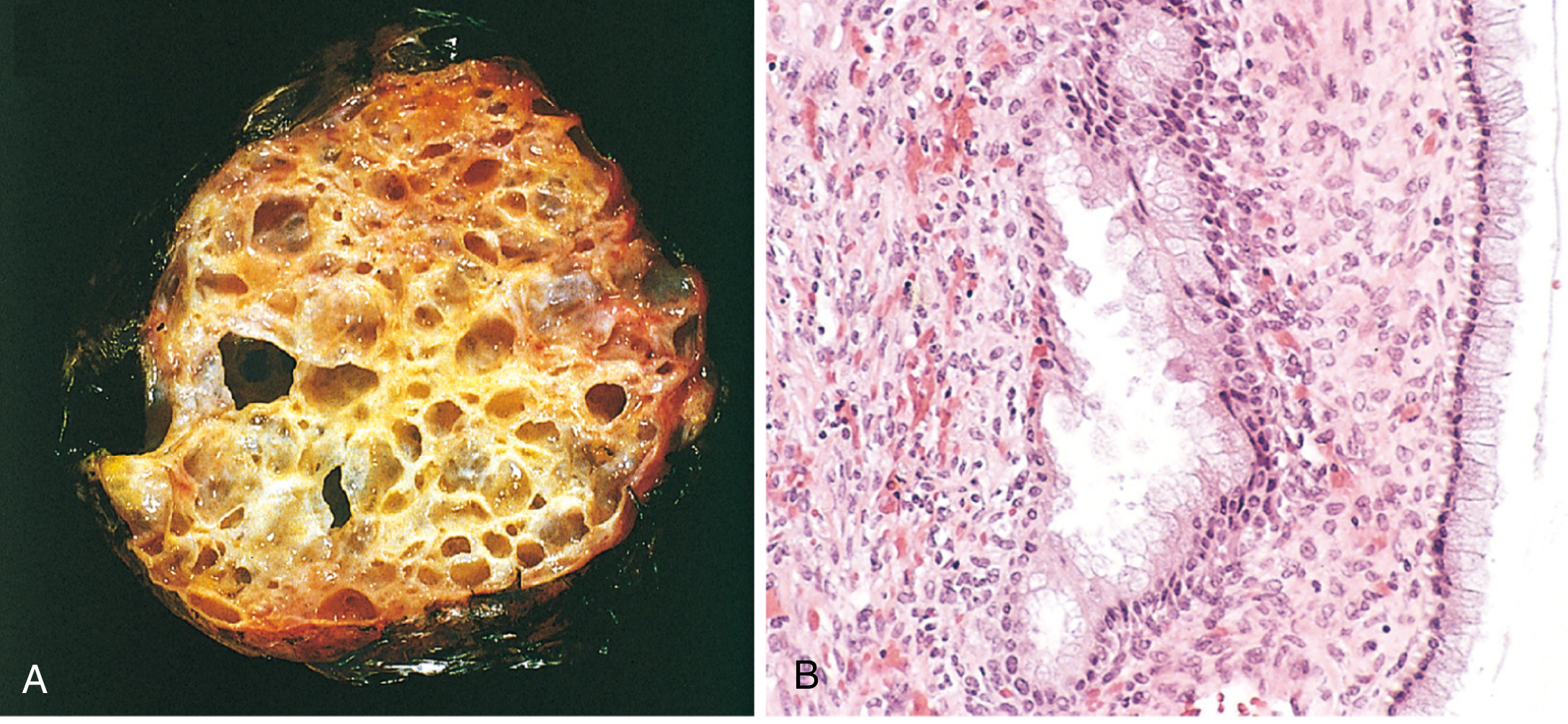
Fig. 22.33 Mucinous cystadenoma - (A) multicystic appearance with glistening mucin; (B) columnar cells lining the cysts. - Robbins Pathology
- Large multiloculated cysts filled with viscous mucin; can reach >25 kg.
- Lined by endocervical-type or intestinal-type epithelium (goblet cells).
- 80% benign, 10% borderline, 10% malignant.
- Pseudomyxoma peritonei: massive mucus accumulation in the peritoneal cavity from tumor rupture - most commonly appendiceal primary.
- Rarely bilateral (<5% malignant); unilateral predominance distinguishes them from serous.
c. Endometrioid Tumors (20% of malignant ovarian tumors)
- Tubular glands resembling benign or malignant endometrium on histology.
- 15-30% of cases co-exist with endometrial carcinoma (usually metastatic from uterus rather than synchronous primary).
- 15-20% arise in association with endometriosis - a recognized precursor.
- Shared mutations with endometrial carcinoma: PTEN, PIK3CA, ARID1A, KRAS.
- 40% bilateral. 5-year survival for Stage I ~75%.
d. Clear Cell Carcinoma (6%)
- Large epithelial cells with abundant clear cytoplasm; hobnail cells lining cyst spaces.
- Associated with endometriosis and endometrioid carcinoma of the ovary.
- Shared mutations with endometrioid type: PIK3CA, ARID1A, KRAS, PTEN.
- Often platinum-resistant - adverse prognosis in advanced stage.
- Stage I confined to ovary: ~90% 5-year survival.
e. Brenner Tumors
- Nests of transitional (urothelial-like) epithelial cells in a dense fibrous stroma.
- Usually small, benign, and asymptomatic - discovered incidentally.
- May produce estrogen from thecomatous stromal component.
- Rare malignant variants exist.
2. Germ Cell Tumors (15-20% of all ovarian tumors)
Predominantly in women under 30 years (children and young adults). Tumor markers are essential for diagnosis and follow-up.
| Tumor | Marker | Key Features |
|---|---|---|
| Mature cystic teratoma (dermoid cyst) | None | Most common benign ovarian tumor overall. Contains ectodermal elements (hair, teeth, skin, sebaceous). 96% benign; 1% undergo malignant transformation (usually SCC). |
| Immature teratoma | AFP (sometimes) | Malignant; contains primitive neuroepithelium. Graded I-III by amount of immature tissue. Mean age 18 years. |
| Dysgerminoma | LDH; rarely β-hCG | Most common malignant GCT (~50% of malignant GCTs). Ovarian counterpart of testicular seminoma. KIT mutations (30-50%). Highly chemosensitive and radiosensitive. 80-90% unilateral. >90% 10-year survival for Stage I after surgery. |
| Yolk sac tumor | AFP | Highly malignant. Schiller-Duval bodies (perivascular glomeruloid structures) pathognomonic. Hyaline globules (AFP-positive). |
| Choriocarcinoma | β-hCG | Rare; highly malignant. Non-gestational type worse prognosis than gestational. |
| Struma ovarii | Thyroid hormones | Monodermal teratoma composed entirely of thyroid tissue; may cause hyperthyroidism. |
| Carcinoid | 5-HIAA, serotonin | Monodermal; carcinoid syndrome if >7 cm (ovarian veins drain directly to systemic circulation). |
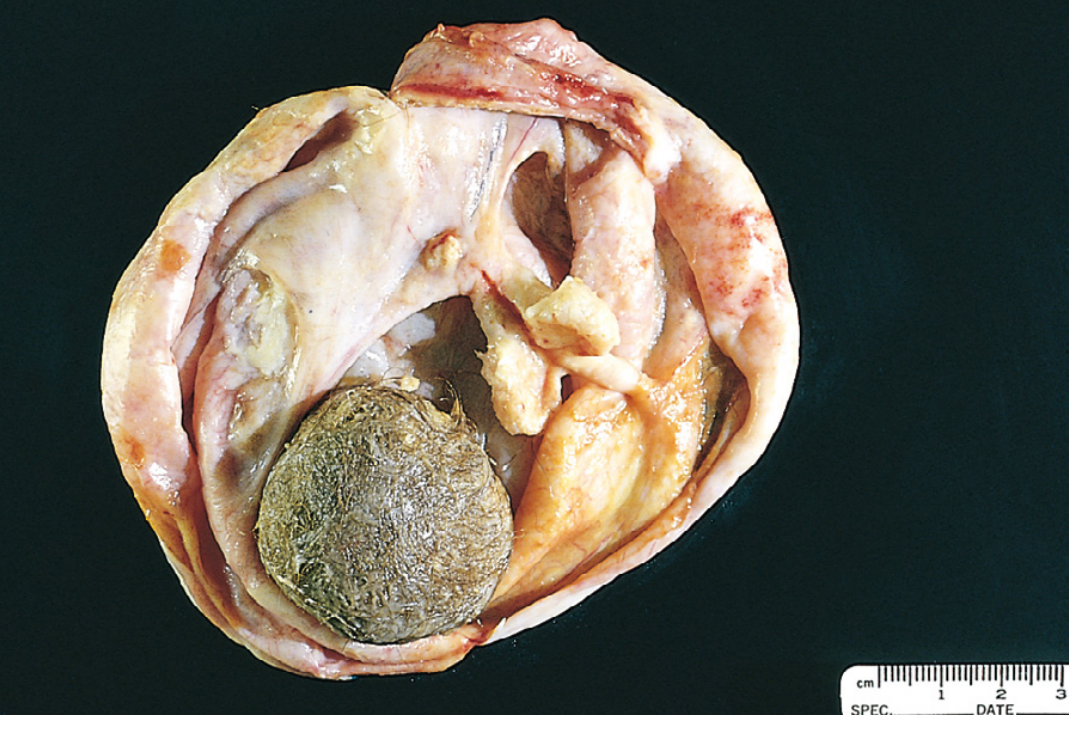
Fig. 22.36 Opened mature cystic teratoma (dermoid cyst) showing hair and mixed tissue contents. - Robbins Pathology
Key concepts for GCTs:
-
Germ cells differentiate toward: oogonia (dysgerminoma), extraembryonic yolk sac (yolk sac tumor), placenta (choriocarcinoma), or multiple germ layers (teratoma).
-
Immature teratoma grading: based on proportion of immature neuroepithelium.
-
BEP chemotherapy (bleomycin, etoposide, cisplatin) is the standard regimen.
-
Fertility-sparing surgery is the norm in young patients with unilateral disease.
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 946-947
3. Sex Cord-Stromal Tumors
Arise from gonadal mesenchyme; the undifferentiated mesenchyme gives rise to female-type cells (granulosa, theca) or male-type cells (Sertoli, Leydig). Hence these tumors are often hormonally active.
a. Granulosa Cell Tumors (5% of all ovarian tumors)
- Cells resemble granulosa cells of a developing follicle. 95% are adult type; 5% juvenile type.
- Two-thirds occur in postmenopausal women.
- Call-Exner bodies: small, glandlike structures filled with acidophilic material - pathognomonic when present.
- Strongly inhibin-positive on immunohistochemistry (Fig. 22.41B, shown below).
- Hallmark mutation: FOXL2 mutation in 97% of adult granulosa cell tumors.
- Estrogenic - causes endometrial hyperplasia/carcinoma (10-15% of cases), breast disease, and precocious puberty (in juvenile type with AKT1/GNAS mutations).
- All potentially malignant but indolent course - recurrences may appear 10-20 years later.
- Stage I 10-year survival ~90-95%.
- Monitor with serum inhibin levels.
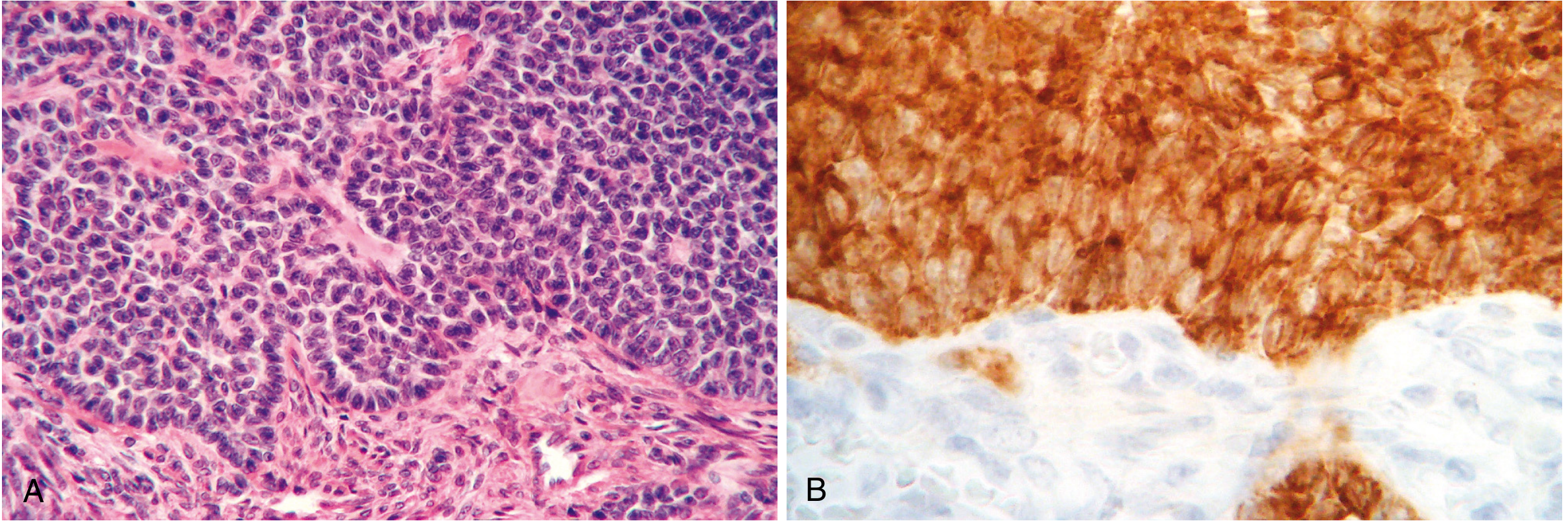
Fig. 22.41 Granulosa cell tumor: (A) Call-Exner bodies on H&E; (B) strong inhibin immunopositivity. - Robbins Pathology
b. Fibromas and Thecomas (4% of all ovarian tumors)
- Fibromas: Solid, hard, gray-white, encapsulated masses composed of well-differentiated fibroblasts. 90% unilateral.
- Meigs' syndrome: Fibroma + ascites + right-sided pleural effusion (occurs in ~40% of tumors >6 cm). All resolve after tumor resection. Hormonally inactive.
- Associated with basal cell nevus (Gorlin) syndrome.
- Thecomas: Composed of plump spindle cells with lipid droplets. Produce estrogen. Rare and almost never malignant.
- Fibromathecoma: Mixed composition.
c. Sertoli-Leydig Cell Tumors (Androblastoma)
- Resemble testicular Sertoli and Leydig cells.
- Produce androgens → defeminization and virilization: amenorrhea, breast atrophy, hirsutism, clitoral hypertrophy, voice changes.
- Usually low-grade malignant; recurrence/metastasis rate <5%.
- Juvenile granulosa cell tumors: AKT1 (60%) and GNAS (30%) mutations.
d. Other Sex Cord-Stromal Tumors
-
Leydig cell tumors: Unilateral, hilar location; contain Reinke crystalloids; produce testosterone; masculinization but milder than Sertoli-Leydig; almost always benign.
-
Gonadoblastoma: Germ cells + sex cord derivatives in phenotypic females with gonadal dysgenesis (often 46,XY); 50% have coexistent dysgerminoma.
-
Steroid (lipid) cell tumors: Produce androgens/estrogens.
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 948-950
4. Metastatic Tumors (~5%)
-
Krukenberg tumor: Bilateral ovarian metastases from gastric carcinoma (most common) or colorectal/biliary/breast. Classic histology: mucin-producing signet-ring cells within hyperplastic ovarian stroma. Both ovaries enlarged but retain their shape. >50% bilateral - bilaterality of any ovarian mass should raise suspicion for metastasis.
-
Other primaries: appendiceal (pseudomyxoma peritonei), colon, pancreatic, breast.
-
Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 950
Clinical Presentation
Symptoms are nonspecific until late disease:
- Abdominal distension / bloating
- Pelvic or abdominal pain
- Change in appetite / early satiety
- Urinary urgency or frequency
- Weight gain, increased girth (ascites)
Over half of women initially present to a non-gynecology specialist with metastatic symptoms (shortness of breath, GI disturbance, change in bowel habit). Ovarian cancer must be in the differential for any woman with persistent, non-specific abdominal symptoms.
Pelvic mass + ascites = ovarian cancer until proved otherwise (exclude Meigs' syndrome = benign fibroma + ascites + pleural effusion).
- Bailey and Love's Short Practice of Surgery 28th Ed., p. 1613
Risk Factors
Increase risk:
- Nulliparity, low parity
- Early menarche, late menopause
- BRCA1 mutation (lifetime risk 20-60%), BRCA2 mutation
- Family history (breast or ovarian cancer)
- Lynch syndrome (endometrioid/clear cell histology)
- Hormone replacement therapy (long-term)
Decrease risk:
- Oral contraceptive use (protection persists up to 30 years after cessation)
- Tubal ligation / hysterectomy
- Breastfeeding, multiparity
- Opportunistic salpingectomy - now recommended at time of other pelvic surgery given fallopian tube origin of most HGSCs
BRCA1 mutations present in ~5% of patients <70 years with ovarian cancer. NCCN recommends genetic testing for all women diagnosed with ovarian cancer, regardless of family history.
Investigations
Tumor Markers by Tumor Type
| Tumor | Key Marker(s) |
|---|---|
| Epithelial (especially serous) | CA-125 (normal <35 U/mL) |
| Yolk sac tumor | AFP |
| Dysgerminoma | LDH; rarely β-hCG |
| Choriocarcinoma | β-hCG |
| Granulosa cell / mucinous | Inhibin |
| Mucinous | CA 19-9, CEA |
CA-125 caveats: Elevated in 50% of Stage I and >90% of advanced disease; but also raised in endometriosis, PID, liver disease, other malignancies, menstruation, and ascites. Non-specific alone.
For women <40 with a suspected complex ovarian mass: measure LDH, AFP, inhibin, β-hCG to exclude germ cell tumors.
Imaging
- Ultrasound (TVUS) is first-line. IOTA group B-rules and M-rules guide assessment:
| Benign (B-rules) | Malignant (M-rules) |
|---|---|
| Unilocular cyst | Irregular solid tumor |
| Solid component <7 mm | Ascites |
| Acoustic shadowing | ≥4 papillary structures |
| Smooth multilocular <100 mm | Irregular multilocular ≥100 mm |
| No blood flow | Blood flow present |
- CT scan: staging investigation; preferred for evaluating upper abdominal disease resectability in advanced cancer.
- MRI: characterization of indeterminate pelvic mass.
Risk of Malignancy Index (RMI)
RMI = U × M × CA-125
- U = ultrasound score (0, 1, or 3 based on number of malignant features: multilocular, solid components, metastases, ascites, bilateral)
- M = menopausal status: premenopausal = 1; postmenopausal = 3
- CA-125 = level in U/mL
RMI >200 typically prompts referral to a gynecological oncologist.
- Bailey and Love's Short Practice of Surgery 28th Ed., p. 1614
FIGO Staging (2014) - Epithelial Ovarian Cancer
| Stage | Description |
|---|---|
| I | Confined to ovaries/fallopian tubes |
| IA | One ovary; capsule intact; no surface tumor; negative washings |
| IB | Both ovaries; capsules intact |
| IC | One/both ovaries with: IC1 surgical spill; IC2 ruptured capsule/surface tumor; IC3 malignant cells in ascites/washings |
| II | Pelvic extension |
| IIA | Extension to uterus/tubes/ovaries |
| IIB | Extension to other pelvic tissues |
| III | Peritoneal spread outside pelvis ± retroperitoneal nodes |
| IIIA1 | Positive retroperitoneal nodes only |
| IIIA2 | Microscopic extrapelvic peritoneal involvement |
| IIIB | Macroscopic peritoneal metastases ≤2 cm |
| IIIC | Macroscopic peritoneal metastases >2 cm |
| IV | Distant metastasis |
| IVA | Pleural effusion with positive cytology |
| IVB | Extra-abdominal organ metastases |
- Schwartz's Principles of Surgery 11th Ed., p. 1844
Treatment
Epithelial Ovarian Cancer
Early Stage (I-II):
- Surgery: total hysterectomy + BSO + omentectomy + peritoneal biopsies + pelvic/para-aortic lymph node sampling.
- Stage IA/IB grade 1-2: surgery alone; cure rate ~90-95%.
- Stage IC, grade 3, or clear cell histology: 3-6 cycles adjuvant carboplatin + paclitaxel.
Advanced Stage (III-IV):
- Three surgical objectives: (1) histologic diagnosis; (2) complete staging; (3) cytoreduction (debulking).
- Optimal cytoreduction: residual tumor ≤1 cm; best survival with no gross residual disease.
- Standard: primary debulking surgery (PDS) followed by carboplatin + paclitaxel.
- Neoadjuvant chemotherapy (NACT) + interval debulking: acceptable alternative for medically unfit patients or when complete PDS is unlikely. Two RCTs showed equivalent survival to PDS. Per the 2025 ASCO guideline update (PMID: 39841949), NACT is an appropriate alternative for carefully selected patients.
- PARP inhibitors (olaparib, niraparib, rucaparib): maintenance therapy post first-line chemotherapy, especially for BRCA1/2-mutated or HRD-positive tumors. A 2025 meta-analysis (PMID: 41191357) confirms significant PFS benefit with PARP inhibitor maintenance in advanced disease.
- Bevacizumab (anti-VEGF): may be added for high-risk patients.
- Fertility-sparing surgery guidelines: ESGO/ESHRE/ESGE 2024 guidance (PMID: 39216500) covers fertility-sparing treatment for early-stage disease.
Germ Cell Tumors
- BEP (bleomycin, etoposide, cisplatin): highly effective; most GCTs are chemosensitive.
- Dysgerminoma is also radiosensitive.
- Fertility-sparing unilateral oophorectomy standard in young patients with unilateral disease.
- Bilateral involvement/dysgerminoma: up to 15% bilateral - inspect contralateral ovary.
Sex Cord-Stromal Tumors
- Surgery primary treatment; unilateral oophorectomy if fertility desired.
- Granulosa cell tumors: monitor inhibin levels; recurrence may be 10-20 years later; BEP or taxane-platinum for recurrence.
Screening
No national screening program exists because no test has been shown to reduce ovarian cancer mortality. CA-125 and TVUS screening trials have not demonstrated a mortality benefit in general population. Risk-reducing salpingo-oophorectomy in BRCA1/2 mutation carriers reduces HGSC lifetime risk to <3%.
Sources:
- Robbins, Cotran & Kumar - Pathologic Basis of Disease (pp. 940-950)
- Schwartz's Principles of Surgery 11th Ed. (pp. 1843-1845)
- Bailey and Love's Short Practice of Surgery 28th Ed. (pp. 1613-1614)
This is a shared conversation. Sign in to Orris to start your own chat.