

Assignment: A) Prescribe single drug for an adult patient suffering from seasonal asthma. B) Prescribe drug therapy for an adult patient suffering from Chronic Obstructive Pulmonary Disease (COPD). C) Criticize, correct and rewrite the following prescription for an adult patient suffering from acute exacerbation of COPD: Tab Prednisolone 5mg 10 days Tab Theophylline 400 mg BD 10 days Tab Erythromycin 250 mg QID 10 days check is that all correct prescription writing and correct it and do assignment
seasonal allergic asthma single drug prescription salbutamol inhaler treatment
COPD chronic obstructive pulmonary disease drug therapy prescription tiotropium formoterol
acute exacerbation COPD prescription prednisolone theophylline antibiotic treatment
Prescriptions in Respiratory System
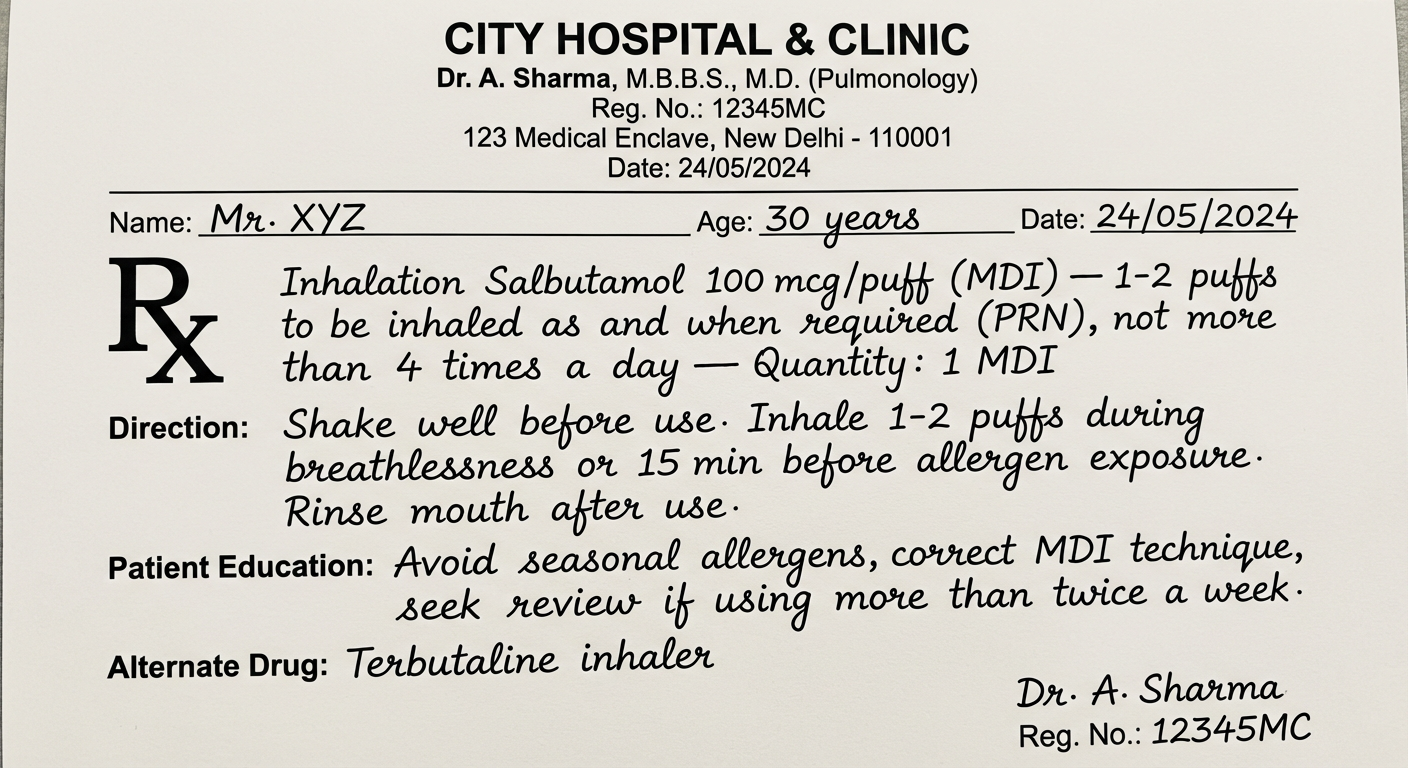
A) Single Drug Prescription — Adult Patient with Seasonal Asthma
Name: Mr./Ms. ___________ Age: ___ years | Date: ___________Rx
Drug Dose Quantity Inhalation Salbutamol 100 mcg/puff (MDI) 1–2 puffs to be inhaled as and when required (PRN), not more than 4 times a day __(1 MDI) Direction: Shake inhaler well before use. Inhale 1–2 puffs during symptomatic episodes or 15 minutes before known allergen/trigger exposure. Rinse mouth after use.Patient Education:
- Avoid known seasonal allergens (pollen, dust mites, cold air)
- Correct MDI technique to be demonstrated and practiced
- Seek medical review if needing rescue inhaler more than twice a week
Alternate Drug: Terbutaline inhaler (SABA)Dr. ___________ | Reg. No. ___________
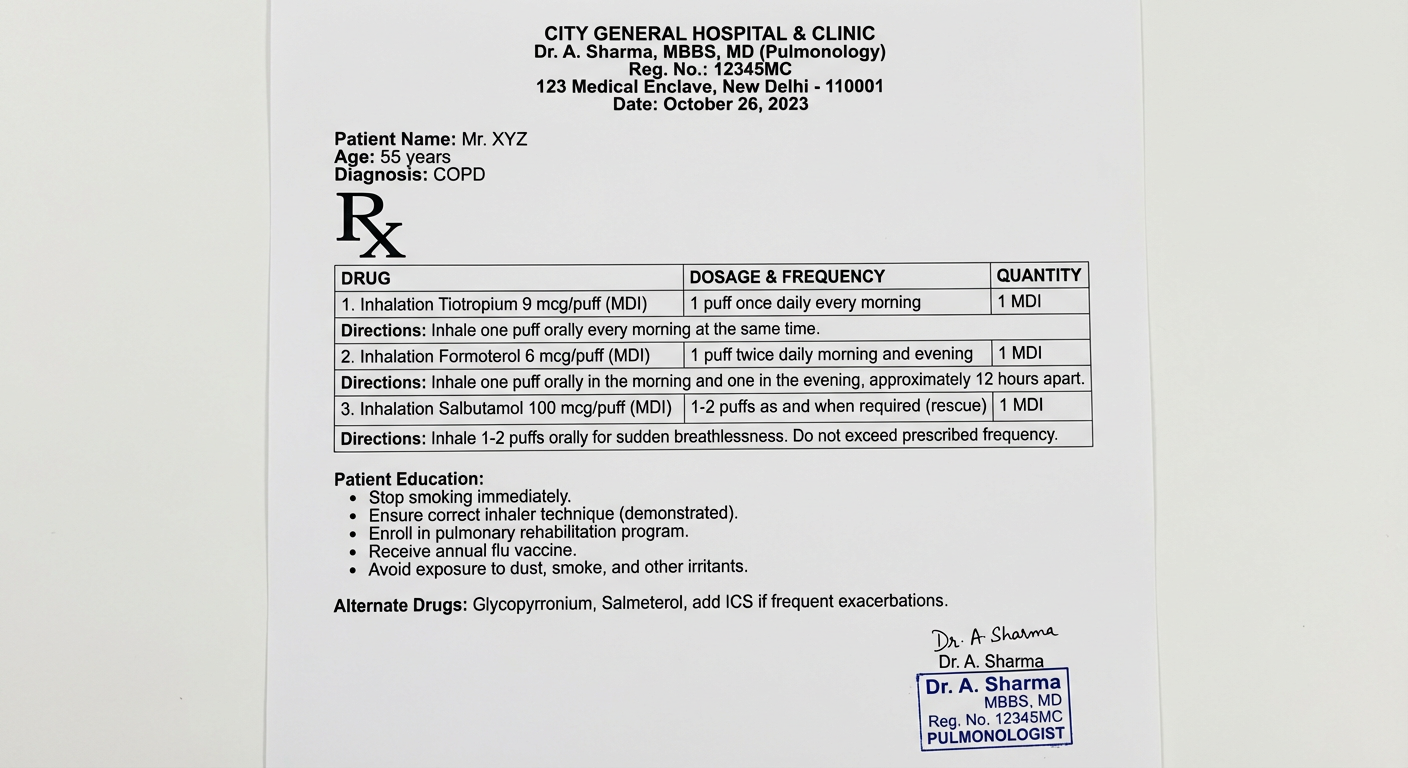
B) Drug Therapy Prescription — Adult Patient with COPD
Name: Mr./Ms. ___________ Age: ___ years | Date: ___________ Diagnosis: Chronic Obstructive Pulmonary Disease (COPD)Rx
Drug Dose Quantity Inhalation Tiotropium 9 mcg/puff (MDI) 1 puff to be inhaled once daily __(1 MDI) Inhalation Formoterol 6 mcg/puff (MDI) 1 puff to be inhaled twice daily __(1 MDI) Inhalation Salbutamol 100 mcg/puff (MDI) 1–2 puffs as and when required (rescue) __(1 MDI) Direction:
- Tiotropium: Inhale 1 puff every morning at the same time.
- Formoterol: Inhale 1 puff morning and evening.
- Salbutamol: Use only for acute breathlessness/rescue; do not exceed 4 puffs/day.
Patient Education:
- Stop smoking — most critical intervention in COPD
- Correct MDI/DPI inhaler technique to be demonstrated
- Pulmonary rehabilitation referral
- Annual influenza vaccination; pneumococcal vaccination
- Avoid smoke, dust, fumes, occupational irritants
- Monitor for worsening breathlessness, increased sputum (signs of exacerbation)
Alternate Drugs:
- LAMA: Glycopyrronium, Umeclidinium
- LABA: Salmeterol, Indacaterol
- Inhaled corticosteroid (ICS) to be added if frequent exacerbations or eosinophil count ≥ 300 cells/µL
Dr. ___________ | Reg. No. ___________
C) Critique, Correction and Rewriting of Prescription for Acute Exacerbation of COPD
Original Prescription (to be evaluated):
| Drug | Dose | Duration |
|---|---|---|
| Tab Prednisolone | 5 mg | 10 days |
| Tab Theophylline | 400 mg BD | 10 days |
| Tab Erythromycin | 250 mg QID | 10 days |
Detailed Criticism:
- ❌ Dose is critically inadequate. The evidence-based and GOLD 2025 recommended dose is 40 mg prednisolone equivalent per day for 5 days (GOLD 2025, p. 129). The prescribed 5 mg is 8× too low — completely subtherapeutic and will not shorten recovery, improve FEV₁, or reduce relapse risk.
- ❌ Duration of 10 days is excessive. The standard course is 5 days. Longer courses are associated with increased risk of pneumonia, sepsis, and mortality (GOLD 2025, p. 129).
- ✅ Route (oral) is acceptable — oral prednisolone is equally effective to IV.
- ❌ Theophylline is NOT recommended for acute exacerbation of COPD. GOLD 2025 guidelines do not recommend IV aminophylline or oral theophylline for acute exacerbations due to lack of efficacy evidence and significant toxicity risk (narrow therapeutic index, arrhythmias, seizures, GI effects).
- ❌ 400 mg BD = 800 mg/day is at the upper limit and risks toxicity without therapeutic benefit in this setting.
- ❌ Omission of bronchodilators: The prescription lacks short-acting bronchodilators (nebulised Salbutamol ± Ipratropium), which are the first-line bronchodilator treatment in acute COPD exacerbation.
- ❌ Dose is subtherapeutic. For respiratory infections in adults, erythromycin is typically prescribed at 500 mg QID (2 g/day), not 250 mg QID (1 g/day).
- ❌ Drug choice is not first-line for COPD exacerbations. GOLD 2025 recommends Amoxicillin-Clavulanate or Azithromycin or Levofloxacin as preferred antibiotics. Erythromycin has high resistance rates among the common COPD pathogens (H. influenzae, S. pneumoniae, M. catarrhalis) and significant GI side effects.
- ❌ Prescription is incomplete — No nebuliser bronchodilators, no oxygen therapy instruction, no route of drug administration specified.
- ❌ Prescription format errors: No patient name/age, no date, no physician signature/registration number, no route (oral/inhaled), no tablet quantity mentioned.
Corrected and Rewritten Prescription:
Name: Mr. ___________ Age: ___ years | Weight: ___ kg | Date: ___________ Diagnosis: Acute Exacerbation of COPD Allergies: NKDARx
Drug Dose Quantity Tab Amoxicillin 500 mg + Potassium Clavulanate 125 mg One tablet to be taken three times a day for 7 days (with food) __(21) Inhalation Salbutamol 2.5 mg/2.5 mL + Ipratropium bromide 0.5 mg/2.5 mL (Nebuliser solution) To be inhaled via nebuliser every 4–6 hours __(1) Tab Prednisolone 40 mg One tablet to be taken once a day for 5 days (in the morning, with food) __(5) Additional instructions:
- Oxygen supplementation if SpO₂ < 90% (target 88–92% in COPD)
- Monitor for respiratory failure — escalate to hospital if worsening
Patient Education:
- Take all antibiotics for the full prescribed course
- Do not stop steroids abruptly if on a longer course
- Return immediately if breathlessness worsens, confusion develops, or oxygen is needed
- Smoking cessation counselling
Alternate Antimicrobials: Azithromycin 500 mg OD × 5 days; Levofloxacin 500 mg OD × 5 days Alternate Bronchodilator: Deriphylline (Etophylline + Theophylline) — if nebuliser unavailableDr. ___________ | Reg. No. ___________ | Signature: ___________
Summary Table of Errors and Corrections:
| Drug | Original Error | Correction |
|---|---|---|
| Prednisolone | 5 mg (too low), 10 days (too long) | 40 mg once daily × 5 days |
| Theophylline | Not recommended in acute COPD exacerbation; toxic | Remove — replace with nebulised Salbutamol + Ipratropium |
| Erythromycin | Subtherapeutic dose (250 mg QID), poor first-line choice | Replace with Amoxicillin-Clavulanate 625 mg TDS × 7 days |
| Missing | No bronchodilators, no oxygen guidance, no format | Added nebulised SABA + SAMA, oxygen instruction, proper Rx format |
what about image prescription
prescription writing format components date patient name drug dose route frequency duration signature
asthma COPD inhaler prescription format sample
A formal handwritten-style medical prescription pad image for seasonal asthma in an adult. The prescription should look like a real doctor's prescription slip with the following details clearly printed: Header: Hospital/Clinic Name, Doctor's name, Qualification, Registration Number, Address, Date Patient section: Name: Mr. XYZ, Age: 30 years, Date: ___ Rx symbol prominently displayed Drug: Inhalation Salbutamol 100 mcg/puff (MDI) — 1-2 puffs to be inhaled as and when required (PRN), not more than 4 times a day — Quantity: 1 MDI Direction: Shake well before use. Inhale 1-2 puffs during breathlessness or 15 min before allergen exposure. Rinse mouth after use. Patient Education: Avoid seasonal allergens, correct MDI technique, seek review if using more than twice a week. Alternate Drug: Terbutaline inhaler Doctor Signature and Registration Number at bottom Clean white background, professional medical format, clear black text, neat layout
A formal medical prescription pad image for Chronic Obstructive Pulmonary Disease (COPD) in an adult patient. The prescription should look like a real doctor's prescription slip with clearly printed professional medical format. Header: Hospital/Clinic Name, Doctor's Name, MBBS MD, Registration No., Address, Date Patient: Name: Mr. XYZ, Age: 55 years, Diagnosis: COPD Rx symbol prominently Three drugs listed in a neat table format: 1. Inhalation Tiotropium 9 mcg/puff (MDI) — 1 puff once daily every morning — Qty: 1 MDI 2. Inhalation Formoterol 6 mcg/puff (MDI) — 1 puff twice daily morning and evening — Qty: 1 MDI 3. Inhalation Salbutamol 100 mcg/puff (MDI) — 1-2 puffs as and when required (rescue) — Qty: 1 MDI Directions for each drug clearly written below each entry. Patient Education section: Stop smoking, correct inhaler technique, pulmonary rehabilitation, annual flu vaccine, avoid irritants. Alternate Drugs: Glycopyrronium, Salmeterol, add ICS if frequent exacerbations. Doctor Signature and stamp at bottom. Clean white background, professional layout, black text.
A formal medical prescription pad image showing a CORRECTED prescription for Acute Exacerbation of COPD in an adult patient. The image should have two sections side by side or one below the other: LEFT SECTION - ORIGINAL INCORRECT PRESCRIPTION (with red cross marks or strikethrough showing errors): Title: "ORIGINAL PRESCRIPTION (INCORRECT)" - Tab Prednisolone 5mg — 10 days ❌ (too low dose, too long) - Tab Theophylline 400mg BD — 10 days ❌ (not recommended) - Tab Erythromycin 250mg QID — 10 days ❌ (wrong drug, wrong dose) RIGHT SECTION - CORRECTED PRESCRIPTION (with green checkmarks): Title: "CORRECTED PRESCRIPTION" Header: Doctor Name, MBBS MD, Reg. No., Date Patient: Mr. XYZ, Age: 55 years, Diagnosis: Acute Exacerbation of COPD Rx symbol 1. Tab Amoxicillin 500mg + Potassium Clavulanate 125mg — One tablet three times a day for 7 days — Qty: 21 2. Inhalation Salbutamol 2.5mg + Ipratropium 0.5mg (Nebuliser) — Every 4-6 hours via nebuliser — Qty: 1 3. Tab Prednisolone 40mg — One tablet once daily for 5 days (morning with food) — Qty: 5 Patient Education: Complete antibiotic course, do not stop steroids abruptly, return if worsening, stop smoking. Alternate drugs: Azithromycin 500mg OD x5 days, Levofloxacin 500mg OD x5 days. Doctor Signature. Professional medical format, clean white background, clear text.
A) Prescription Image — Seasonal Asthma (Single Drug)
B) Prescription Image — COPD Drug Therapy
C) Corrected Prescription — Acute Exacerbation of COPD (Written Format)
╔══════════════════════════════════════════════════════════════╗
║ DR. [NAME] MBBS, MD (Pharmacology) ║
║ Reg. No.: ___________ ║
║ City Hospital, [Address] Date: __________ ║
╠══════════════════════════════════════════════════════════════╣
║ Patient: Mr. XYZ Age: 55 yrs Sex: Male ║
║ Diagnosis: Acute Exacerbation of COPD ║
╠══════════════════════════════════════════════════════════════╣
║ Rx ║
║ ║
║ 1. Tab Amoxicillin 500 mg + (21) ║
║ Potassium Clavulanate 125 mg ║
║ Direction: One tablet three times a day ║
║ for 7 days (with food) ║
║ ║
║ 2. Inhal. Salbutamol 2.5 mg + (1) ║
║ Ipratropium 0.5 mg (Nebuliser solution) ║
║ Direction: To be inhaled via nebuliser ║
║ every 4–6 hours ║
║ ║
║ 3. Tab Prednisolone 40 mg (5) ║
║ Direction: One tablet once daily ║
║ for 5 days (morning, with food) ║
║ ║
║ Alternate: Azithromycin 500 mg OD × 5 days ║
╠══════════════════════════════════════════════════════════════╣
║ Patient Education: ║
║ • Complete full antibiotic course ║
║ • Do not stop steroids abruptly ║
║ • Return if breathlessness worsens ║
║ • Stop smoking immediately ║
╠══════════════════════════════════════════════════════════════╣
║ Dr. [Signature] ║
║ Reg. No.: ___________ ║
╚══════════════════════════════════════════════════════════════╝
What Was Wrong in the Original (Quick Visual Summary):
| ❌ Original | Error | ✅ Corrected |
|---|---|---|
| Prednisolone 5 mg × 10 days | Dose 8× too low; duration too long | 40 mg × 5 days |
| Theophylline 400 mg BD | Not recommended in acute COPD exacerbation | Removed → Nebulised Salbutamol + Ipratropium |
| Erythromycin 250 mg QID | Subtherapeutic dose; wrong drug choice | Amoxicillin-Clavulanate 625 mg TDS × 7 days |
| No bronchodilators | Most critical acute treatment missing | Added nebulised SABA + SAMA |
| No Rx format | No name, date, sig, quantity, route | Full format added |
1. Allergic Rhinitis Rx Tablet Levocetirizine10 mg (7) Direction: One tablet to be taken once a day for seven days. Saline nasal drops (1 bottle) Direction: 1-2 drops to be instilled in each nostril 2-3 times a day Xylometazoline 0.05% Nasal drops (1 bottle) Direction: 1-2 drops to be instilled in each nostril 3-4 times a day. Patient education: • Saline gargles and steam inhalation Alternate drugs: • Chlorpheniramine, fexofenadine 2. Dry cough Rx Lozenges Dextromethorphan 5 mg (9) Direction: To be taken three times a day. Alternate drugs: • Codeine phosphate 3. Acute otitis media Rx Capsule Amoxicillin 500 mg+ Potassium clavulanate 125 mg (21) Direction: One capsule to be taken three times a day for seven days. Tablet Levocetirizine10mg (7) Direction: One tablet to be taken once a day for seven days. Tablet Paracetamol 500 mg (28) Direction: One tablet to be taken four times a day for seven days. Alternate drugs: • Azithromycin, ciprofloxacin is this correct ?
allergic rhinitis treatment levocetirizine xylometazoline nasal drops prescription guidelines
dry cough antitussive dextromethorphan codeine lozenges dose treatment
acute otitis media antibiotic treatment amoxicillin clavulanate paracetamol prescription
Prescription Review: Allergic Rhinitis, Dry Cough & Acute Otitis Media
1. Allergic Rhinitis
✅ What is Correct:
| Item | Verdict |
|---|---|
| Levocetirizine 10 mg OD × 7 days | ✅ Correct drug, correct dose, correct frequency and duration |
| Saline nasal drops 1–2 drops each nostril 2–3×/day | ✅ Correct — safe, non-pharmacological adjunct |
| Xylometazoline 0.05% nasal drops | ✅ Correct concentration for adults (0.1% is also acceptable for adults; 0.05% is safer) |
| Xylometazoline direction 3–4×/day | ✅ Acceptable |
| Quantity: Levocetirizine (7), Saline (1 bottle), Xylometazoline (1 bottle) | ✅ Correct |
| Alternate drugs: Chlorpheniramine, Fexofenadine | ✅ Both are valid antihistamine alternatives |
❌ Errors Found:
- Xylometazoline is a decongestant nasal drop. It must NOT be used for more than 3–5 consecutive days — prolonged use causes rhinitis medicamentosa (rebound nasal congestion). The prescription does not state a limit.
- Correction: Add — "Not to be used for more than 3–5 days continuously."
- For moderate-to-severe or persistent allergic rhinitis, an intranasal corticosteroid (e.g., Mometasone/Fluticasone nasal spray) is the first-line drug per ARIA guidelines. If this is mild intermittent rhinitis, the prescription is acceptable; otherwise an INCS should be added.
- "Saline gargles and steam inhalation" is listed under patient education — this is more relevant for upper respiratory tract infection, not specifically for allergic rhinitis.
- More appropriate education: avoid allergens (dust, pollen, pet dander), avoid rubbing eyes/nose, use air purifiers.
Corrected Prescription 1:
Rx
Tablet Levocetirizine 10 mg (7)
Direction: One tablet to be taken once a day for seven days.
Saline Nasal Drops (1 bottle)
Direction: 1–2 drops to be instilled in each nostril 2–3 times a day.
Xylometazoline 0.05% Nasal Drops (1 bottle)
Direction: 1–2 drops to be instilled in each nostril 3–4 times a day.
⚠ Do NOT use for more than 3–5 days continuously.
Patient Education:
• Avoid known allergens (pollen, dust, pet dander)
• Do not rub eyes or nose
• Steam inhalation for symptomatic relief
• Seek review if symptoms persist beyond 7 days
Alternate drugs: Chlorpheniramine, Fexofenadine
2. Dry Cough
✅ What is Correct:
| Item | Verdict |
|---|---|
| Dextromethorphan as antitussive | ✅ Correct drug class — centrally acting non-narcotic antitussive (Harrison's, p. 1127) |
| Frequency: Three times a day | ✅ Acceptable |
| Alternate: Codeine phosphate | ✅ Correct — narcotic antitussive, more potent but with more side effects |
❌ Errors Found:
- Standard adult dose of Dextromethorphan lozenges/tablets is 10–20 mg every 4–6 hours, not 5 mg.
- 5 mg is a pediatric/low dose. For an adult, this will have minimal to no antitussive effect.
- Correction: Dextromethorphan 15 mg (lozenge) three times a day.
- The prescription does not specify how many days to take the lozenges. Duration should be stated (typically 3–5 days for dry cough).
- Correction: Add "for 3–5 days or until cough resolves."
- If TDS × 5 days = 15 lozenges needed. 9 lozenges only covers 3 days at TDS — duration mismatch.
- Correction: Quantity should be (15) for 5 days TDS.
- Dry cough is a symptom, not a diagnosis. The prescription should ideally note the underlying cause (post-viral, ACE inhibitor-induced, etc.) and treat accordingly.
Corrected Prescription 2:
Rx
Lozenges Dextromethorphan 15 mg (15)
Direction: One lozenge to be taken three times a day
for five days or until cough resolves.
Patient Education:
• Avoid cold air, smoke, and irritants
• Stay well hydrated
• Seek review if cough persists beyond 2 weeks or blood is noticed
Alternate drugs: Codeine phosphate (narcotic — use only if refractory)
3. Acute Otitis Media
✅ What is Correct:
| Item | Verdict |
|---|---|
| Amoxicillin 500 mg + Clavulanate 125 mg TDS × 7 days | ✅ Correct first-line antibiotic, correct dose, frequency, and duration |
| Quantity (21) for antibiotic | ✅ Correct (TDS × 7 days = 21 capsules) |
| Paracetamol 500 mg QID × 7 days for pain | ✅ Correct — acetaminophen/paracetamol is recommended for pain in AOM (Harrison's, p. 1058) |
| Paracetamol quantity (28) | ✅ Correct (QID × 7 = 28 tablets) |
| Alternate drugs: Azithromycin, Ciprofloxacin | ✅ Azithromycin is an acceptable alternate |
❌ Errors Found:
- Levocetirizine is an antihistamine. There is no evidence that antihistamines help in AOM. AOM is caused by bacterial infection (S. pneumoniae, H. influenzae) — it is NOT an allergic condition.
- The inclusion of levocetirizine here is irrational and incorrect.
- Correction: Remove levocetirizine entirely from this prescription.
- Ciprofloxacin (a fluoroquinolone) has poor coverage against Streptococcus pneumoniae, the most common AOM pathogen. It is not a preferred alternate for AOM.
- Better alternate: Azithromycin (acceptable) or Co-trimoxazole.
- For symptomatic relief of ear pain, topical analgesic ear drops (e.g., Benzocaine ear drops) can be added as adjunct therapy per Harrison's (p. 1058).
- Paracetamol 500 mg QID (2 g/day) is on the lower end for adults. Standard adult dosing is 500–1000 mg every 4–6 hours (max 4 g/day). Consider 1000 mg (two 500 mg tablets) TDS for better analgesic effect, or at minimum document the dose clearly.
Corrected Prescription 3:
Rx
Capsule Amoxicillin 500 mg + Potassium Clavulanate 125 mg (21)
Direction: One capsule to be taken three times a day
for seven days (with food).
Tablet Paracetamol 500 mg (28)
Direction: One to two tablets to be taken four times a day
for seven days (for pain/fever relief).
Patient Education:
• Complete the full antibiotic course even if feeling better
• Apply warm compress over affected ear for pain relief
• Do not insert anything into the ear canal
• Seek review if symptoms worsen or fever persists beyond 48 hours
Alternate drugs: Azithromycin, Co-trimoxazole
Overall Summary Table
| Prescription | Major Errors | Verdict |
|---|---|---|
| Allergic Rhinitis | Xylometazoline duration limit missing; patient education not specific | ⚠ Mostly correct, minor corrections needed |
| Dry Cough | Dose too low (5 mg → should be 15 mg); duration missing; quantity insufficient | ❌ Needs correction |
| Acute Otitis Media | Levocetirizine is irrational here; Ciprofloxacin is poor alternate for AOM | ❌ Needs correction (remove levocetirizine) |
latest GINA guidline in india
GINA 2024 guidelines asthma diagnosis management stepwise treatment
GINA guidelines India asthma inhaler ICS LABA SABA preferred controller treatment steps
GINA 2024 track 1 track 2 asthma step 1 2 3 4 5 budesonide formoterol SMART therapy
GINA asthma step 3 step 4 step 5 biologics low dose ICS LABA severe asthma omalizumab
GINA 2023 2024 asthma diagnosis spirometry symptoms classification severity adults
GINA step 1 step 2 low dose ICS as needed reliever SABA no longer recommended
GINA 2024 Guidelines — Asthma Management (India Context)
GINA = Global Initiative for Asthma — updated annually. The 2024 report is the current version. India follows GINA guidelines as the primary framework, with adaptations for drug availability and affordability.
🔑 The Biggest Change in Recent GINA (2021 onwards, retained in 2024)
SABA-only therapy is NO longer recommended at any step.
GINA 2024 — Two Treatment Tracks
| Track 1 (Preferred) | Track 2 (Alternative) | |
|---|---|---|
| Reliever | Low-dose ICS-Formoterol as needed | SABA as needed |
| Controller | ICS-Formoterol (SMART) | Regular ICS or ICS-LABA |
| Preferred? | ✅ YES — GINA preferred track | ✅ Acceptable where Track 1 unavailable |
| India relevance | Growing availability; preferred | Widely available; commonly used |
GINA 2024 — Step-by-Step Treatment (Adults ≥12 years)
TRACK 1 — Preferred (ICS-Formoterol based)
| Step | Severity | Preferred Controller | Preferred Reliever |
|---|---|---|---|
| Step 1 | Mild intermittent | None needed as regular controller | Low-dose ICS-Formoterol as needed (PRN) |
| Step 2 | Mild persistent | Low-dose ICS-Formoterol daily | Low-dose ICS-Formoterol PRN |
| Step 3 | Moderate persistent | Low-dose ICS-Formoterol daily (SMART) | ICS-Formoterol PRN |
| Step 4 | Moderate-severe persistent | Medium-dose ICS-Formoterol daily (SMART) | ICS-Formoterol PRN |
| Step 5 | Severe uncontrolled | High-dose ICS-LABA + add-on biologics (Omalizumab, Mepolizumab) | ICS-Formoterol PRN |
SMART = Single Maintenance And Reliever Therapy — Budesonide/Formoterol inhaler used as BOTH controller (daily) AND reliever (as needed). Supported by Harrison's (p. 7937) and Asthma Management Guidelines (p. 81, 84).
TRACK 2 — Alternative (SABA-based reliever)
| Step | Preferred Controller | Reliever |
|---|---|---|
| Step 1 | Low-dose ICS taken whenever SABA is taken | SABA PRN |
| Step 2 | Low-dose ICS daily | SABA PRN |
| Step 3 | Low-dose ICS-LABA daily | SABA PRN |
| Step 4 | Medium-dose ICS-LABA daily | SABA PRN |
| Step 5 | High-dose ICS-LABA + tiotropium/biologics | SABA PRN |
Drugs Commonly Used in India (GINA-aligned)
| Drug Class | Generic Name | Brand (India) | Step Used |
|---|---|---|---|
| ICS | Budesonide | Budecort, Pulmicort | Steps 1–5 |
| ICS | Beclomethasone | Beclate | Steps 2–4 |
| ICS | Fluticasone | Flohale | Steps 2–5 |
| LABA | Formoterol | Foradil | Steps 3–5 |
| LABA | Salmeterol | Serevent | Steps 3–5 |
| ICS + LABA (SMART) | Budesonide + Formoterol | Foracort, Symbicort | Steps 1–5 (preferred) |
| ICS + LABA | Fluticasone + Salmeterol | Seroflo | Steps 3–5 |
| SABA (rescue) | Salbutamol | Asthalin | Reliever (Track 2) |
| LAMA (add-on) | Tiotropium | Tiova | Step 4–5 add-on |
| Anti-IgE biologic | Omalizumab | Xolair | Step 5 |
| Anti-IL5 biologic | Mepolizumab | Nucala | Step 5 |
| OCS (short course) | Prednisolone | Wysolone | Exacerbations |
ICS Dose Table (GINA 2024 — Adults)
| ICS Drug | Low Dose | Medium Dose | High Dose |
|---|---|---|---|
| Budesonide MDI | 200–400 mcg/day | 400–800 mcg/day | >800 mcg/day |
| Beclomethasone | 200–500 mcg/day | 500–1000 mcg/day | >1000 mcg/day |
| Fluticasone propionate | 100–250 mcg/day | 250–500 mcg/day | >500 mcg/day |
| Budesonide/Formoterol | 200/6 mcg × 1–2 puffs/day | 200/6 mcg × 2 puffs BD | 400/12 mcg BD |
GINA 2024 — Key Principles Relevant to India
1. Confirm Diagnosis Before Treating
- Spirometry (FEV₁/FVC < 0.7 + reversibility ≥12% with bronchodilator) confirms asthma
- Many Indian patients are treated empirically — GINA 2024 emphasizes objective confirmation
2. Assess & Treat Comorbidities
- Allergic rhinitis, GERD, obesity, smoking — all worsen asthma control
- Treat these alongside asthma
3. Inhaler Technique is Critical
- Poor inhaler technique is a major cause of uncontrolled asthma in India
- Always demonstrate and verify MDI/DPI technique at every visit
4. Step Down When Controlled
- After 3 months of good control → consider stepping down to the lowest effective dose
- Do not over-treat
5. Severe Asthma & Biologics in India
- Omalizumab (anti-IgE) — available in India; expensive; for allergic severe asthma
- Mepolizumab, Benralizumab — available for eosinophilic severe asthma
- Tezepelumab — newest biologic (TSLP blocker); limited availability in India currently
Asthma vs. COPD vs. Asthma-COPD Overlap (ACO) — India
| Feature | Asthma | COPD | ACO |
|---|---|---|---|
| Age of onset | Usually < 40 years | Usually > 40 years | Variable |
| Smoking | Not required | Usually present | Often present |
| Spirometry reversibility | Yes (≥12%) | Incomplete | Partial |
| Eosinophils | Often elevated | Variable | Often elevated |
| Treatment | ICS + LABA (GINA) | LAMA + LABA (GOLD) | ICS + LAMA + LABA |
Non-Pharmacological Management (GINA 2024)
- Smoking cessation — single most important intervention
- Allergen avoidance — dust mites, pollen, cockroach, mold (highly relevant in India)
- Exercise — encouraged; use reliever 15 min before exercise if needed
- Weight reduction in obese patients
- Vaccinations — annual influenza, pneumococcal
- Avoid NSAIDs/Aspirin in aspirin-exacerbated respiratory disease (AERD)
- Written Asthma Action Plan — give every patient a personalized plan
Summary: Old vs. New GINA (Most Important Change for Exams)
| Aspect | Old GINA (before 2021) | GINA 2024 |
|---|---|---|
| Step 1 reliever | SABA alone (Salbutamol) | Low-dose ICS-Formoterol PRN |
| Step 2 controller | Low-dose ICS daily | Low-dose ICS daily or ICS-Formoterol PRN |
| SMART therapy | Step 3 onwards | All steps (1–4) |
| SABA monotherapy | Acceptable at Step 1 | No longer recommended at any step |
| Biologic therapy | Limited | Expanded (anti-IL4, anti-TSLP added) |