Dka aout protocol
Reading File
search_medical_text
DKA diabetic ketoacidosis protocol diagnosis management treatment
search_medical_image
DKA diabetic ketoacidosis management protocol flowchart
GradeResponse
GradeResponse
Assuming you mean DKA protocol (diabetic ketoacidosis), here is a concise adult ER/ICU protocol.
1) Confirm DKA
Diagnosis is typically:
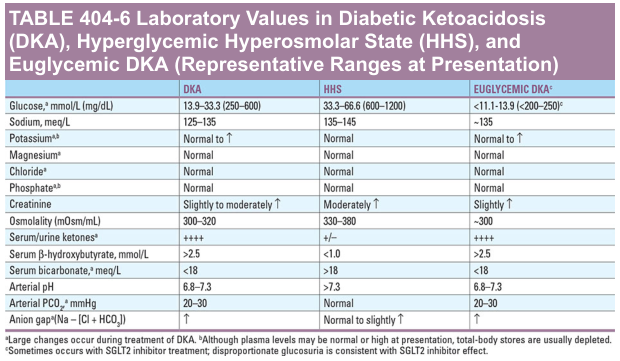
- Glucose >250 mg/dL (can be lower in euglycemic DKA)
- Metabolic acidosis: pH <7.30 and/or HCO3 ≤18 mEq/L
- Ketosis: elevated serum beta-hydroxybutyrate or urine ketones
- Usually elevated anion gap
Harrison’s lists representative DKA labs including glucose 250 to 600 mg/dL and typical electrolyte patterns (Harrison’s, p. 11343).
2) Immediate first hour
- ABCs, monitor, IV access, cardiac monitor
- Labs: BMP, venous/arterial blood gas, ketones, CBC, osmolality, Mg, phosphate, ECG, infection workup if indicated
- Start fluids:
- 0.9% saline 15 to 20 mL/kg in first hour (about 1 to 1.5 L in most adults)
3) Potassium-guided insulin start
- K <3.3 mEq/L: hold insulin, give K first (usually 20 to 30 mEq/h) until >3.3
- K 3.3 to 5.2: start insulin + add K to IV fluids (20 to 30 mEq per liter)
- K >5.2: start insulin, no K initially, recheck frequently
4) Insulin therapy
- Regular insulin IV:
- 0.1 U/kg bolus then 0.1 U/kg/h, or
- 0.14 U/kg/h without bolus
- Goal glucose drop: about 50 to 75 mg/dL per hour
5) Ongoing fluids and dextrose transition
- After first hour, choose fluid by corrected sodium:
- low Na: continue 0.9% saline
- normal/high Na: 0.45% saline
- When glucose reaches ~200 mg/dL (DKA), add D5-containing fluid and reduce insulin rate (often 0.02 to 0.05 U/kg/h) to continue clearing ketones and closing anion gap.
6) Bicarbonate and phosphate
- Bicarbonate: generally avoid unless severe acidemia (commonly pH <6.9)
- Phosphate: not routine; replace if severe hypophosphatemia, cardiac dysfunction, respiratory weakness, or other specific indications
7) Monitoring
- Hourly bedside glucose
- Electrolytes, anion gap, bicarbonate, creatinine every 2 to 4 hours
- Strict input/output, mental status, vitals
- Search and treat precipitating cause (infection, missed insulin, MI, stroke, pancreatitis, drugs). Harrison’s emphasizes identifying and treating triggers and close reassessment (p. 11347).
8) Resolution criteria (typical)
DKA resolved when:
- glucose <200 mg/dL and
- two of:
- bicarbonate ≥15 mEq/L
- pH >7.30
- anion gap normalized
9) Transition IV to subcutaneous insulin
- Give long-acting basal insulin
- Overlap IV insulin for 1 to 2 hours after first SC dose to prevent rebound ketosis
- Ensure patient can eat and cause is addressed
Useful reference image
If you want, I can give this as a one-page bedside order set (fluids, insulin, potassium, and lab timing) for quick use in adults, or a pediatric-specific protocol (which differs).
This is a shared conversation. Sign in to Orris to start your own chat.