HellCan you tell me about lung cancer
Reading File
Searching the Web
lung cancer types diagnosis treatment 2025
Finding Sources
Searching PubMed
"lung cancer"[MeSH Terms] AND "treatment"[MeSH Terms]
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information from multiple authoritative textbooks. Let me compile a thorough response.
Lung Cancer - A Comprehensive Overview
Epidemiology & Burden
Lung cancer is one of the most common cancers worldwide and the leading cause of cancer death. In the UK alone, approximately 45,000 new cases are diagnosed per year. The prognosis remains poor: 60% of patients die within 1 year of diagnosis, and only 15% survive to 5 years. Survival depends heavily on the stage at presentation. - Bailey and Love's Short Practice of Surgery, 28th Ed.
Risk Factors
- Cigarette smoking is the dominant risk factor, accounting for 85-95% of all cases
- Atmospheric/environmental pollution
- Occupational exposures: mining of radioactive ores, chromium compounds
- Radon gas exposure
- Never-smokers can also develop lung cancer (more often adenocarcinoma), though late diagnosis is more common due to lower clinical suspicion
Classification
Lung cancers are divided into two major groups in a 1:4 ratio:
1. Small Cell Lung Cancer (SCLC) - ~20%
- Previously called "oat cell" carcinoma due to the packed appearance of small dense cells
- A type of neuroendocrine tumour (NET)
- Tendency to metastasize early - to lymph nodes and via haematogenous spread
- Median survival measured in months
- Very chemotherapy-responsive (survival may double, but cure is rare)
- Surgery rarely offered except in very limited-stage disease
2. Non-Small Cell Lung Cancer (NSCLC) - ~80%
| Subtype | Features |
|---|---|
| Adenocarcinoma | Now the most common NSCLC subtype; rising incidence in women; common in never-smokers; associated with deeper inhalation of lower-tar cigarettes |
| Squamous cell carcinoma | Typically central; often presents as a cavitating tumour |
| Large cell undifferentiated | Discrete histological type; classified within NETs |
- Bailey and Love's Short Practice of Surgery, 28th Ed.
Symptoms & Clinical Presentation
Lung cancer has one of the most diverse presentation patterns of any malignancy - Schwartz's Principles of Surgery, 11th Ed.
Pulmonary Symptoms (in order of frequency)
| Symptom | Mechanism |
|---|---|
| Cough | Bronchus irritation or compression |
| Dyspnea | Central airway obstruction or atelectasis |
| Wheezing | >50% airway obstruction |
| Hemoptysis | Tumor erosion or irritation (central location) |
| Pneumonia/Lung abscess | Airway obstruction, necrosis, cavitation |
Nonpulmonary Thoracic Symptoms
| Symptom | Mechanism |
|---|---|
| Pleuritic pain | Parietal pleural irritation or invasion |
| Chest wall/radicular pain | Rib, muscle, intercostal nerve involvement |
| Pancoast's syndrome | Superior sulcus tumour invading stellate ganglion, brachial plexus (causes ipsilateral Horner's syndrome + arm pain) |
| SVC obstruction | Compression/invasion of superior vena cava |
| Hoarseness | Recurrent laryngeal nerve involvement |
Paraneoplastic Syndromes
Paraneoplastic manifestations may present before local symptoms, aiding early diagnosis. They often resolve with successful treatment and recur with disease progression.
Imaging
Chest X-Ray (CXR):
Below is a CXR from Bailey & Love's showing a large mass in the right upper lobe causing Horner's syndrome - a classic Pancoast tumour:
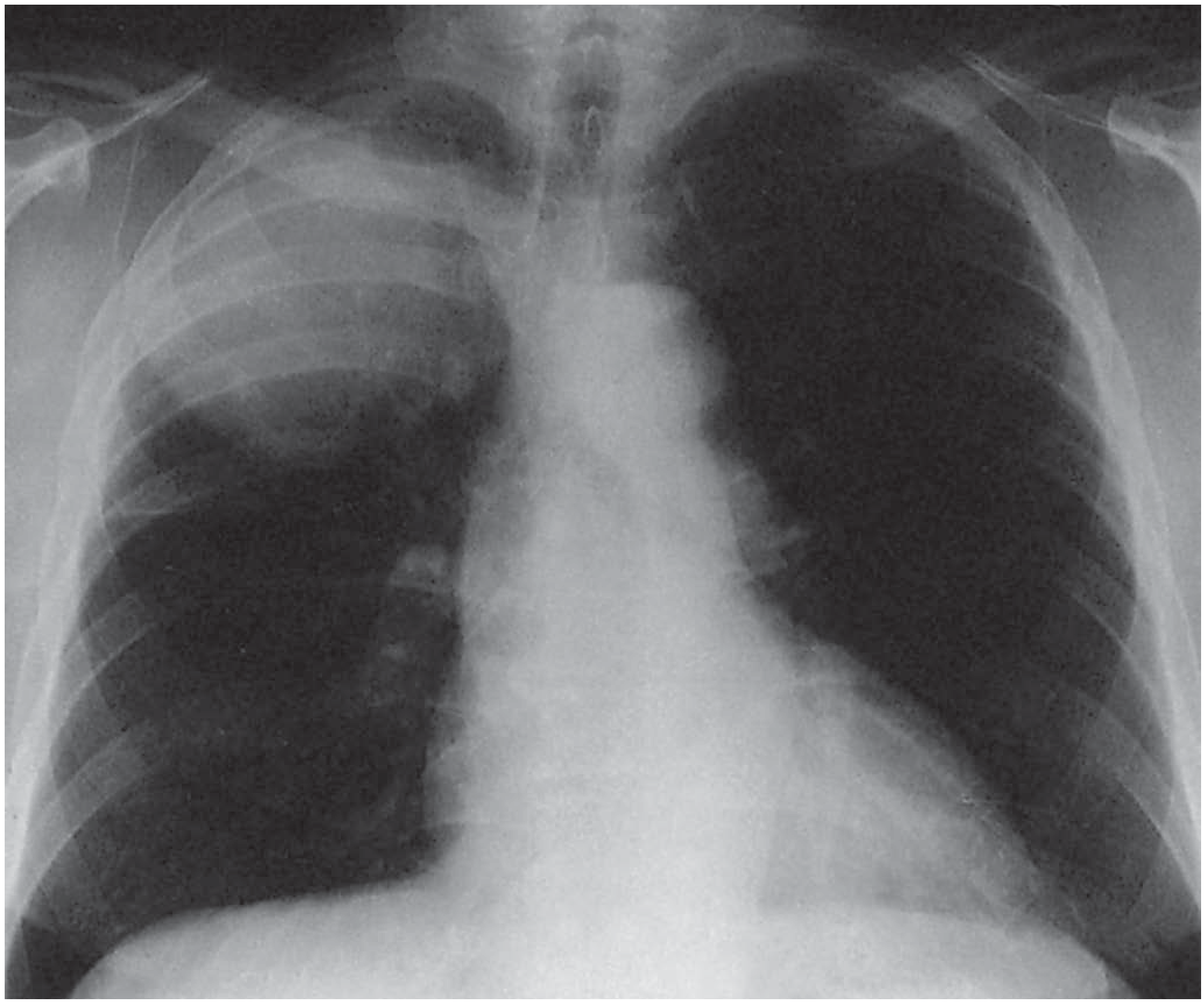
Figure: Chest radiograph of carcinoma of the lung - large right upper lobe mass causing Horner's syndrome (Pancoast tumour). - Bailey and Love's Short Practice of Surgery, 28th Ed.
CT Scan: Contrast-enhanced CT chest is standard, demonstrating the primary tumour and mediastinal lymphadenopathy.
PET-CT (FDG-PET): High FDG avidity associated with lung cancers. Detects metastatic disease and guides staging. Important to note that infection/inflammation can also be FDG-avid (false positives).
Diagnosis & Staging Workup
Non-invasive
- CXR, CT chest/abdomen/pelvis
- PET-CT scan
- Sputum cytology (high false-negative rate)
Invasive
- Flexible bronchoscopy: cytological brushing/washing, TBNA - for centrally placed tumours
- Endobronchial ultrasound (EBUS): ultrasound-guided TBNA of mediastinal lymph nodes
- Endoscopic ultrasound (EUS): FNA of mediastinal nodes via oesophagus
- Navigational bronchoscopy: 3D virtual map for targeting peripheral lesions
- CT-guided percutaneous biopsy: for peripheral lesions
Molecular/Biomarker Testing
Histologic and molecular diagnosis is now critical before starting treatment:
- All adenocarcinoma specimens should be tested for: EGFR, KRAS, ALK, ROS1, BRAF, HER2, MET, RET
- Differentiation between adenocarcinoma and squamous cell carcinoma matters because:
- Pemetrexed and bevacizumab are effective in adenocarcinoma but NOT squamous cell
- Bevacizumab carries risk of life-threatening hemorrhage in squamous cell carcinoma
- EGFR mutation predicts response to EGFR tyrosine kinase inhibitors (TKIs) - now recommended first-line in advanced adenocarcinoma
- PD-L1 expression testing guides immunotherapy eligibility
TNM Staging (8th Edition)
Stage I NSCLC:
- Stage IA: T1a-cN0M0 (tumour ≤3 cm)
- Stage IB: T2aN0M0 (3-4 cm tumour)
- Only 16% of NSCLC patients present at Stage I
Treatment
NSCLC - By Stage
| Stage | Primary Treatment | Notes |
|---|---|---|
| IA & IB | Surgery (lobectomy) | Adjuvant chemo for tumours ≥4 cm or high-risk features (vascular invasion, visceral pleural involvement) |
| IIA & IIB | Surgery + adjuvant chemotherapy | ~5% improvement in 5-year survival with adjuvant chemo |
| III (locally advanced) | Concurrent chemoradiotherapy ± immunotherapy | Unresectable disease; durvalumab consolidation after CRT |
| IV (metastatic) | Chemotherapy, targeted therapy, immunotherapy | Biomarker-driven selection; palliative care offered from diagnosis |
- Murray & Nadel's Textbook of Respiratory Medicine
Medically Inoperable Stage I NSCLC
Stereotactic Body Radiation Therapy (SBRT) is an effective alternative to surgery.
Stage IV / Advanced NSCLC - Treatment Drivers
Targeted therapy (if driver mutation present):
- EGFR mutation (exon 19 del/L858R): EGFR-TKIs (erlotinib, gefitinib, osimertinib) as first-line; 5-year survival improved from ~4% (pre-TKI era) to ~14.6%
- ALK fusion: ALK inhibitors (crizotinib, alectinib)
- ROS1 rearrangement: ROS1 inhibitors
- BRAF V600E: dabrafenib + trametinib
- MET exon 14 skip / MET amplification: capmatinib, tepotinib
Immunotherapy (if no driver mutation):
- PD-1/PD-L1 checkpoint inhibitors (pembrolizumab, nivolumab, atezolizumab)
- High PD-L1 expression (≥50%) predicts strongest response
- Pembrolizumab monotherapy is first-line standard if PD-L1 ≥50% with no targetable mutation
Chemotherapy:
- Platinum-based doublets (carboplatin/cisplatin + paclitaxel, gemcitabine, pemetrexed) remain the backbone for those without targetable mutations
SCLC Treatment
- Extensive stage: platinum-based chemotherapy (etoposide + cisplatin/carboplatin) + immunotherapy (atezolizumab or durvalumab)
- Surgery rarely offered
- Prophylactic cranial irradiation (PCI) considered in responding limited-stage SCLC
Prognosis
| Stage | Approximate 5-Year Survival (NSCLC) |
|---|---|
| Stage I | 60-80% |
| Stage II | 30-55% |
| Stage III | 10-35% |
| Stage IV | ~5-15% (improving with targeted/immunotherapy) |
Overall survival across all stages is ~15-20% at 5 years. Targeted therapy in EGFR-mutant advanced disease has significantly improved outcomes in that subset.
Recent Advances (2025-2026)
Per MSKCC reporting and the 2025 NSCLC management update in PMC, the most significant recent developments include:
- Perioperative immunotherapy (pembrolizumab - KEYNOTE-671; durvalumab - AEGEAN) for resectable Stage II-IIIB NSCLC, improving event-free survival
- Expansion of post-operative adjuvant targeted therapy (osimertinib for EGFR-mutant resected NSCLC)
- Growing role of next-generation sequencing (NGS) panels to identify rare actionable mutations
- Liquid biopsy (ctDNA) for minimal residual disease monitoring
Sources: Bailey and Love's Short Practice of Surgery 28th Ed. | Schwartz's Principles of Surgery 11th Ed. | Murray & Nadel's Textbook of Respiratory Medicine | Tietz Textbook of Laboratory Medicine 7th Ed. | Harrison's Principles of Internal Medicine 22nd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.