Differential diagnosis and approach to post menopausal bleeding
Reading File
search_medical_text
postmenopausal bleeding differential diagnosis causes etiology
search_medical_text
postmenopausal bleeding investigation workup management endometrial biopsy ultrasound
search_medical_image
postmenopausal bleeding algorithm approach transvaginal ultrasound endometrial thickness
GradeResponse
GradeResponse
GradeResponse
Postmenopausal Bleeding (PMB): Differential Diagnosis & Approach
Definition: Any vaginal bleeding occurring >12 months after the last menstrual period in a woman not on hormone therapy (or unexpected/unscheduled bleeding on HRT). PMB is a red flag symptom until proven otherwise — ~10% harbor endometrial malignancy.
Differential Diagnosis
PMB can originate from the genital tract or be non-gynaecological. The most useful mnemonic framework organizes by anatomical site:
A. Uterine / Endometrial (most common)
| Cause | Notes |
|---|---|
| Endometrial atrophy | Most common overall (~60–80%). Thin, fragile epithelium bleeds with minimal trauma. |
| Endometrial polyps | Focal overgrowth; typically benign but can harbour atypia or carcinoma |
| Endometrial hyperplasia | Simple or complex; with/without atypia — the key premalignant lesion |
| Endometrial carcinoma | ~10% of PMB; most important diagnosis to exclude (Harrison's, p. 2692) |
| Uterine sarcoma | Leiomyosarcoma, endometrial stromal sarcoma — rare but aggressive |
| Submucous fibroids | Less common in postmenopausal women; regress after menopause |
B. Cervical
| Cause | Notes |
|---|---|
| Cervical atrophy | Very common; thinned epithelium |
| Cervical polyp | Benign, but can bleed |
| Cervical carcinoma | Must exclude — especially with contact/post-coital bleeding |
| Cervicitis / infection | Atrophic vaginitis with cervical involvement |
C. Vaginal
| Cause | Notes |
|---|---|
| Atrophic vaginitis | Estrogen deficiency → thin, friable mucosa; very common |
| Vaginal carcinoma | Rare primary; more often secondary from cervix/endometrium |
| Trauma | Especially if patient on anticoagulation |
D. Vulval
- Vulval intraepithelial neoplasia (VIN), vulval carcinoma, lichen sclerosus with excoriation
E. Non-gynaecological (often misidentified as vaginal bleeding)
| Source | Cause |
|---|---|
| Urinary | Haematuria from UTI, bladder carcinoma, urethral caruncle |
| Gastrointestinal | Haemorrhoids, colorectal carcinoma, rectal bleeding |
F. Systemic / Iatrogenic
- Hormone replacement therapy (HRT): Unscheduled bleeding in first 3 months may be acceptable; after 3 months warrants investigation
- Tamoxifen use: Stimulates endometrium — significantly increases risk of endometrial hyperplasia and carcinoma
- Anticoagulant therapy: Warfarin, DOACs — may unmask underlying pathology
- Coagulopathy: Rare but consider if no structural cause found
Risk Factors for Endometrial Cancer in PMB
| ↑ Risk | ↓ Risk |
|---|---|
| Obesity (BMI >30) | Combined OCP use |
| Nulliparity | Multiparity |
| Late menopause (>52 yrs) | Progestin use |
| Unopposed oestrogen | Smoking (paradoxically) |
| Tamoxifen use | — |
| PCOS, chronic anovulation | — |
| Hereditary (Lynch syndrome / HNPCC) | — |
| Hypertension, diabetes | — |
| Prior pelvic radiation | — |
Diagnostic Approach
Step 1 — Full History
- Onset, duration, amount, colour of bleeding
- Relationship to coitus (suggests cervical/vaginal source)
- HRT or tamoxifen use
- Smear history, prior gynaecological history
- Family history (Lynch syndrome: endometrial + colorectal cancers)
- Anticoagulant use
Step 2 — Physical Examination
- General: BMI, signs of metabolic syndrome
- Abdominal: Uterine size, adnexal masses, ascites (advanced disease)
- Vulvoscopy / speculum exam: Assess vulva, vagina, cervix for atrophy, polyps, lesions, trauma
- Bimanual exam: Uterine size, mobility, adnexal tenderness/masses
Step 3 — First-Line Investigation: Transvaginal Ultrasound (TVUS)
TVUS is the first-line investigation of choice.
- Endometrial thickness (ET) threshold:
- ≤4 mm: Risk of malignancy <1% → reassure (if no structural abnormality or ongoing bleeding)
- >4 mm or structurally abnormal → proceed to endometrial sampling
- Assess endometrial morphology (homogeneous vs. heterogeneous, fluid in cavity), myometrium, adnexa
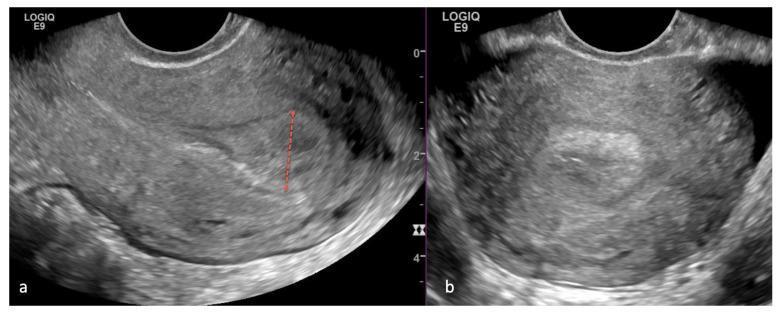
The image below demonstrates classic TVUS findings in PMB due to endometrial carcinoma:
Step 4 — Endometrial Sampling (Biopsy)
Indicated when (Bailey & Love, p. 1606):
- ET >4 mm on TVUS
- Structurally abnormal or persistently thickened endometrium
- Ongoing / recurrent PMB even with ET ≤4 mm
- On tamoxifen or unopposed oestrogen
- Irregular/unscheduled bleeding on HRT beyond initial 3 months
- Strong risk factors: Lynch syndrome family history, PCOS, obesity
Methods:
- Pipelle biopsy (outpatient) — first choice; ~90% sensitivity for endometrial carcinoma
- Hysteroscopy + directed biopsy — gold standard; mandatory if Pipelle is non-diagnostic or focal lesion suspected (polyp)
- D&C — largely replaced by hysteroscopy but used when hysteroscopy unavailable
Step 5 — Further Investigations
| Test | Indication |
|---|---|
| Cervical smear / colposcopy | If cervical lesion seen or smear overdue |
| MRI pelvis | Staging of confirmed endometrial/cervical carcinoma |
| CT chest/abdomen/pelvis | Staging for advanced/high-grade disease |
| Blood tests: FBC, coagulation screen | Anaemia, coagulopathy |
| CA-125 | Not diagnostic, but elevated in advanced endometrial/ovarian disease |
| Saline infusion sonography (SIS) | Delineates intracavitary lesions (polyps) before hysteroscopy |
Summary Algorithm
PMB
│
├─► History + Examination
│ ├─ Obvious vulval/vaginal/cervical cause on speculum?
│ │ └─► Treat accordingly (atrophic vaginitis, polyp removal, refer if malignancy suspected)
│ └─ No obvious cause
│
├─► Transvaginal Ultrasound (TVUS)
│ ├─ ET ≤4 mm, homogeneous, no structural abnormality
│ │ └─► Reassure + follow up (if bleeding recurs → hysteroscopy)
│ └─ ET >4 mm OR heterogeneous / structural abnormality
│ └─► Endometrial biopsy (Pipelle)
│ ├─ Adequate + benign → reassure / treat cause
│ ├─ Hyperplasia with atypia / carcinoma → refer oncology/gynae-oncology
│ └─ Inadequate / inconclusive → Hysteroscopy + directed biopsy
│
└─► If malignancy confirmed → Staging (MRI / CT) → MDT management
Key Points
- Never reassure without investigation — 10% of PMB is endometrial carcinoma
- TVUS ET >4 mm is the standard threshold for proceeding to biopsy in postmenopausal women
- Recurrent PMB with normal TVUS still warrants hysteroscopy — polyps and focal lesions can be missed
- Tamoxifen creates a subendometrial effect that makes TVUS unreliable; direct hysteroscopy/biopsy is preferred
- Lynch syndrome patients require heightened surveillance and counselling for prophylactic surgery
- Atrophic vaginitis/endometrial atrophy is the most common cause, but malignancy must always be excluded first
This is a shared conversation. Sign in to Orris to start your own chat.