Double donut sign
double donut sign radiology imaging
double donut sign imaging finding
Double Donut Sign
1. Intussusception (Most Classic Association)
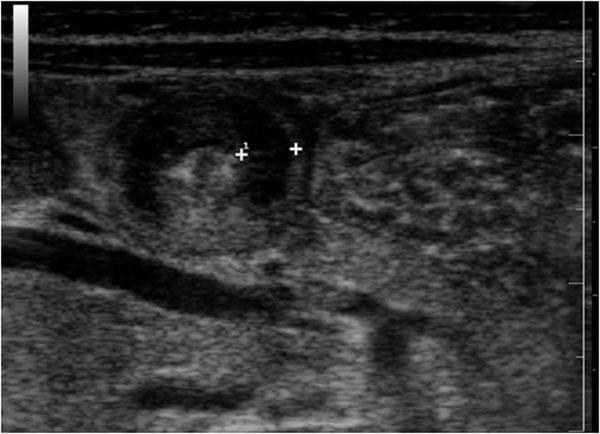
- On cross-section, the intussuscepted bowel produces two concentric hyperechoic rings separated by a hypoechoic layer, creating a "donut within a donut" or "target" appearance
- The outer ring = the intussuscipiens (receiving bowel wall)
- The inner ring = the intussusceptum (invaginated bowel segment)
- The hypoechoic halo between them represents edematous mesentery and bowel wall
- Seen in ileocolic intussusception, the most common type in children (peak age: 3 months – 6 years)
- Ultrasound sensitivity for intussusception is >97% when this sign is present
- Presence of a lead point (e.g., Meckel's diverticulum, lymphoma, polyp) should be suspected in older children and adults
- Management: air or hydrostatic enema reduction; surgery if peritonitis or failed reduction
2. Hypertrophic Pyloric Stenosis (HPS)
| Parameter | Threshold |
|---|---|
| Pyloric muscle thickness | ≥ 3–4 mm |
| Pyloric channel length | ≥ 14–17 mm |
| Pyloric diameter | ≥ 10–14 mm |
3. Ovarian Torsion / Pelvic Pathology
Comparison of Key Contexts
| Feature | Intussusception | HPS |
|---|---|---|
| Age group | 3 months – 6 years (peak) | Neonates (3–6 weeks) |
| Modality | Ultrasound (transverse) | Ultrasound (transverse) |
| Sign appearance | Two concentric rings | Single ring (mucosa + muscle) |
| Clinical presentation | Colicky pain, "currant jelly" stools, palpable mass | Projectile non-bilious vomiting, olive mass |
| Management | Enema reduction / surgery | Pyloromyotomy (Ramstedt) |
Imaging
Double donut sign in dengue
double donut sign dengue
double donut sign dengue ultrasound
dengue gallbladder wall thickening edema ultrasound plasma leakage
dengue gallbladder wall edema double wall ultrasound
Double Donut Sign in Dengue
Pathophysiology
Ultrasound Appearance
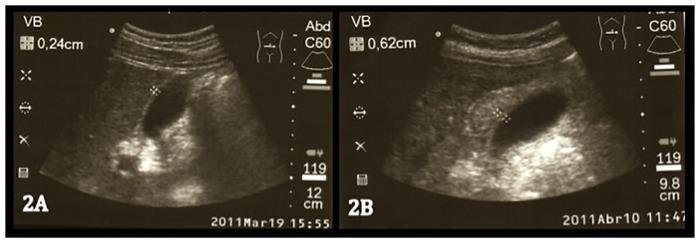
- A layered / striated appearance — alternating echogenic and hypoechoic bands within the wall
- The double donut / double-wall configuration is best seen on transverse cross-section: a hypoechoic (dark) halo surrounds the echogenic inner wall layer, creating two concentric rings
- Gallbladder wall thickness (GBWT) ≥ 3–4 mm is considered abnormal (normal: ~2–3 mm); in severe dengue, GBWT can exceed 6 mm
| Parameter | Normal | Dengue (Critical Phase) |
|---|---|---|
| GBWT | ≤ 0.3 cm | ≥ 0.4–0.6 cm or more |
| Wall appearance | Thin, echogenic | Layered, hypoechoic halo |
| Associated fluid | None | Pericholecystic fluid, ascites, pleural effusion |
Clinical Significance
| Aspect | Detail |
|---|---|
| Timing | Critical phase: days 4–6 of illness |
| Indicator of | Significant plasma leakage / dengue with warning signs |
| Severity marker | GBWT correlates with degree of vascular permeability |
| Associated findings | Ascites, bilateral pleural effusions, periorbital edema |
| Risk | Flags patients at risk for dengue shock syndrome (DSS) and hemorrhagic complications |
Imaging
Differential Diagnosis of Gallbladder Wall Thickening
| Cause | Distinguishing Feature |
|---|---|
| Dengue fever | Fever + thrombocytopenia + dengue serology |
| Acute cholecystitis | Tenderness, Murphy's sign, gallstones |
| Hypoalbuminemia (cirrhosis, nephrotic syndrome) | Low albumin, chronic disease |
| Congestive heart failure | Elevated JVP, cardiomegaly |
| Hepatitis | Elevated transaminases, jaundice |
| Ascites (any cause) | Requires correlation |
Double donut sign in ct scan mri scan in dengue
dengue CT scan MRI findings double donut sign gallbladder
dengue CT scan gallbladder wall thickening double donut sign
dengue fever CT abdomen findings plasma leakage ascites
dengue MRI brain spinal cord neurological imaging findings
Double Donut Sign in Dengue on CT and MRI
On CT Scan
Appearance
| Layer | CT Appearance |
|---|---|
| Inner layer (mucosa + submucosa) | Hyperattenuating (enhances with contrast) |
| Middle layer (submucosal edema) | Hypoattenuating (low-density fluid/edema) |
| Outer layer (serosa/muscularis) | Iso- to slightly hyperattenuating |
Additional CT Findings in Dengue
| Finding | CT Appearance |
|---|---|
| Gallbladder wall thickening | Wall > 3 mm, stratified/layered |
| Pericholecystic fluid | Low-density fluid around GB fossa |
| Ascites | Free fluid in peritoneal cavity |
| Pleural effusions | Bilateral > unilateral; right-sided predominance |
| Hepatosplenomegaly | Enlarged liver and/or spleen |
| Peripancreatic edema | Stranding around pancreas (in severe cases) |
| Retroperitoneal edema | Fat stranding |
CT is not the first-line modality for dengue (ultrasound is preferred due to cost, availability, and lack of radiation), but CT is used when complications like hemorrhage, bowel involvement, or abdominal organ pathology need to be excluded.
On MRI
Appearance
| Sequence | Appearance |
|---|---|
| T1-weighted | Inner wall isointense; edematous middle layer hypointense |
| T2-weighted | Middle edematous layer markedly hyperintense (bright) — best sequence for the double donut sign |
| T1 post-gadolinium | Enhancement of inner mucosal and outer serosal layers with non-enhancing edematous middle layer — classic "sandwich" / double donut pattern |
| MRCP | Can assess biliary involvement; GB wall thickening clearly delineated |
- Bright (hyperintense) edematous halo = inner ring
- Hypointense lumen content
- Bright pericholecystic fluid surrounding the outer wall ...producing the double donut appearance.
MRI in Dengue Encephalitis / Neurological Dengue
| Location | MRI Finding |
|---|---|
| Bilateral thalami | T2/FLAIR hyperintensities (most characteristic) |
| Cerebral cortex | Diffuse edema, FLAIR signal changes |
| Cerebellum | Cerebellar edema, T2 signal changes |
| Basal ganglia | Hyperintensities on T2/FLAIR |
| Spinal cord | Myelitis pattern (rare) |
| White matter | Leukoencephalopathy (rare) |
Summary Comparison Across Modalities
| Feature | Ultrasound | CT | MRI |
|---|---|---|---|
| Double donut sign | Hypoechoic halo around echogenic wall | Hypoattenuating edema band between enhancing layers | T2 hyperintense edema band between enhancing layers |
| Best sequence/mode | B-mode transverse | CECT axial | T2 axial / post-Gad T1 |
| Added value | Bedside, no radiation, first-line | Detects hemorrhage, complications | Best soft tissue resolution, brain involvement |
| Limitation | Operator-dependent | Radiation, contrast risk | Cost, availability, time |
| Role in dengue | Screening and monitoring | Second-line / complications | CNS dengue, complex cases |
Double donut sign in brain ct mri
double donut sign brain CT MRI
double donut sign brain CT MRI
double donut sign thalamus bilateral dengue encephalitis MRI T2
bilateral thalamic hyperintensity dengue encephalitis MRI axial
Double Donut Sign in Brain CT/MRI — with Dengue Context
What Is the Double Donut Sign on Brain MRI?
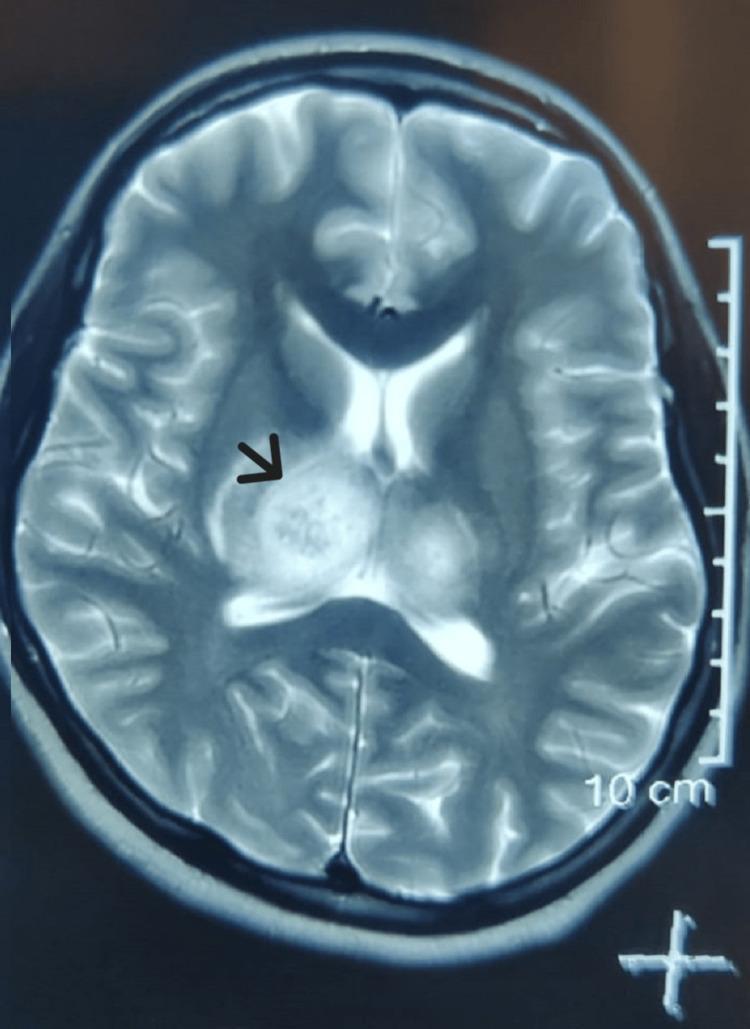
- Two symmetrical, ovoid, hyperintense lesions in the bilateral thalami
- Flanking the third ventricle centrally
- Creating a "double donut" or "owl eye" configuration
- With possible mass effect on the third ventricle and posterior limbs of the internal capsule
Double Donut Sign in Dengue Encephalitis
Pathophysiology
- Direct neurotropism — DENV crosses the blood-brain barrier and infects neurons/glial cells
- Immune-mediated injury — cytokine storm, autoimmune demyelination
- Metabolic encephalopathy — hepatic failure, electrolyte disturbance, SIADH
- Microvascular injury — thrombocytopenia-related microhemorrhages, cerebral edema
MRI Sequences and Findings
| Sequence | Finding in Dengue Encephalitis |
|---|---|
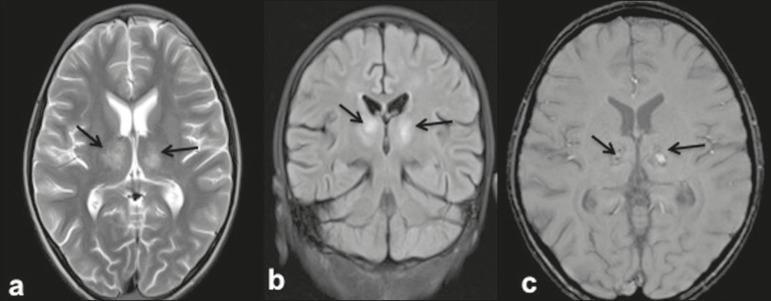
| T2-weighted (axial) | Bilateral thalamic hyperintensities — the double donut sign; well-defined oval lesions |
| FLAIR | Confirms edema and inflammation in thalami; suppresses CSF to better delineate lesions |
| DWI | Restricted diffusion if cytotoxic edema (acute ischemic/necrotic component) |
| SWI / GRE | Hypointense foci with blooming = microhemorrhages within thalamic lesions |
| T1 post-Gadolinium | Variable; may show ring or patchy enhancement in severe cases |
Imaging
CT Findings in Dengue Encephalitis
| Finding | Appearance on CT |
|---|---|
| Bilateral thalamic hypodensity | Symmetric low-density areas in both thalami (the CT correlate of the double donut sign) |
| Cerebral edema | Sulcal effacement, loss of grey-white differentiation |
| Hemorrhagic transformation | Hyperdense foci within thalami or elsewhere |
| Herniation | In severe cases with massive edema |
| Normal CT | CT can be entirely normal early — MRI is far superior |
CT may miss subtle thalamic lesions that are clearly visible on T2/FLAIR MRI. A normal CT does not exclude dengue encephalitis.
Differential Diagnosis of the Double Donut Sign (Bilateral Thalamic Lesions)
| Condition | Distinguishing Features |
|---|---|
| Dengue encephalitis | Dengue serology +ve, fever, thrombocytopenia, endemic area |
| Japanese Encephalitis (JEV) | Most common cause; similar MRI pattern; JEV IgM in CSF |
| West Nile Virus encephalitis | Involves thalamus, basal ganglia, brainstem; WNV serology |
| Wernicke's encephalopathy | Thiamine deficiency; also involves mammillary bodies and periaqueductal grey |
| Deep cerebral venous thrombosis | Bilateral thalamic venous infarcts; MRV shows thrombosed deep veins |
| Artery of Percheron infarct | Single arterial territory supplying both thalami; DWI positive |
| Creutzfeldt-Jakob disease (CJD) | "Pulvinar sign"; rapidly progressive dementia; DWI striking |
| Acute necrotizing encephalopathy | Children; bilateral thalamic necrosis; often post-viral/influenza |
| Osmotic demyelination | Central pontine + extrapontine myelinolysis; associated with rapid Na correction |
| CNS lymphoma / toxoplasmosis | HIV context; ring-enhancing lesions (Harrison's, p. 5928) |
Summary
| Feature | Detail |
|---|---|
| Sign | Double donut sign = bilateral symmetrical thalamic hyperintensities on axial T2/FLAIR |
| Best modality | MRI (T2, FLAIR, DWI, SWI) |
| CT value | Low-density thalamic changes; less sensitive; hemorrhage detection |
| Dengue mechanism | Direct neurotropism + immune injury + microvascular hemorrhage |
| Key additional finding | SWI microhemorrhages suggest hemorrhagic dengue encephalitis |
| Clinical correlation | Altered consciousness, seizures, fever, thrombocytopenia in dengue-endemic region |