Pathological and physiological jaundice
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative textbooks. Let me compile a thorough answer.
Physiological and Pathological Jaundice
Jaundice (icterus) is the yellow discoloration of the skin, sclera, and mucous membranes due to accumulation of bilirubin in extracellular fluid. It becomes clinically visible when serum bilirubin rises above ~1.5-3 mg/dL (normal is ~0.5 mg/dL or lower).
Bilirubin Metabolism - The Foundation
Understanding jaundice requires knowing normal bilirubin metabolism:
- Production: 65-80% of bilirubin comes from breakdown of hemoglobin in senescent RBCs. Macrophages split Hb into globin and heme; cleavage of the heme ring releases free iron (transported by transferrin) and a 4-pyrrole chain reduced to unconjugated (indirect) bilirubin - lipophilic, bound to albumin.
- Transport: Unconjugated bilirubin bound to albumin travels to the liver.
- Conjugation: Hepatocytes use UGT1A1 (UDP-glucuronosyltransferase) to convert bilirubin to monoglucuronide and diglucuronide conjugates - water-soluble, direct bilirubin.
- Excretion: Conjugated bilirubin enters bile canaliculi via MRP2 transporter, passes into bile, and is excreted. Conjugated bilirubin cannot be reabsorbed by biliary or intestinal epithelium under normal circumstances.
Classification of Jaundice
| Type | Bilirubin Fraction | Urine Bilirubin | Urine Urobilinogen | Stools |
|---|---|---|---|---|
| Pre-hepatic (hemolytic) | Unconjugated (indirect) | Absent | Increased | Dark |
| Hepatocellular | Both (mixed) | Present | Variable | Pale |
| Post-hepatic (obstructive) | Conjugated (direct) | Present | Absent | Pale/Clay |
Physiological Jaundice (Neonatal)
Definition
A benign, self-limiting unconjugated hyperbilirubinemia occurring in approximately 50% of normal newborns in the first week of life.
Mechanism - Three Contributing Factors
Neonatal jaundice reflects the immaturity of bilirubin metabolism plus higher production:
- Increased bilirubin production: Neonates have a higher RBC turnover rate - fetal hemoglobin (HbF) is replaced by adult HbA, leading to excess hemolysis.
- Decreased hepatic clearance and conjugation: The UGT1A1 enzyme system is immature, especially in premature infants; hepatic uptake proteins (ligandin/Y protein) are also reduced.
- Increased enterohepatic recirculation: The neonatal gut has high beta-glucuronidase activity, which deconjugates bilirubin back to the unconjugated form, allowing reabsorption.
Clinical Features
- Jaundice never present on day 1 of life (appearance within 24 hours is almost always pathological)
- Total bilirubin peaks between day 2-5 at approximately 6 mg/dL in term infants
- Yellow discoloration resolves by 2 weeks in term infants
- Nearly every newborn develops unconjugated bilirubin >1 mg/dL (adult normal upper limit); jaundice becomes visible when bilirubin exceeds ~5 mg/dL
Breast Milk Jaundice
A distinct, second most common cause of neonatal jaundice:
- Pathophysiology uncertain - possibly hormonally mediated or due to increased enterohepatic resorption
- Peaks later than physiologic jaundice: around days 10-21
- May persist for 3-10 weeks
- Mild unconjugated hyperbilirubinemia; benign course
Pathological Jaundice
Key Distinguishing Features from Physiological Jaundice (Neonatal Context)
| Feature | Physiological | Pathological |
|---|---|---|
| Onset | Day 2-3 | Within 24 hours |
| Bilirubin fraction | Unconjugated | Conjugated OR very high unconjugated |
| Duration (term) | Resolves <2 weeks | Persists beyond 3 weeks |
| Rise rate | Gradual | Rapid |
| Bilirubin level | <12 mg/dL (term) | >12 mg/dL (term), any level with direct fraction |
| Infant appearance | Well | May appear sick |
Red flags for pathological jaundice in infants (Box 166.1, Rosen's Emergency Medicine):
- Jaundice appearing within 24 hours of birth
- Any elevated direct (conjugated) bilirubin - always pathological
- Rapidly rising total serum bilirubin unexplained by history/exam
- TSB approaching exchange transfusion level or not responding to phototherapy
- Jaundice persisting beyond 3 weeks of age
- Sick-appearing infant
Causes of Pathological (Unconjugated) Hyperbilirubinemia
A. Overproduction (pre-hepatic / hemolytic):
- Inherited hemolytic disorders: Spherocytosis, sickle cell anemia, thalassemia, G6PD deficiency, pyruvate kinase deficiency
- Acquired hemolytic disorders: Microangiopathic hemolytic anemia (HUS/TTP), paroxysmal nocturnal hemoglobinuria, immune hemolysis, malaria, babesiosis
- Ineffective erythropoiesis: Cobalamin, folate, iron deficiency
- Neonatal specific: ABO/Rh isoimmunization, cephalhematoma resorption
- Serum bilirubin rarely exceeds 5 mg/dL in chronic hemolysis; higher levels suggest concurrent hepatic/renal dysfunction
B. Impaired hepatic uptake:
- Drugs: Rifampin, probenecid, atazanavir, certain penicillins and cephalosporins
C. Impaired conjugation (genetic):
- Crigler-Najjar type I: Complete absence of UGT1A1 activity; bilirubin >20 mg/dL; kernicterus in infancy; often fatal without liver transplant
- Crigler-Najjar type II: Residual UGT1A1 activity <10%; bilirubin 6-25 mg/dL; phenobarbital-responsive (induces residual enzyme); survives into adulthood
- Gilbert's syndrome: UGT1A1 activity 10-35% of normal; mild unconjugated hyperbilirubinemia, benign; triggered by fasting, illness, or stress
Causes of Pathological (Conjugated) Hyperbilirubinemia
Conjugated hyperbilirubinemia is always pathological - even in neonates.
Inherited:
- Dubin-Johnson syndrome: Defective hepatocyte secretion of conjugated bilirubin into bile (MRP2 defect); benign
- Rotor syndrome: Similar but without liver pigmentation
Hepatocellular disease:
- Viral hepatitis (Hep A, B, C, D, E; CMV; EBV)
- Alcoholic liver disease, non-alcoholic fatty liver disease
- Autoimmune hepatitis
- Drug-induced liver injury (acetaminophen toxicity)
- Wilson's disease (especially in patients <40 years)
- Cirrhosis
Cholestatic / Obstructive:
- Intrahepatic: Primary biliary cholangitis (AMA-positive), primary sclerosing cholangitis, drug-induced cholestasis, intrahepatic cholestasis of pregnancy
- Extrahepatic: Choledocholithiasis, pancreatic head cancer, cholangiocarcinoma, biliary strictures
- Neonatal: Biliary atresia (must be excluded urgently in persistent neonatal jaundice), choledochal cyst, neonatal hepatitis, TORCHS infections, inborn errors of metabolism
Complications of Pathological Jaundice
Kernicterus (Bilirubin-Induced Neurologic Dysfunction - BIND)
- Unconjugated bilirubin crosses the blood-brain barrier and causes cell death
- Risk increases significantly when bilirubin exceeds 20-25 mg/dL
- Acute bilirubin encephalopathy (ABE): Somnolence, poor feeding, hypotonia/hypertonia, high-pitched cry → lethargy, retrocollis, opisthotonos, fever, apnea, seizures, death
- Chronic sequelae (Kernicterus): Cerebral palsy, sensorineural hearing loss, upward gaze palsy, intellectual disability
- ABE may be reversible if treated promptly; kernicterus is permanent
Diagnostic Approach to Jaundice
The flowchart below from Harrison's Principles of Internal Medicine (22nd ed.) illustrates the systematic evaluation:
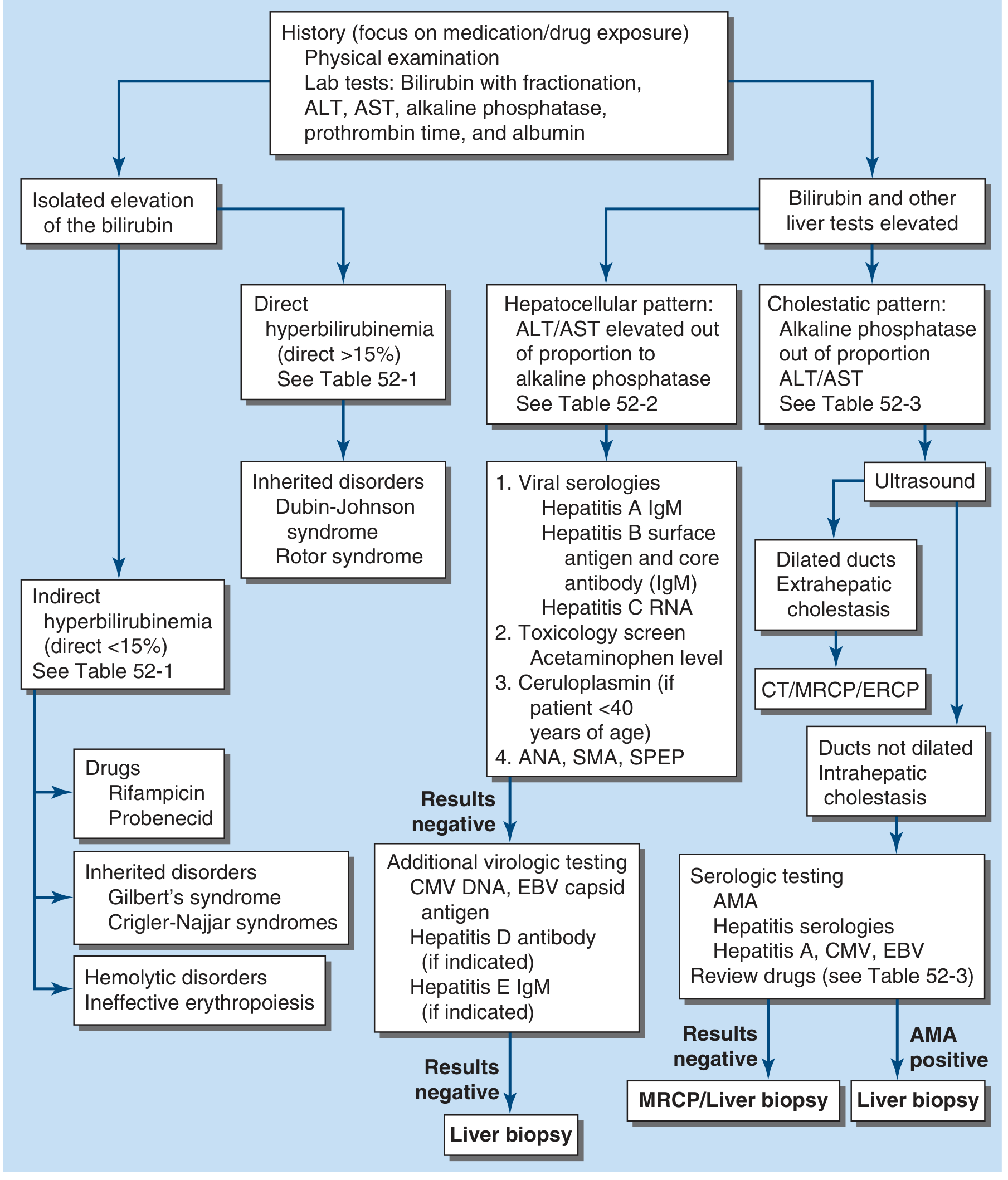
Key steps:
- Fractionate bilirubin: predominantly unconjugated or conjugated?
- Are other liver tests (ALT, AST, ALP, albumin, PT) normal or elevated?
- If elevated: hepatocellular pattern (ALT/AST disproportionate) vs. cholestatic pattern (ALP disproportionate)?
- If cholestatic: ultrasound to check for dilated bile ducts (extrahepatic obstruction) vs. non-dilated (intrahepatic cholestasis)
Treatment Principles
| Condition | Treatment |
|---|---|
| Physiological neonatal jaundice | Reassurance, adequate feeding |
| Neonatal hyperbilirubinemia (approaching toxic levels) | Phototherapy - converts bilirubin to photoisomers and water-soluble oxidation products that don't require conjugation for excretion |
| Severe/exchange-level hyperbilirubinemia | Exchange transfusion |
| Crigler-Najjar type II | Phenobarbital (induces UGT1A1) |
| Crigler-Najjar type I | Liver transplantation |
| Obstructive jaundice | Surgical or endoscopic biliary decompression (ERCP stenting, surgical bypass) |
| Hemolytic jaundice | Treat underlying cause |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Edition (2025), Chapter 52
- Rosen's Emergency Medicine, 9th Edition, Chapter 166 - Neonatal Jaundice
- Medical Physiology (Boron & Boulpaep), Box 46-1 - Jaundice
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease, Chapter on Jaundice
This is a shared conversation. Sign in to Orris to start your own chat.