Give me detailed notes on erector spinae plane block
Reading File
Finding Sources
Searching PubMed
"erector spinae plane block" AND analgesia
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading Article
PMID: 37811665
I now have comprehensive, well-sourced content from three major anesthesia textbooks plus a 2023 Cochrane review. I have all I need to compile detailed notes.
Erector Spinae Plane (ESP) Block - Detailed Notes
1. Historical Background
- First described in 2016 as an analgesic technique for neuropathic chest wall pain
- Rapidly gained popularity as an alternative to paravertebral block (PVB) and neuraxial techniques
- Considered a fascial plane block - a category of ultrasound-guided regional techniques
2. Anatomy
Erector Spinae Muscle Group
The erector spinae group consists of three muscles:
- Iliocostalis (most lateral)
- Longissimus (intermediate)
- Spinalis (most medial)
These function together to straighten and rotate the axial skeleton (paraspinal extensors).
Superficial relations vary by level:
- High thoracic: muscles lie deep to the trapezius and rhomboid muscles
- Low thoracic: lie deep to the latissimus dorsi
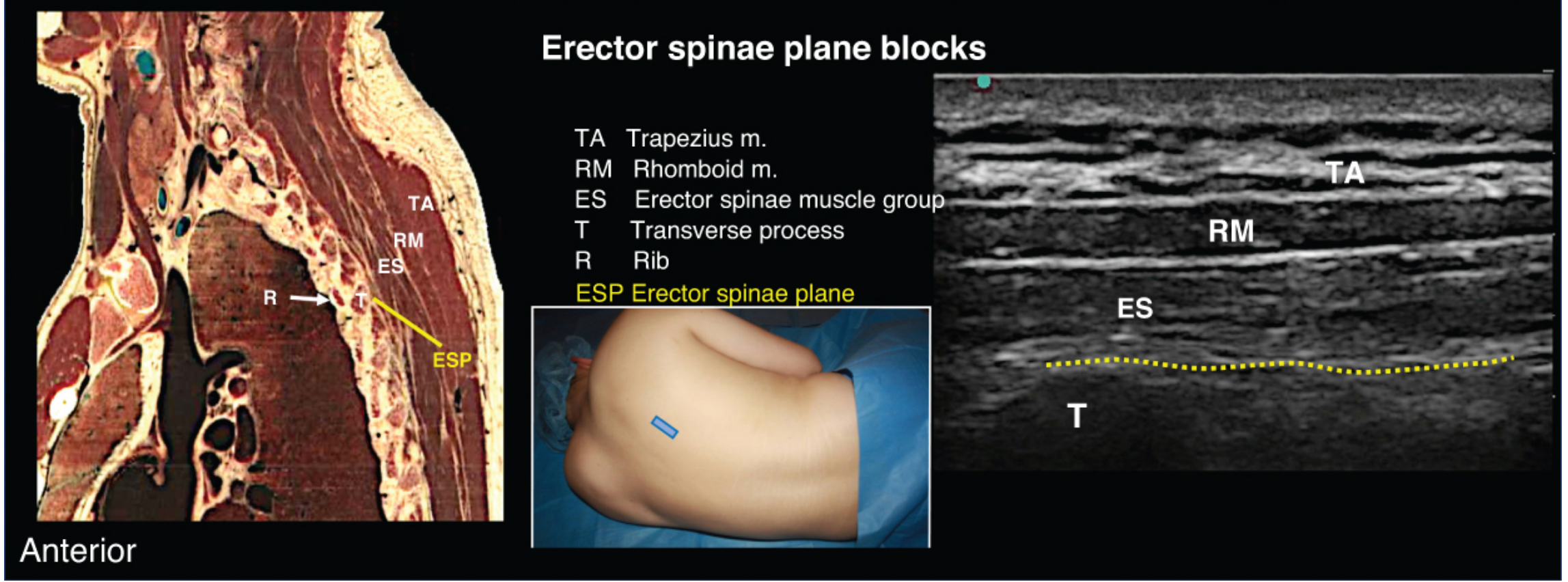
The ESP plane lies between the anterior surface of the erector spinae muscle group and the transverse processes of the vertebrae. This fascial plane runs continuously from the cervical vertebrae (C1) and T1 down to the medial sacral crest on both sides of the spine.
3. Mechanism of Action
The exact mechanism is not fully elucidated, but the proposed mechanisms include:
- Local anesthetic diffusion - Injectate spreads cranially and caudally within the continuous ESP fascial plane
- Paravertebral space diffusion - LA may track anteriorly into the paravertebral space (some authors consider the ESP block a variant of the PVB)
- Blockade of dorsal and ventral rami of thoracic spinal nerves
- Sympathetic nerve fiber blockade - contributing to visceral pain control
- A 20 mL injection at T5 can result in spread from C7 to T8 levels
Both somatic and visceral analgesia are provided, though the visceral component is variable.
4. Indications
| Surgical / Procedural | Acute Pain / Trauma |
|---|---|
| Thoracotomy / VATS | Rib fractures |
| Breast surgery | Post-thoracotomy pain |
| Spine surgery | Chronic chest wall neuropathic pain |
| Cardiac surgery (sternotomy) | |
| Lung surgery | |
| Pyeloplasty | |
| Inguinal hernia repair | |
| Laparoscopic cholecystectomy | |
| Hip surgery | |
| Abdominal wall surgery |
Particularly useful in patients on anticoagulation (where neuraxial or PVB carries higher risk), given the block's posterior and more superficial location.
5. Advantages Over Other Blocks
| Feature | ESP Block | Paravertebral Block | Thoracic Epidural |
|---|---|---|---|
| Pneumothorax risk | Lower | Higher | Negligible |
| Neuraxial injury risk | Very low | Low | Present |
| Technical difficulty | Lower | Moderate-high | Moderate |
| Safe in anticoagulation | Yes | Relatively | No |
| Bilateral easy | Yes | Yes | Yes |
| Visceral analgesia | Variable | Yes | Yes |
| Catheter placement | Yes | Yes | Yes |
The transverse process serves as a reliable osseous backstop - a clear endpoint confirming needle tip position, making the technique more predictable than PVB where the needle "drops" past the transverse process into the paravertebral space.
The location is away from major arteries, pleura, and neuraxial structures compared to PVB.
6. Patient Positioning
- Sitting, or
- Lateral decubitus (block-side up)
Both positions allow good access to the paraspinal region.
7. Ultrasound-Guided Technique
Probe Selection & Placement
- Linear probe (13-6 MHz) - standard for average adult
- Curvilinear probe (8-3 MHz) - for larger patients with deep structures
- Probe placed in parasagittal orientation over the paraspinal skin at the target thoracic or lumbar level
- Slide the probe laterally from the spinous process until the transverse processes are clearly visible (rectangular hyperechoic structures with acoustic shadowing) without pleura interposed between the transverse process and probe
Sonoanatomy to Identify
From superficial to deep:
- Trapezius (upper thoracic) / Latissimus dorsi (lower thoracic)
- Rhomboid muscles (upper thoracic)
- Erector spinae muscle group (large, fusiform)
- Transverse processes - rectangular hyperechoic, with acoustic shadow below
- Ribs appear as overlapping curved lines
- Pleura - hyperechoic line between rib shadows (deeper and more lateral)
In the thoracic area, transverse processes appear as shallow rectangular structures with hyperechoic outlines and acoustic shadowing - distinguishable from the diagonal sawtooth appearance of the laminae.
Needle Technique (In-Plane)
- Insert the needle either:
- Caudal to the probe, directing cranially (caudal-to-cephalad)
- Cephalad to the probe, directing caudally (cephalad-to-caudad)
- Advance in-plane until the tip contacts the transverse process
- Administer a saline bolus (hydrodissection) first to open the collapsible ESP plane - the erector spinae muscle should visibly lift/detach from the transverse process
- If resistance is encountered, withdraw the needle slightly (while keeping it beneath the erector spinae) and re-attempt
- After confirming correct plane (linear spread of LA deep to ESM), inject in 5 mL aliquots after each aspiration
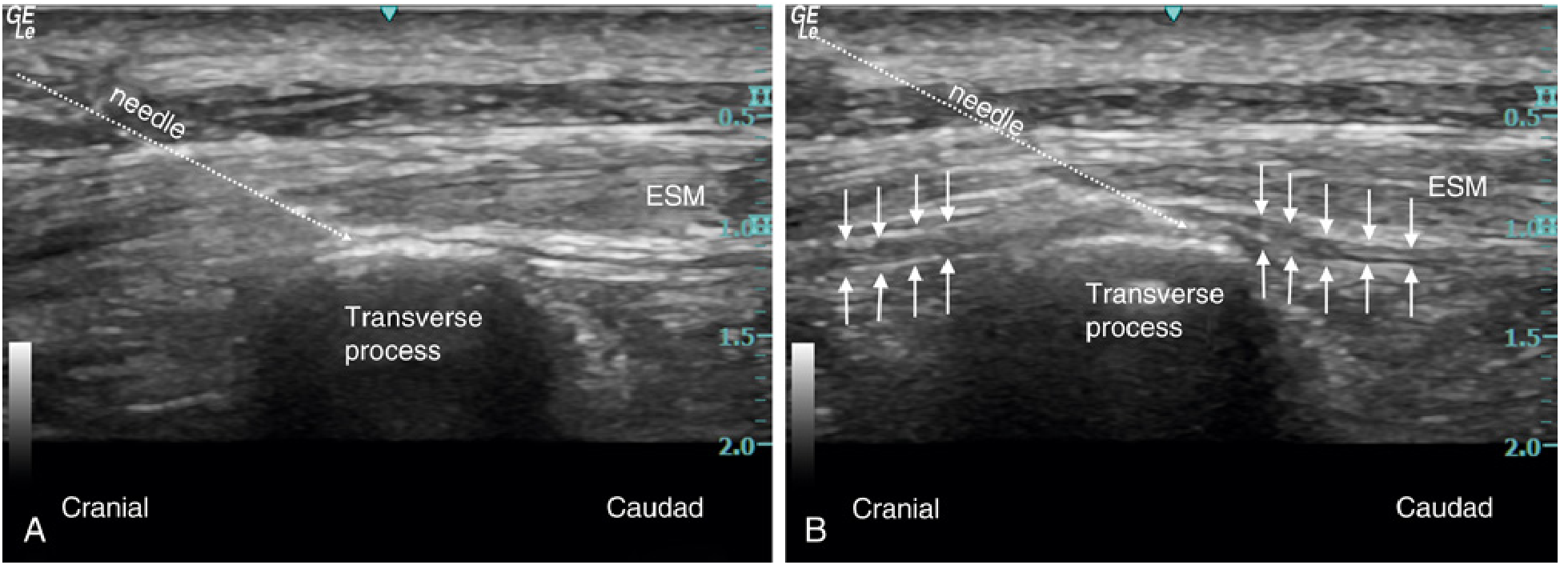
Confirmation of Correct Plane
- Spread of LA visible deep to the erector spinae muscle, superficial to the transverse process
- Cranial and caudal spread spanning multiple vertebral levels
- Muscle visibly lifting off the transverse process
8. Local Anesthetic Dosing
| Parameter | Details |
|---|---|
| Drug choices | Ropivacaine 0.2-0.5%, Bupivacaine 0.25-0.5%, Levobupivacaine |
| Volume (single-shot) | 20-50 mL (large volume required as fascial plane block) |
| Typical adult dose | 20-30 mL of 0.2-0.5% ropivacaine |
| Bilateral blocks | Use lower volumes per side to avoid LAST |
| Catheter infusion | 5-8 mL/h (ropivacaine 0.2%) |
| Catheter insertion depth | 5 cm beyond needle tip |
The large volume is required because the goal is to spread over multiple dermatomes with a single injection.
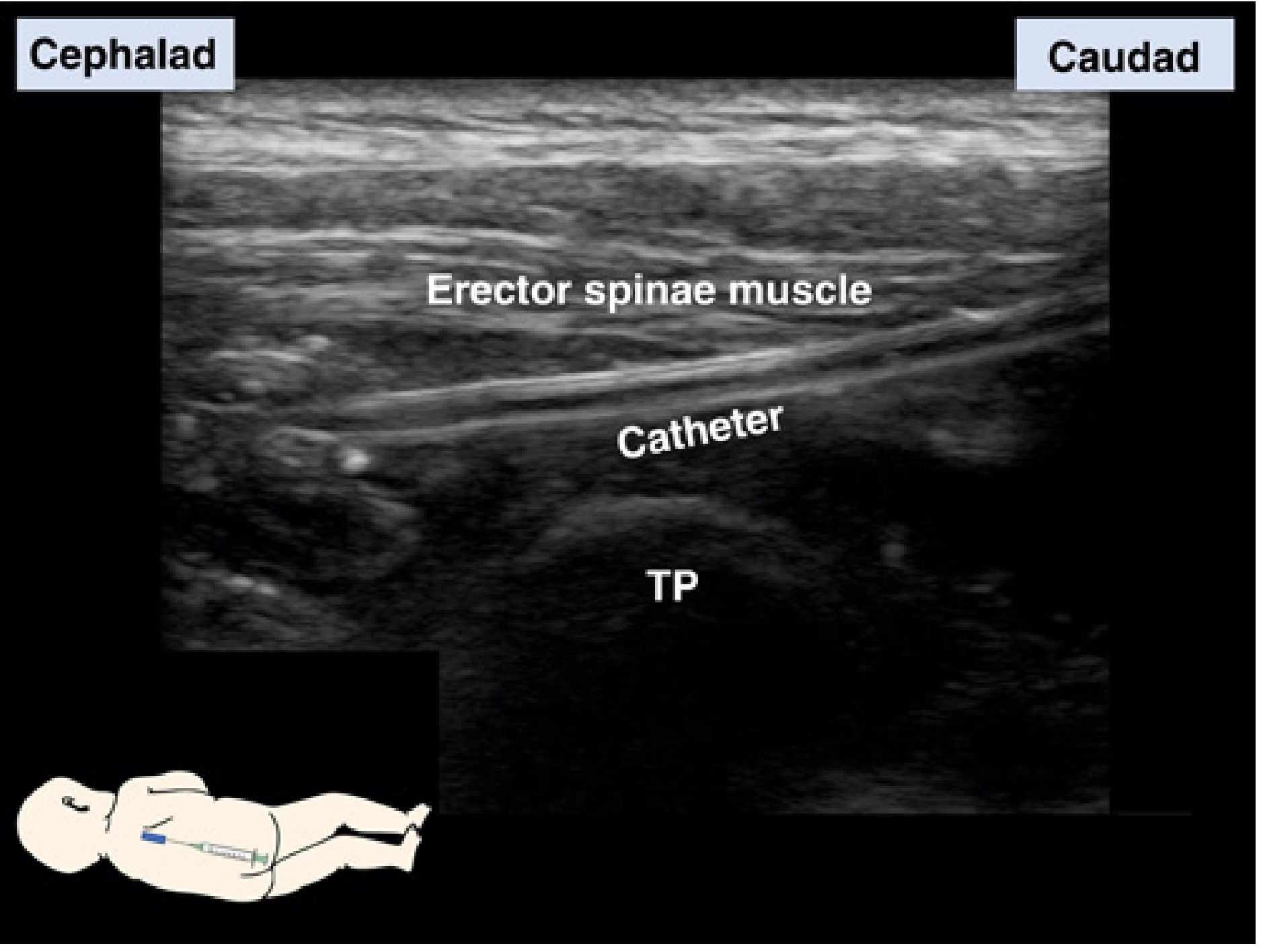
9. Catheter Technique
Continuous ESP block via catheter is well described:
- After hydrodissection opens the plane, pass catheter 5 cm beyond needle tip
- Programmed intermittent bolus, continuous infusion, or patient-controlled options
- Particularly valuable for thoracotomy, rib fractures, and spine surgery
- Case reports include use in neonates and infants for thoracotomy analgesia
10. Landmark Technique (Non-Ultrasound)
- Transverse processes are located 1-2.5 cm lateral to the spinous processes
- Insert needle perpendicularly until transverse process is contacted
- Inject after aspiration; withdraw slightly if resistance is high
- Ultrasound is strongly recommended over landmark technique for safety
11. Complications and Safety Profile
| Complication | Notes |
|---|---|
| LAST (Local Anesthetic Systemic Toxicity) | Key concern - high vascularity of the region, especially with large volumes or bilateral blocks |
| Pneumothorax | Reported; lower risk than PVB but not zero |
| Hematoma | Rare; relatively safe in anticoagulated patients |
| Infection | Standard procedural risk |
| Block failure | Possible if LA doesn't spread to paravertebral space |
The ESP block is lower risk than PVB because:
- Transverse process acts as an osseous backstop - the needle does not need to go "past" it
- Location is more superficial and posterior, away from pleura, major vessels, and neuraxial structures
12. Special Populations
- Anticoagulated patients (e.g., cardiac surgery with cardiopulmonary bypass): ESP block is a preferred analgesic option given lower bleeding risk
- Pediatric / neonatal patients: Case reports of successful use for thoracotomy analgesia, including pre-term infants
- High-risk patients: The more superficial posterior location makes this safer than neuraxial or PVB
13. Comparison with Retrolaminar Block
The retrolaminar block is a closely related fascial plane block:
- The US probe is slid medially from the ESP position until vertebral laminae (diagonal sawtooth structures) are visualized
- LA is deposited on the periosteum of the lamina rather than the transverse process
- Considered an alternative to the ESP block, sometimes used for cardiac and noncardiac pediatric procedures
14. Current Evidence (2023 Cochrane Review)
The 2023 Cochrane systematic review by Schnabel et al. (64 RCTs, 3,973 participants) found:
- vs. No block: Moderate-certainty evidence of a slight but not clinically meaningful reduction in 24-hour pain at rest (MD -0.77 VAS points, 95% CI -1.08 to -0.46)
- vs. Placebo block: Moderate-certainty evidence of no significant difference (MD -0.14, 95% CI -0.29 to 0.00)
- vs. Paravertebral block: Low-certainty evidence - no significant difference in 24-hour pain at rest (MD 0.23)
- Block-related adverse events: No events reported across multiple trials
- Conclusion: ESPB is safe, but the analgesic benefit over placebo is uncertain and may be inferior to PVB in expert hands
A 2025 meta-analysis in European Spine Journal (PMID 40175641) specifically found benefit for postoperative recovery quality in spinal surgery.
15. Key Clinical Pearls
- Inject deep to the erector spinae muscle, superficial to the transverse process - do not inject into the muscle itself
- Hydrodissect first with saline to open the plane before injecting LA
- Large volumes (20-50 mL) are needed to spread across multiple dermatomes - vigilance for LAST is required
- The clear osseous endpoint (transverse process contact) makes this technically simpler than PVB
- It may be inferior to PVB in expert hands but preferred in lower-volume centers or when PVB complications are a concern
- For bilateral blockade, reduce volumes per side to avoid exceeding toxic LA thresholds
- Spread from C7 to T8 is possible from a single T5 injection - plan level selection based on surgical site
- Can be used as rescue analgesia when thoracic epidural fails or is contraindicated
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7e, p. 1951-1952
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, p. 2979-2983
- Miller's Anesthesia, 10e, p. 7344-7345, p. 11082-11083
- Schnabel A et al. Erector spinae plane block for postoperative pain. Cochrane Database Syst Rev. 2023 (PMID 37811665)
- Zhang L et al. Impact of ESPB on postoperative recovery quality in spinal surgery. Eur Spine J. 2025 (PMID 40175641)
This is a shared conversation. Sign in to Orris to start your own chat.