Lung Abscess and Pulmonary Gangrene
Reading File
search_medical_text
lung abscess etiology pathophysiology clinical features diagnosis management
search_medical_text
pulmonary gangrene causes treatment complications
search_medical_image
lung abscess chest X-ray CT scan imaging findings
GradeResponse
GradeResponse
GradeResponse
Lung Abscess and Pulmonary Gangrene
LUNG ABSCESS
Definition
A lung abscess is a localized area of suppurative necrosis within the pulmonary parenchyma, resulting in the formation of one or more cavities containing necrotic debris or fluid, caused by microbial infection.
Classification
| Type | Criteria |
|---|---|
| Primary | Aspiration-related; occurs in otherwise healthy host |
| Secondary | Complicates pre-existing conditions (obstruction, immunosuppression, septic emboli) |
| Acute | Symptoms < 4–6 weeks |
| Chronic | Symptoms > 4–6 weeks |
Etiology & Microbiology
Anaerobes are the dominant pathogens (~90% of cases), typically yielding 3–6 isolates per sample (Harrison's, p. 5087):
- Peptostreptococcus spp.
- Bacteroides spp.
- Fusobacterium nucleatum
- Prevotella melaninogenica
Aerobes/Mixed organisms (particularly in secondary or hospital-acquired cases):
- Staphylococcus aureus (can cause abscess without anaerobic component)
- Klebsiella pneumoniae (classic in alcoholics — "currant jelly" sputum)
- Pseudomonas aeruginosa
- Streptococcus milleri group
- Nocardia, fungi (Aspergillus, Histoplasma) in immunocompromised patients
Predisposing Factors / Pathophysiology
The central mechanism is aspiration of oropharyngeal/gastric contents, followed by:
- Microaspiration of bacteria into dependent lung segments
- Local pneumonitis → tissue necrosis → cavity formation
- Communication with bronchus → air-fluid level develops
Risk factors:
- Altered consciousness (alcohol, seizures, general anesthesia, drug overdose)
- Dysphagia, esophageal disorders
- Poor dental hygiene / periodontal disease (antecedent dental infection is common)
- Bronchial obstruction (tumor, foreign body)
- Septic emboli (IV drug use, right-sided endocarditis)
- Immunosuppression (HIV, chemotherapy, transplant)
Anatomical Distribution
Abscesses typically occur in dependent pulmonary segments (Harrison's, p. 5087):
- Right lower lobe — posterior segment (most common when supine)
- Right upper lobe — posterior segment
- Left lower lobe — posterior segment
- Upper lobe involvement suggests hematogenous spread or specific organisms (e.g., Klebsiella)
Clinical Features
Subacute onset over 1–3 weeks prior to presentation:
- Constitutional: fever, malaise, night sweats, weight loss
- Respiratory: cough, chest pain, dyspnea
- Hallmark: foul-smelling (putrid) sputum — pathognomonic of anaerobic infection
- Hemoptysis (variable)
- Finger clubbing (in chronic cases)
- Signs of consolidation on examination
Diagnosis
Imaging
Chest X-ray:
- Cavitary lesion with a thick wall and air-fluid level
- Usually in dependent segments
- Surrounding consolidation/infiltrate
CT Thorax (gold standard):
- Defines cavity morphology, wall thickness, and multilocularity
- Distinguishes abscess from empyema with bronchopleural fistula
- Key CT features: thick irregular enhancing wall, air-fluid level, surrounding parenchymal consolidation
Differential diagnosis of cavitary lung lesion includes: necrotizing pneumonia, empyema with bronchopleural fistula, pneumatocele, cavitating malignancy, tuberculosis, fungal infection, Wegener's granulomatosis (Harrison's, p. 5087)
Imaging: Lung Abscess in a 12-year-old with CAP
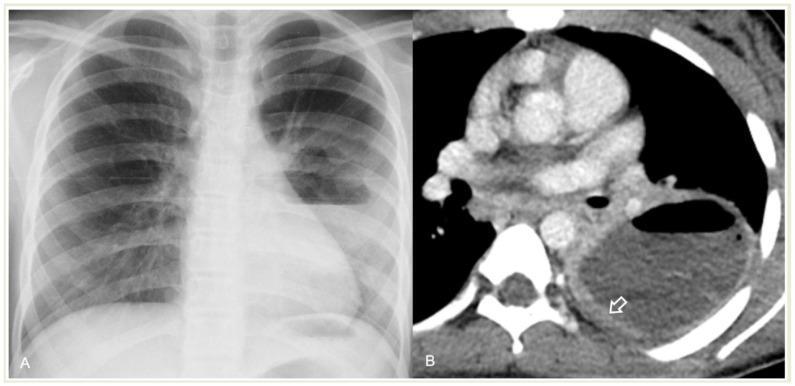
Panel A (CXR): Large cavitary lesion in right lung with prominent air-fluid level. Panel B (CECT): Thick, irregular, strongly enhancing peripheral wall — classic abscess sign. Air-fluid level confirmed.
Laboratory
- CBC: leukocytosis with left shift
- Elevated CRP, ESR
- Blood cultures (positive in hematogenous cases)
- Sputum Gram stain & culture (anaerobic culture requires proper technique)
- Bronchoscopy with BAL/protected specimen brush — if obstruction suspected or no response to treatment
- Serology / fungal antigens if immunocompromised
Management
Antibiotic Therapy
| Scenario | Preferred Regimen |
|---|---|
| Community-acquired (aspiration/anaerobic) | Amoxicillin-clavulanate OR Clindamycin |
| Severe / hospital-acquired | Piperacillin-tazobactam OR Carbapenem ± vancomycin (if MRSA) |
| S. aureus (MSSA) | Flucloxacillin / nafcillin |
| MRSA | Vancomycin or linezolid |
| Klebsiella | Ceftriaxone or fluoroquinolone |
| Fungal | Amphotericin B or azoles (per organism) |
- Duration: typically 4–6 weeks (until radiological resolution)
- IV initially → step down to oral when clinically improving
Postural Drainage
- Physiotherapy and postural drainage to promote expectoration of pus
- Positioning the patient with the affected segment dependent
Bronchoscopy
- Therapeutic: relieve obstruction (foreign body, tumor)
- Diagnostic: obtain cultures, exclude malignancy
Surgical / Interventional
Indicated when:
- Failure to respond to antibiotics after 4–6 weeks
- Massive hemoptysis
- Abscess > 6 cm diameter
- Suspected underlying malignancy
- Tension cavity
- Bronchopleural fistula
Options: CT-guided percutaneous drainage, surgical resection (lobectomy/segmentectomy)
Prognosis & Complications
- Cure rate ~90% with appropriate antibiotic therapy
- Poor prognostic factors: large cavity (>6 cm), immunosuppression, aerobic/nosocomial organisms, obstruction by tumor
- Complications:
- Empyema / bronchopleural fistula
- Massive hemoptysis
- Spread to contralateral lung
- Septicemia
- Pulmonary gangrene (most severe complication — see below)
PULMONARY GANGRENE
Definition
Pulmonary gangrene is the most severe form of pulmonary suppuration, characterized by massive necrosis and putrefaction of a large portion of the lung (a lobe or entire lung), associated with vascular thrombosis and tissue devitalization. It represents the extreme end of the spectrum: Lung abscess → Necrotizing pneumonia → Pulmonary gangrene.
Pathophysiology
- Virulent organisms or impaired host defenses lead to extensive pneumonitis
- Vascular thrombosis of pulmonary vessels (both arterial and venous) within the affected area → ischemic necrosis
- Superimposed septic and putrefactive processes → massive tissue destruction
- Sloughing of necrotic lung tissue → pulmonary sequestrum (detached necrotic tissue floating in a cavity — "sequestrum sign" on imaging)
Etiology
Often polymicrobial. Key organisms:
- Klebsiella pneumoniae (classical cause, especially in diabetics/alcoholics)
- Staphylococcus aureus (including MRSA)
- Streptococcus pneumoniae (type III, uncommon but recognized)
- Pseudomonas aeruginosa
- Anaerobes
- Aspergillus (in severely immunocompromised)
Clinical Features
- Extremely ill, toxic patient
- High-grade fever, rigors
- Severe chest pain
- Massive foul-smelling / blood-stained sputum (expectoration of necrotic lung tissue)
- Rapidly progressive respiratory failure
- Septic shock
- Hemoptysis (can be massive and life-threatening)
Imaging
Chest X-ray:
- Extensive consolidation of a lobe or lung
- Large, irregular cavities
- Sequestrum: a sloughed piece of necrotic lung floating within the cavity
CT Thorax:
- Extensive necrosis with multiple irregular cavities
- Vascular occlusion / absent enhancement of involved parenchyma
- Sequestrum sign: detached lung parenchyma within a fluid-filled cavity
- Contralateral spread may be seen
Comparison: Lung Abscess vs. Pulmonary Gangrene
| Feature | Lung Abscess | Pulmonary Gangrene |
|---|---|---|
| Extent of necrosis | Localized | Massive (lobar/whole lung) |
| Vascular involvement | Minimal | Prominent thrombosis |
| Onset | Subacute (weeks) | Acute/fulminant |
| Tissue viability | Surrounding tissue viable | Tissue devitalized |
| Sequestrum | Absent | Present (pathognomonic) |
| Prognosis | Good (90% with antibiotics) | Poor; high mortality |
| Surgical need | Occasional | Frequent (often mandatory) |
Management of Pulmonary Gangrene
Pulmonary gangrene requires aggressive multidisciplinary management:
- Resuscitation — ICU admission, aggressive fluid resuscitation, vasopressors for septic shock
- Broad-spectrum antibiotics (IV)
- Cover anaerobes + Gram-negatives + MRSA
- E.g., Piperacillin-tazobactam + vancomycin ± metronidazole
- Antifungals if immunocompromised
- Drainage of pus (bronchoscopic or CT-guided)
- Bronchoscopic debridement of necrotic material
- Surgical resection
- Often required due to massive necrosis and failure of conservative therapy
- Pneumonectomy or lobectomy may be necessary
- High operative mortality — surgery reserved for life-threatening hemorrhage or failure to improve
- Supportive care: mechanical ventilation, nutritional support, management of complications
The principles from Bailey & Love's (p. 1031) for gangrene management apply: drainage of pus, liberal debridement of dead tissue, antibiotics, and consideration of primary resection in patients with life-threatening systemic upset.
Prognosis
- Mortality remains high (up to 20–50% in some series)
- Early aggressive treatment improves survival
- Survivors may have significant residual pulmonary dysfunction
Summary
| Aspect | Key Points |
|---|---|
| Lung abscess organisms | Predominantly anaerobes (~90%); S. aureus, Klebsiella in specific contexts |
| Classic presentation | Subacute illness, foul sputum, cavity with air-fluid level in dependent segment |
| First-line treatment | Amoxicillin-clavulanate or clindamycin; 4–6 weeks |
| Pulmonary gangrene | Massive necrosis + vascular thrombosis; lobar/lung involvement; sequestrum |
| Gangrene management | ICU + broad antibiotics + surgical debridement/resection |
This is a shared conversation. Sign in to Orris to start your own chat.