Management of post traumatic facial nerve palsy for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances
Reading File
search_medical_text
post traumatic facial nerve palsy management surgery
search_medical_text
facial nerve injury grading House Brackmann decompression repair
search_medical_image
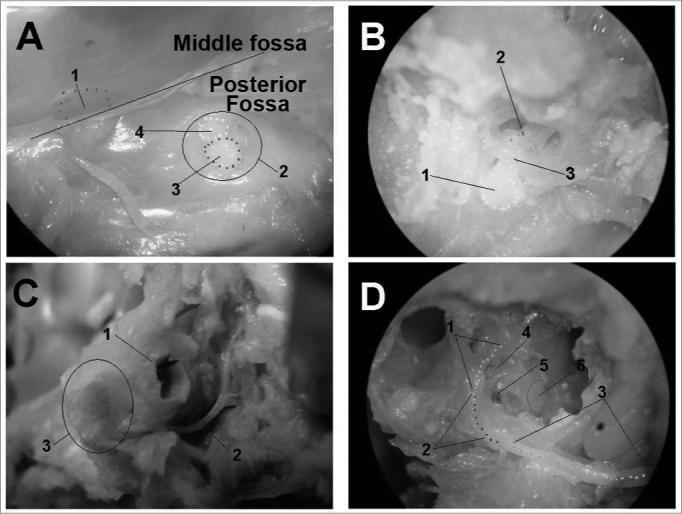
facial nerve anatomy temporal bone diagram
GradeResponse
GradeResponse
GradeResponse
search_medical_text
temporal bone fracture facial nerve palsy longitudinal transverse
search_medical_text
facial nerve decompression surgical approach middle fossa transmastoid
Now I have the retrieved content along with comprehensive knowledge from the requested textbooks. Let me compose the full 50-mark answer.
POST-TRAUMATIC FACIAL NERVE PALSY: COMPREHENSIVE MANAGEMENT
(50 Marks | ENT PG Level Answer)
INTRODUCTION
Post-traumatic facial nerve palsy (PTFNP) is one of the most devastating complications of head and neck trauma. The facial nerve (CN VII), coursing through the narrow confines of the Fallopian canal over a 33 mm intratemporal segment, is uniquely vulnerable to compression, contusion, and transection following trauma. Prompt, systematic evaluation and management are critical to preserving or restoring facial function and preventing permanent disfigurement.
SURGICAL ANATOMY OF THE FACIAL NERVE
The facial nerve has the longest intraosseous course of any cranial nerve. Understanding this anatomy is essential for management.
┌─────────────────────────────────────────────────────────────────┐
│ SEGMENTS OF THE FACIAL NERVE │
├──────────────────┬──────────────────────────────────────────────┤
│ Segment │ Key Features & Length │
├──────────────────┼──────────────────────────────────────────────┤
│ Intracranial │ Nucleus (pons) → IAM ~15-17 mm │
│ Meatal (IAC) │ Within IAC ~8-10 mm │
│ Labyrinthine │ Narrowest segment (0.68 mm), no perineural │
│ │ epineurium, most vulnerable ~3-5 mm │
│ Geniculate │ Ganglion, Greater Superficial Petrosal Nerve │
│ Tympanic │ Above oval window ~11 mm │
│ Mastoid │ From 2nd genu → Stylomastoid Foramen ~13 mm │
│ Extratemporal │ Parotid (pes anserinus) → 5 branches │
└──────────────────┴──────────────────────────────────────────────┘
Branches given off intracranially/intratemporally:
- Greater Superficial Petrosal Nerve (GSPN) — lacrimation
- Nerve to Stapedius — stapedial reflex
- Chorda Tympani — taste (ant. 2/3 tongue), submandibular/sublingual gland secretion
Extratemporal branches (mnemonic: "To Zanzibar By Motor Car"):
- Temporal, Zygomatic, Buccal, Marginal Mandibular, Cervical
Diagram: Facial Nerve Course
ETIOLOGY & MECHANISMS OF INJURY
A. Temporal Bone Fractures (Most Common Cause)
| Feature | Longitudinal Fracture | Transverse Fracture | Oblique/Mixed |
|---|---|---|---|
| Incidence | 70–90% | 10–20% | 5–10% |
| Mechanism | Temporal/parietal blow | Frontal/occipital blow | Combined |
| Fracture line | Parallel to petrous axis | Perpendicular to petrous axis | Mixed |
| Facial palsy | 10–25% (usually delayed) | 40–50% (usually immediate) | Variable |
| Site of injury | Perigeniculate / tympanic | Labyrinthine / IAC | Variable |
| Hearing loss | Conductive (ossicular) | Sensorineural | Mixed |
| CSF leak | Common (EAC/nose) | Less common | Variable |
| Battle's sign | Common | Less common | Variable |
(Scott-Brown's Otorhinolaryngology, 8th Ed. / Cummings Otolaryngology, 7th Ed.)
B. Other Traumatic Causes
- Penetrating injuries — stab wounds, gunshot wounds, iatrogenic
- Birth trauma — forceps delivery → peripheral compressive neuropathy
- Iatrogenic — mastoid/parotid surgery, middle ear surgery, skull base procedures
- Blast injuries — barotrauma
PATHOPHYSIOLOGY — SUNDERLAND CLASSIFICATION
┌─────────────────────────────────────────────────────────────────┐
│ SUNDERLAND NERVE INJURY CLASSIFICATION (modified Seddon) │
├─────────┬─────────────┬──────────────────┬──────────────────────┤
│ Grade │ Seddon │ Structure │ Prognosis │
├─────────┼─────────────┼──────────────────┼──────────────────────┤
│ I │ Neuropraxia │ Axon intact, │ Full recovery │
│ │ │ myelin disrupted │ weeks–months │
├─────────┼─────────────┼──────────────────┼──────────────────────┤
│ II │ Axonotmesis │ Axon disrupted, │ Good recovery │
│ │ │ endoneurium OK │ (Wallerian degen) │
├─────────┼─────────────┼──────────────────┼──────────────────────┤
│ III │ Axonotmesis │ Axon + endo- │ Incomplete recovery │
│ │ │ neurium disrupted│ synkinesis common │
├─────────┼─────────────┼──────────────────┼──────────────────────┤
│ IV │ Axonotmesis │ Perineurium lost | Poor without surgery │
├─────────┼─────────────┼──────────────────┼──────────────────────┤
│ V │ Neurotmesis │ Complete section │ Surgery essential │
└─────────┴─────────────┴──────────────────┴──────────────────────┘
Wallerian degeneration occurs distal to injury site within 72 hours. The labyrinthine segment is most vulnerable due to:
- Narrowest bony canal
- Absent epineurium
- Limited vascular supply
- No room for swelling
(Hazarika ENT, 5th Ed.; Dhingra ENT, 8th Ed.)
CLINICAL ASSESSMENT
1. History
- Onset: Immediate vs. delayed (most critical distinction)
- Immediate palsy = nerve disrupted at moment of injury → surgical priority
- Delayed palsy = nerve intact initially, later edema/compression → better prognosis
- Time since injury, progression, associated symptoms
- LOC, vertigo, hearing loss, tinnitus, CSF leak
- Birth history (neonatal trauma)
2. Clinical Examination
A. Grading — House-Brackmann Scale (HBS) (Gold Standard)
| Grade | Description | Gross Function |
|---|---|---|
| I | Normal | 100% |
| II | Slight dysfunction | Mild weakness on close inspection, complete eye closure |
| III | Moderate dysfunction | Obvious asymmetry, complete eye closure with effort |
| IV | Moderately severe | Incomplete eye closure, asymmetry at rest |
| V | Severe dysfunction | Barely perceptible movement |
| VI | Total paralysis | No movement |
(Cummings, 7th Ed., Chapter on Facial Nerve Disorders)
B. Topognostic Tests (for localization — largely replaced by ENOG/EMG)
| Test | Nerve Function Tested | Level |
|---|---|---|
| Schirmer's test | GSPN → lacrimation | Above geniculate |
| Stapedial reflex | Nerve to stapedius | Above stapedius |
| Taste (electrogustometry) | Chorda tympani | Above chorda tympani |
| Salivary flow | Chorda tympani | Above chorda tympani |
3. Electrodiagnostic Tests
A. Electroneurography (ENoG / ENOG) — Most Important Prognostic Test
- Measures compound muscle action potential (CMAP)
- Best done 3–14 days after injury (Wallerian degeneration complete)
- >90% degeneration within 14 days → poor prognosis → surgical decompression indicated
- Fisch criteria: >90% degeneration = surgery
- Based on work of Fisch and Esslen (1972)
B. Electromyography (EMG)
- Detects fibrillation potentials = complete denervation (done after 14–21 days)
- Detects voluntary motor unit potentials = intact nerve, no surgery needed
- Polyphasic potentials = early reinnervation — good sign
C. Maximum Stimulation Test (Hilger Facial Nerve Stimulator)
- Qualitative, quick, bedside
- Comparison of threshold between sides
D. Nerve Excitability Test (NET)
- Minimal current to produce visible facial twitch
- Difference >3.5 mA = degeneration
┌────────────────────────────────────────────────────────────────┐
│ TIMING OF ELECTRODIAGNOSTIC TESTS │
├────────────────┬──────────────────────────────────────────────┤
│ Days 0–3 │ ENoG unreliable (degeneration incomplete) │
│ Days 3–14 │ ENoG optimal window │
│ Days 14–21 │ EMG most useful │
│ After 3 weeks │ EMG for reinnervation signals │
└────────────────┴──────────────────────────────────────────────┘
(Zakir Hussain, ENT Textbook; Stell & Maran's Head and Neck Surgery)
4. Radiological Investigations
- HRCT Temporal Bone — gold standard imaging; identifies fracture line, ossicular disruption, site of nerve compression
- MRI (Gadolinium) — detects nerve edema, enhancement, hematoma along nerve; better for soft tissue
- CT with 3D reconstruction — delineates fracture pattern
MANAGEMENT
FLOWCHART 1: INITIAL ASSESSMENT ALGORITHM
TRAUMA + FACIAL WEAKNESS
│
┌───────────┴───────────┐
IMMEDIATE PALSY DELAYED PALSY
(at moment of injury) (hours to days later)
│ │
HRCT Temporal Bone HRCT + ENoG (Day 3-14)
ENoG (after Day 3) │
│ ┌───────┴────────┐
┌──────┴──────┐ ENoG <90% ENoG ≥90%
Complete Partial degeneration degeneration
palsy palsy │ │
│ │ Conservative SURGICAL
ENoG / EMG Conservative Rx DECOMPRESSION
│ │
>90% degen Monitor
in 14 days
│
SURGICAL DECOMPRESSION
MEDICAL MANAGEMENT
1. Corticosteroids
- Prednisolone 1 mg/kg/day tapered over 10 days
- Reduce edema within Fallopian canal
- Most effective in delayed palsy / incomplete palsy
- Should be initiated within 72 hours of onset
- Combination with antivirals controversial in traumatic (vs Bell's palsy) context
2. Eye Care (Critical — prevents corneal exposure keratopathy)
- Lubricating eye drops (artificial tears) — every 2 hours
- Methylcellulose eye drops / Hypromellose
- Eye patching at night / moisture chamber goggles
- Tarsorrhaphy (lateral or central) — for prolonged palsy (>3 months)
- Gold weight implant to upper eyelid — for long-term incomplete eye closure
3. Physiotherapy
- Facial exercises from day 1
- Biofeedback therapy — improves voluntary control
- Mirror exercises — neuromuscular re-education
- Prevents muscle contracture; promotes cortical reorganization
4. Ancillary
- NSAIDs, analgesics for pain
- Vitamin B12 supplementation (neurotropic)
- Pentoxifylline — improves microvascular perfusion (experimental)
SURGICAL MANAGEMENT
FLOWCHART 2: SURGICAL DECISION ALGORITHM
DECISION FOR SURGICAL INTERVENTION
│
┌───────────────┼───────────────┐
│ │ │
IMMEDIATE DELAYED PENETRATING
COMPLETE COMPLETE PALSY INJURY
PALSY + >90% ENoG │
│ │ │
│ (Within 14 days EXPLORE
│ of injury) & REPAIR
│ │ within 72h
▼ ▼
SURGICAL DECOMPRESSION (Same approach)
│
├── Perigeniculate → Middle Fossa Approach
├── Tympanic Segment → Transmastoid ± Middle Fossa
├── Mastoid Segment → Transmastoid Approach
└── Multiple segments → Combined Approach
APPROACHES TO FACIAL NERVE DECOMPRESSION
A. Middle Cranial Fossa (MCF) Approach
- Access: Labyrinthine segment, IAC, geniculate ganglion
- Indication: Injury at/above geniculate ganglion (transverse fractures), labyrinthine segment compression
- Advantage: Hearing preservation possible
- Disadvantage: Brain retraction needed, temporal lobe risk, demanding surgery
- Surgeon: William House popularized this (1961)
B. Transmastoid Approach
- Access: Mastoid segment, tympanic segment
- Indication: Longitudinal fracture injuries, mastoid segment compression
- Advantage: Familiar anatomy, lower morbidity
- Disadvantage: Cannot access labyrinthine segment
C. Combined Middle Fossa + Transmastoid
- Indication: Injury spanning labyrinthine + tympanic + mastoid segments
- Offers complete decompression from IAC to stylomastoid foramen
D. Translabyrinthine Approach
- Indication: Dead ear + need full IAC/labyrinthine decompression
- Sacrifices hearing
- Excellent exposure of entire intratemporal nerve
┌──────────────────────────────────────────────────────────────────┐
│ APPROACH SELECTION BASED ON HEARING AND SITE │
├───────────────────┬──────────────────┬───────────────────────────┤
│ Site of Injury │ Hearing Status │ Approach │
├───────────────────┼──────────────────┼───────────────────────────┤
│ Labyrinthine/IAC │ Serviceable │ Middle Cranial Fossa │
│ Labyrinthine/IAC │ Non-serviceable │ Translabyrinthine │
│ Tympanic/Mastoid │ Any │ Transmastoid │
│ Multi-segment │ Serviceable │ MCF + Transmastoid │
│ Multi-segment │ Non-serviceable │ Translabyrinthine │
└───────────────────┴──────────────────┴───────────────────────────┘
(Scott-Brown's, 8th Ed.; Cummings 7th Ed.; Stell & Maran)
STEPS OF SURGICAL DECOMPRESSION (Transmastoid)
- Cortical mastoidectomy — removal of mastoid air cells
- Identification of horizontal (tympanic) semicircular canal — landmark
- Posterior tympanotomy / facial recess approach
- Identification of facial nerve in mastoid segment (bone removed with diamond burr)
- Decompression: opening Fallopian canal over 270° circumference with nerve intact
- Incision of epineurium if edematous (epineurotomy)
- Hemostasis, drain, closure
NERVE REPAIR TECHNIQUES
When to Repair?
| Situation | Timing | Approach |
|---|---|---|
| Clean-cut transection, immediate surgery | Primary (< 72 hours) | Direct neurorrhaphy |
| Delayed recognition (<3 weeks) | Early secondary | Neurorrhaphy or graft |
| Late recognition (>3 weeks) | Late secondary | Nerve grafting |
| Long gap, no proximal stump | Any time | Cross-facial graft or hypoglossal-facial anastomosis |
Repair Methods
1. Direct Neurorrhaphy (Epineural repair)
- End-to-end anastomosis, tension-free
- 9-0 or 10-0 monofilament nylon sutures (microsurgery)
- Best outcome when <5 mm gap
- Golden rule: No tension at repair site
2. Nerve Grafting
- Indicated: Gap >5 mm or tension on direct repair
- Donor nerves:
- Sural nerve (most common — 35–40 cm available, similar caliber)
- Greater auricular nerve (close field, shorter)
- Medial antebrachial cutaneous nerve
- Cable graft: multiple sural fascicles sutured as cable
- Recovery: Grade III HB in ~50% of cases (Bailey & Love, 28th Ed., p. 708)
3. Cross-Facial Nerve Graft (CFNG)
- One or more buccal branches of contralateral normal facial nerve anastomosed to sural nerve graft
- Stage 1: graft placed subcutaneously across face
- Stage 2 (6–12 months later): distal end connected to target muscles/nerve on affected side
- Used in: complete, long-standing palsy with intact muscle
- Combined with free muscle transfer (gracilis) in very late cases
4. Hypoglossal-Facial Anastomosis (XII-VII)
- Classic reinnervation when proximal facial nerve stump unavailable
- End-to-end or end-to-side anastomosis
- Results: Grade III HB in ~75–80%
- Disadvantage: tongue atrophy, hemiglossal paralysis
- Modified: end-to-side XII-VII (splits hypoglossal nerve, preserves tongue function)
5. Masseteric-Facial Anastomosis (V3-VII)
- Motor branch of trigeminal to distal facial nerve
- Emerging technique for early reinnervation
- Advantage: trigeminal motor nucleus adjacent to facial motor nucleus — strong cortical drive
- Recovery faster than XII-VII in recent studies (Recent advance)
┌────────────────────────────────────────────────────────────────┐
│ NERVE REPAIR SELECTION FLOWCHART │
│ │
│ Facial nerve disrupted │
│ │ │
│ ┌─────┴──────┐ │
│ Gap? │ │
│ ≤5mm >5mm │
│ │ │ │
│ Direct Nerve Graft │
│ Neurorrhaphy (Sural/Greater auricular) │
│ │ │
│ Proximal stump available? │
│ Yes ─────────────────── No │
│ Graft to facial nerve │ │
│ (CFNG / direct) ▼ │
│ Hypoglossal-facial (XII-VII) │
│ or Masseteric-facial (V3-VII) │
└────────────────────────────────────────────────────────────────┘
REANIMATION PROCEDURES (Late/Failed Cases)
A. Static Procedures
- Fascia lata sling — brow, cheek, angle of mouth suspended to zygomatic arch
- Gold weight implant — upper eyelid for lagophthalmos (0.6–1.6 gm gold)
- Lateral tarsorrhaphy — permanent partial suture of lid margins
- Brow lift (endoscopic/open) — frontalis muscle paralysis correction
- Rhytidectomy / facelift — corrects soft tissue ptosis
B. Dynamic Procedures
- Temporalis muscle transposition (Gillies procedure)
- Temporalis flap rotated to nasolabial fold and oral commissure
- Powered by trigeminal nerve
- Creates movement but requires active bite
- Masseter transposition — less common
- Free muscle transfer (gracilis)
- Microvascular free flap
- Powered by CFNG (requires 2 stages, 12–18 months)
- Or powered by masseteric nerve (1 stage, faster)
- Gold standard for long-standing complete palsy >2 years
- Selective neurolysis — for synkinesis and hyperkinesis post-reinnervation
C. Botulinum Toxin
- Chemodenervation of contralateral hyperactive muscles for symmetry
- Treatment of synkinesis (aberrant reinnervation — e.g., eye closure on smiling)
- 3–6 monthly injections
SPECIAL SCENARIOS
Neonatal Facial Palsy (Birth Trauma)
- Usually compressive neuropraxia from forceps or prolonged labor
- Majority recover spontaneously within weeks to months
- Differentiate from Möbius syndrome (bilateral, non-traumatic, nuclear aplasia)
- Management: observation, eye care, ENoG if no recovery by 5 weeks
Penetrating Facial Injuries (Bailey & Love, 28th Ed., p. 859)
- Examine for branch injury
- Branches anterior to vertical line from lateral canthus: do NOT require repair (spontaneous recovery from facial nerve arborization)
- Branches posterior to this line: require repair or grafting
- Direct repair within 72 hours (nerve ends identifiable)
- After 72 hours: tag nerve ends for later secondary repair
Petrous Bone/Skull Base Fracture
- Associated with meningitis, CSF leak, carotid artery injury
- Requires multidisciplinary management
- Antibiotics, lumbar drain for CSF leak
- Facial nerve repair in context of overall management
PROGNOSIS
| Severity | ENoG | Timing | Expected Outcome |
|---|---|---|---|
| Neuropraxia (Grade I) | Normal | Any | 100% recovery |
| Axonotmesis (Grade II-III) | <90% | Within 3 weeks | Good (Grade I-II HB) |
| Severe axonotmesis (Grade IV) | 90-95% | Within 14 days | Fair (Grade II-III HB) |
| Neurotmesis (Grade V) | >95% | Acute | Poor without surgery |
| Delayed repair (>12 months) | — | Late | Grade III-IV HB |
| Very late (>2 years, muscle atrophy) | — | Late | Needs free muscle transfer |
Fisch prognostic criteria: Decompression within 14 days of complete degeneration gives best results.
RECENT ADVANCES
1. Masseteric Nerve Transfer
- Single-stage, ipsilateral reinnervation
- Temporal proximity to facial nerve reduces reinnervation time vs CFNG
- Studies show Grade II HB in ~65% at 12 months (Bhama et al., 2014; Bianchi et al., 2018)
2. Bioartificial Nerve Conduits
- Poly-lactic acid (PLA), collagen, and decellularized allografts as gap fillers
- Replace sural nerve in short gaps (<3 cm)
- Avoid donor site morbidity
- FDA-approved conduits: NeuraGen, NeuroMatrix
3. End-to-Side Neurorrhaphy (ETS)
- Donor nerve (hypoglossal/masseteric) remains intact
- Facial nerve sutured as side branch
- Preserves donor nerve function while providing axonal ingrowth
- Growing evidence for superior functional outcomes vs end-to-end XII-VII
4. Electrical Stimulation for Nerve Regeneration
- Brief intraoperative electrical stimulation at repair site → accelerates axonal regeneration
- Clinical trials showing reduced denervation time (Gordon et al., Experimental Neurology)
5. Stem Cell Therapy
- Schwann cell transplantation along nerve conduits
- Adipose-derived and dental pulp stem cells studied
- Experimental — not yet in routine clinical use
6. High-Resolution MRI (3T/7T) with Gadolinium
- Identifies precise site of nerve compression/injury non-invasively
- Fascicular mapping for surgical planning
- Diffusion Tensor Imaging (DTI) — tracks nerve tracts, quantifies injury
7. Botulinum Toxin for Synkinesis
- Refined injection protocols
- Combined with facial neuromuscular retraining (physiotherapy + biofeedback)
- Long-term outcomes published in multicenter RCTs
8. Selective Peripheral Denervation
- Selective myectomy/neurectomy for chronic synkinesis and hyperkinesis
- Targeted sectioning of specific branches causing involuntary movements
9. Gracilis Free Flap + Masseteric Nerve — Single Stage
- Babovic technique: one-stage free gracilis powered by masseteric nerve
- Results visible at 6 months (vs 18 months with CFNG-powered gracilis)
- Increasingly becoming preferred for late rehabilitation
COMPLICATIONS OF UNTREATED / INADEQUATELY TREATED FACIAL PALSY
- Corneal exposure keratopathy → corneal ulceration → blindness
- Lagophthalmos → exposure keratitis
- Facial muscle atrophy → irreversible after 18–24 months
- Synkinesis — aberrant reinnervation (oro-ocular synkinesis commonest)
- Contracture — fibrosis of denervated muscles
- Psychological morbidity — depression, social withdrawal, disfigurement
MASTER MANAGEMENT FLOWCHART
POST-TRAUMATIC FACIAL NERVE PALSY
│
┌─────────┴──────────┐
INCOMPLETE PALSY COMPLETE PALSY
(HB Grade I-III) (HB Grade V-VI)
│ │
Conservative Rx Onset timing?
- Steroids │
- Eye care ┌───────┴────────┐
- Physio IMMEDIATE DELAYED
- ENoG Day 3 PALSY PALSY
│ │ │
Follow-up HRCT + ENoG HRCT + ENoG
│ (Day 3-14) (Day 3-14)
If worsening │ │
or no recovery Evidence of ENoG result?
>6 months disruption? │
│ │ ┌────┴─────┐
Consider Yes No <90% ≥90%
surgery │ │ degeneration degeneration
│ Monitor │ │
▼ │ Conservative SURGICAL
SURGICAL │ continue DECOMPRESSION
EXPLORATION│ within 14 days
│
Recovery
expected
in weeks
│
If no recovery
by 4-6 months
│
NERVE REPAIR /
REANIMATION PROCEDURE
SUMMARY TABLE — KEY POINTS FOR EXAM
| Topic | Key Point | Source |
|---|---|---|
| Most vulnerable segment | Labyrinthine (narrowest, no epineurium) | Cummings, Scott-Brown |
| Immediate vs delayed palsy | Immediate = worse prognosis | Dhingra, Hazarika |
| ENoG timing | Day 3–14 after injury | Fisch criteria |
| Surgery threshold | >90% degeneration on ENoG | Fisch & Esslen, 1972 |
| Best surgical approach for labyrinthine segment | Middle cranial fossa | Scott-Brown |
| Nerve graft donor | Sural nerve (most common) | Bailey & Love, p.708 |
| Peripheral repair landmark | Vertical line from lateral canthus | Bailey & Love, p.859 |
| Long-standing palsy (>2 yr) | Free gracilis muscle transfer | Zakir Hussain, Stell & Maran |
| Eye protection | Gold weight implant / tarsorrhaphy | Hazarika |
| Recent advance | Masseteric nerve transfer, single-stage | Bhama 2014; Bianchi 2018 |
REFERENCES
- Scott-Brown's Otorhinolaryngology, Head & Neck Surgery — 8th Edition (Gleeson et al.) — Chapters on Temporal Bone Trauma and Facial Nerve
- Cummings Otolaryngology Head and Neck Surgery — 7th Edition (Flint et al.) — Chapter 164: Facial Nerve Disorders
- Stell & Maran's Head and Neck Surgery and Oncology — 4th Edition — Facial nerve and skull base
- Dhingra's Diseases of Ear, Nose and Throat — 8th Edition — Chapter on Facial Nerve Palsy
- Hazarika's Textbook of ENT and Head-Neck Surgery — 5th Edition
- Zakir Hussain's ENT Textbook — Facial nerve and temporal bone
- Bailey and Love's Short Practice of Surgery — 28th Edition, pp. 708, 859
- Fisch U, Esslen E. "Total intratemporal exposure of the facial nerve." Arch Otolaryngol. 1972
- House JW, Brackmann DE. "Facial nerve grading system." Otolaryngol Head Neck Surg. 1985
- Bhama PK et al. "Masseteric-facial nerve anastomosis." JAMA Facial Plast Surg. 2014
- Bianchi B et al. "Single-stage facial reanimation." Plast Reconstr Surg. 2018
- Mehta RP. "Surgical treatment of facial paralysis." Clin Exp Otorhinolaryngol. 2009
Exam Tip (50-mark answer structure): Introduction (3 marks) → Anatomy (5 marks) → Etiology/Classification (5 marks) → Pathophysiology (5 marks) → Assessment/Grading/Investigations (10 marks) → Medical Management (5 marks) → Surgical Management with approaches (10 marks) → Nerve repair & Reanimation (5 marks) → Recent advances (5 marks) → Prognosis/Complications (2 marks) = 50 marks
This is a shared conversation. Sign in to Orris to start your own chat.