Hypercalcemic investigation approch
Reading File
Finding Sources
Searching PubMed
"hypercalcemia" AND "diagnosis" AND "investigation"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content and three diagnostic flowcharts from authoritative textbooks. Let me compile the full structured response.
Hypercalcemia: Investigation Approach
Definition and Confirmation
Hypercalcemia is defined as:
- Serum adjusted (albumin-corrected) calcium > 10.5 mg/dL (2.62 mmol/L), or
- Ionized calcium > 5.25 mg/dL (1.31 mmol/L)
Always confirm on two separate occasions before initiating a full workup, and always measure ionized calcium to rule out spurious hypercalcemia from hyperalbuminemia.
Albumin correction formula:
Corrected Ca = Measured Ca + 0.8 × (4.0 - serum albumin in g/dL)
Epidemiology of Causes
- Outpatients: Primary hyperparathyroidism (PHPT) is the most common cause (~90% of cases in ambulatory settings)
- Inpatients: Malignancy is more common
- Together, PHPT and malignancy account for 90-95% of all cases
- Vitamin D supplementation excess has become increasingly common
Differential Diagnosis
| Category | Specific Causes |
|---|---|
| PTH-mediated | Primary hyperparathyroidism (adenoma 80%, hyperplasia 15%, carcinoma <1%), tertiary hyperparathyroidism, MEN-1, MEN-2A, lithium therapy |
| Malignancy | PTHrP-secreting tumors (lung, breast, renal, squamous), osteolytic metastases (breast, myeloma), lymphoma (1,25-OH-D production) |
| Vitamin D excess | Vitamin D3/D2 intoxication, granulomatous disease (sarcoidosis, TB, histoplasmosis) |
| Other endocrine | Thyrotoxicosis, Addison disease, pheochromocytoma, islet cell tumors, acromegaly |
| Drugs | Thiazide diuretics, lithium, calcium carbonate, vitamin A, estrogens/antiestrogens |
| Miscellaneous | Familial hypocalciuric hypercalcemia (FHH), immobilization, milk-alkali syndrome, parenteral nutrition |
Clinical Presentation: "Bones, Stones, Moans, and Abdominal Groans"
| Mnemonic | Manifestation |
|---|---|
| Bones | Bone pain, pathologic fractures, osteitis fibrosa cystica, subperiosteal resorption |
| Stones | Nephrolithiasis, nephrocalcinosis, polyuria, polydipsia |
| Moans | Depression, psychosis, cognitive impairment, lethargy, coma |
| Abdominal groans | Nausea, vomiting, constipation, peptic ulcers, pancreatitis |
Serum calcium >13 mg/dL generally produces symptoms; >14 mg/dL is more characteristic of malignancy than PHPT.
Step-by-Step Investigation Algorithm
Step 1: Confirm Hypercalcemia
- Check serum calcium on 2 occasions
- Measure ionized calcium (free calcium)
- Correct for albumin
- Assess renal function (creatinine, eGFR)
- Take a detailed drug and supplement history (thiazides, lithium, vitamin D, calcium supplements)
Step 2: Measure PTH (the Pivotal Branch Point)
Intact PTH (1-84) is the key first-line test. The result divides the workup into two major pathways:
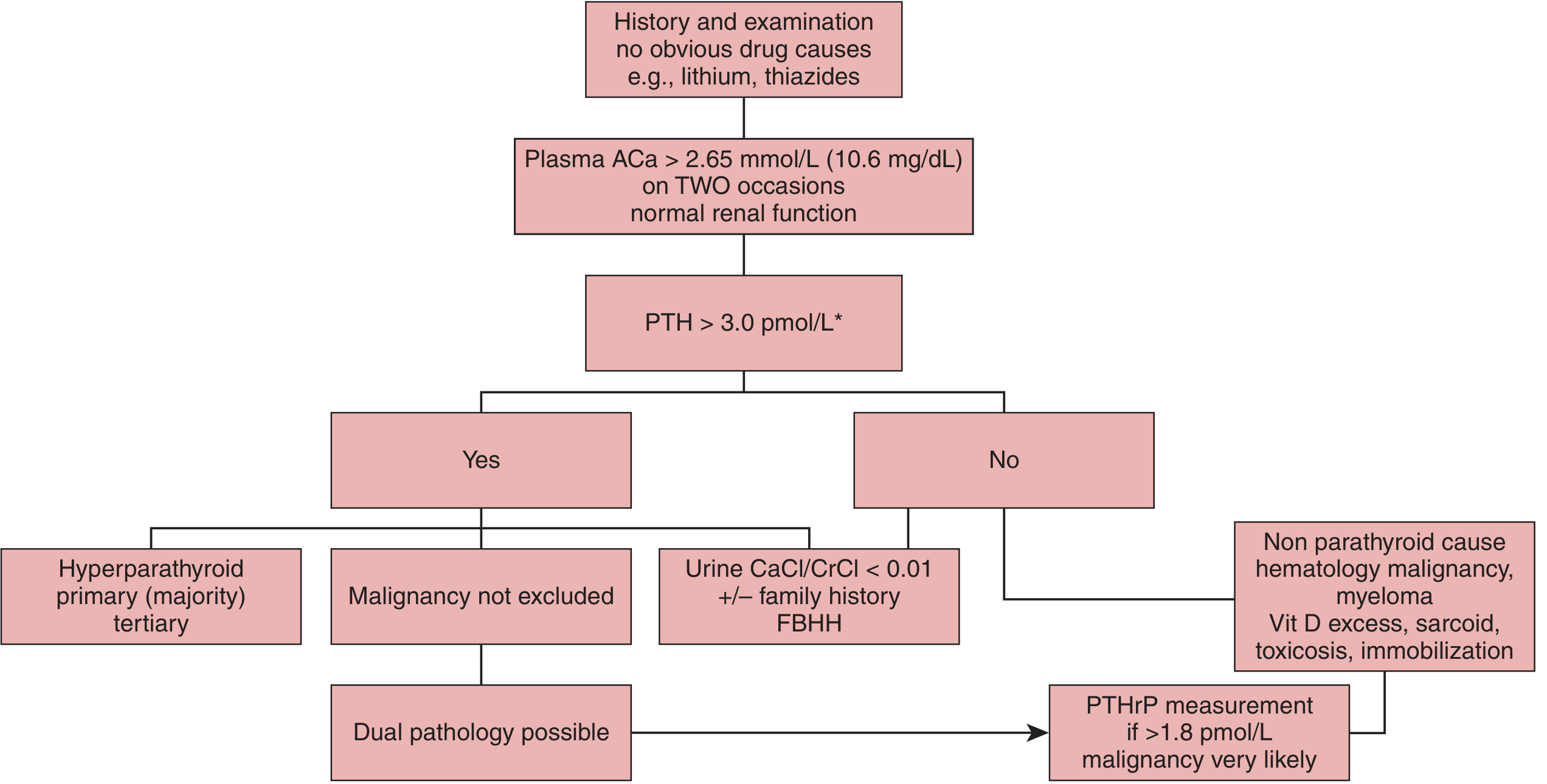
Algorithm A (Tietz Laboratory Medicine, Fig. 54.6A):
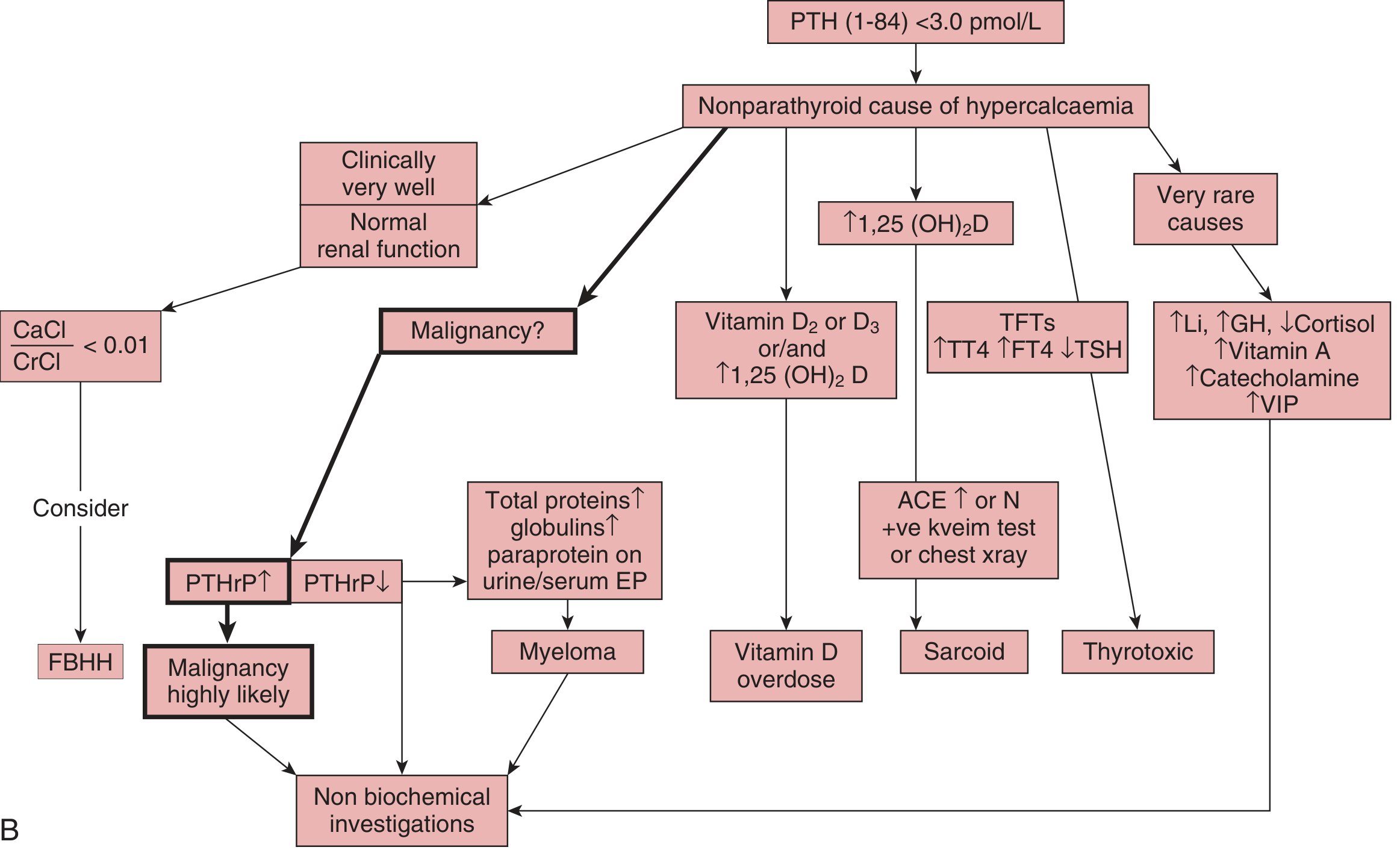
Algorithm B - Nonparathyroid Hypercalcemia (Tietz Laboratory Medicine, Fig. 54.6B):
Algorithm C (Goldman-Cecil Medicine):
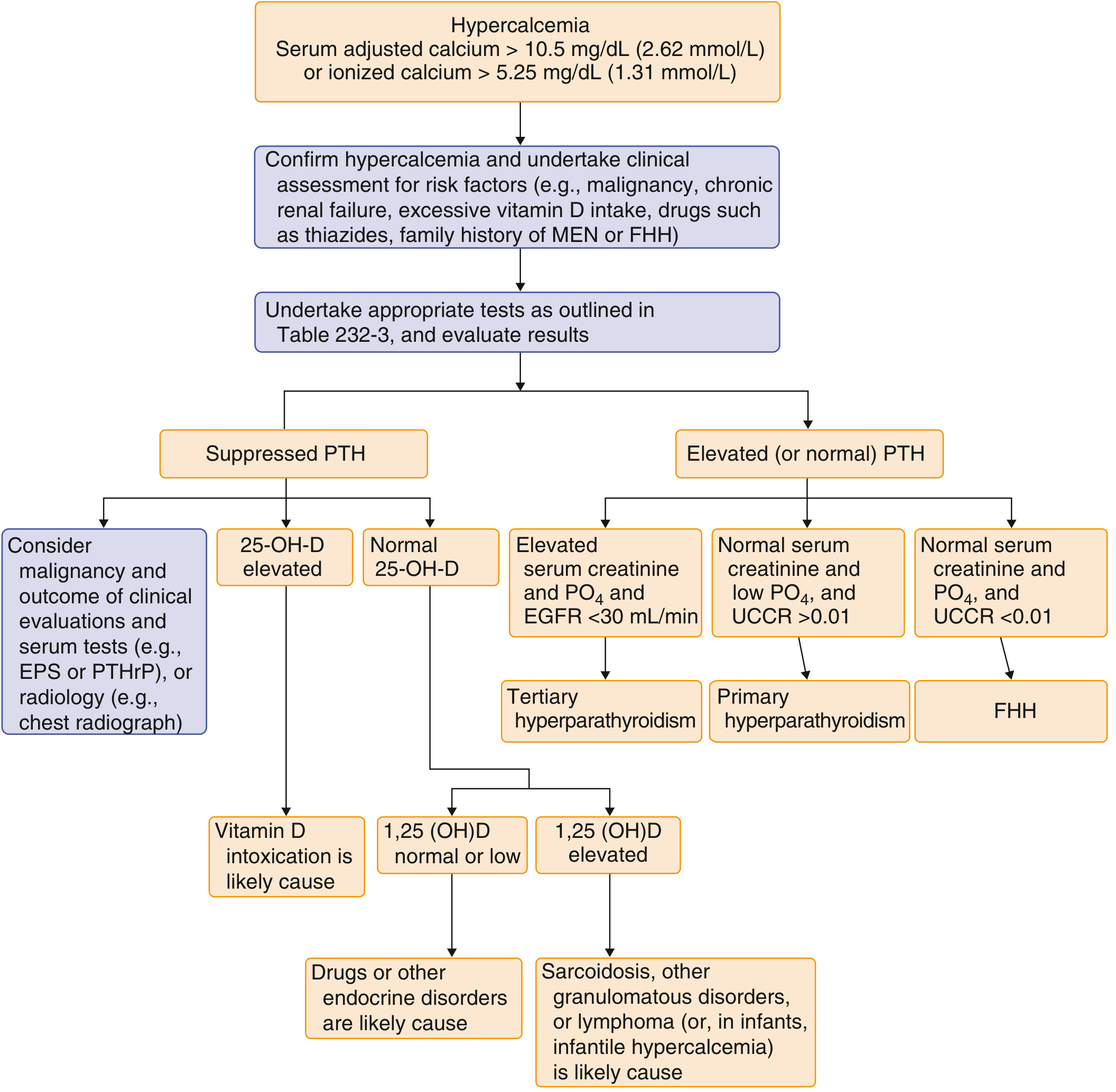
Pathway 1: PTH Elevated or Inappropriately Normal
PTH should be suppressed when calcium is high. Any PTH value in the normal range is therefore "inappropriately normal" and essentially PTH-dependent.
| Finding | Diagnosis |
|---|---|
| Elevated PTH + high calcium + low phosphate + UCCR >0.01 | Primary hyperparathyroidism (PHPT) |
| Elevated PTH + high calcium + UCCR <0.01 + family history | Familial Hypocalciuric Hypercalcemia (FHH) |
| Elevated PTH + elevated creatinine + elevated phosphate + eGFR <30 mL/min | Tertiary hyperparathyroidism |
| Elevated PTH + malignancy not excluded | Check PTHrP - if >1.8 pmol/L, malignancy highly likely (dual pathology) |
Key urine test: UCCR (Urinary Calcium Clearance-to-Creatinine Clearance Ratio)
UCCR = (Urine Ca × Serum Cr) / (Serum Ca × Urine Cr)
- UCCR < 0.01 → suggests FHH
- UCCR > 0.01 → suggests PHPT
Biochemical profile of PHPT (Textbook of Family Medicine):
| Test | Typical Finding |
|---|---|
| Serum calcium | >10.2 mg/dL (mean ~10.7) |
| Serum phosphorus | Low-normal (~2.8 mg/dL) |
| PTH (IRMA) | Elevated (mean ~119 pg/mL; ref 10-65) |
| Alkaline phosphatase | Mildly elevated |
| 25(OH) vitamin D | Often low-normal |
| 1,25(OH)2 vitamin D | Normal or elevated |
| Urinary calcium | Hypercalciuria |
Pathway 2: PTH Suppressed
When PTH is low (<3.0 pmol/L), the cause is non-parathyroid. The next step is:
2a. Check PTHrP
- Elevated PTHrP (>1.8 pmol/L) → Humoral Hypercalcemia of Malignancy (HHM)
- Most common mechanism (80%): solid tumors - squamous cell carcinoma (lung, head/neck), renal, breast
- PTHrP mimics PTH: increases bone resorption, increases renal tubular Ca reabsorption, increases nephrogenic cAMP
- Unlike PTH, PTHrP does NOT stimulate 1,25-(OH)2D production significantly
2b. Check Vitamin D Metabolites
| Metabolite | Interpretation |
|---|---|
| 25-OH-D elevated | Vitamin D2/D3 intoxication (dietary excess, supplements) |
| 1,25-(OH)2D elevated, PTHrP normal | Granulomatous disease (sarcoidosis, TB, histoplasmosis), lymphoma |
Granulomatous macrophages contain 1-alpha-hydroxylase that converts 25-OH-D to active 1,25-(OH)2D autonomously (not regulated by PTH feedback).
2c. Serum Protein Electrophoresis (SPEP) + Urine EP
- Paraprotein (M-band) on SPEP → Multiple Myeloma
- Also check: elevated total protein, globulins, Bence-Jones proteins in urine
- Skeletal survey: lytic bone lesions
2d. Thyroid Function Tests
- TT4/FT4 elevated, TSH suppressed → Thyrotoxicosis (increases bone resorption)
2e. ACE Level + Chest X-ray
- Elevated ACE + bilateral hilar lymphadenopathy or pulmonary infiltrates → Sarcoidosis
2f. Other rare causes
- Elevated lithium level → lithium toxicity
- Elevated GH/IGF-1 → acromegaly
- Low cortisol/ACTH stimulation test → Addison disease
- Elevated catecholamines (urine/plasma metanephrines) → pheochromocytoma
Summary: Key Laboratory Panel for Hypercalcemia Workup
| Test | Purpose |
|---|---|
| Serum adjusted/ionized Ca | Confirm hypercalcemia |
| Serum albumin | Correction factor |
| Intact PTH (1-84) | Primary branch point |
| Serum phosphate | Low in PHPT/HHM; high in CKD |
| Serum creatinine/eGFR | Assess renal function |
| 24-hr urine calcium + creatinine (UCCR) | PHPT vs. FHH |
| PTHrP | Humoral malignancy |
| 25-OH-D | Vitamin D toxicity |
| 1,25-(OH)2D | Granulomatous disease, lymphoma |
| Serum/urine protein electrophoresis | Multiple myeloma |
| TFTs (TSH, FT4) | Thyrotoxicosis |
| Serum ACE | Sarcoidosis |
| Alkaline phosphatase | Bone involvement |
| Bone-specific ALP / urine DPD, PYD | Bone turnover markers (PHPT) |
| Chest X-ray | Malignancy, sarcoidosis, granulomas |
Severity Classification
| Grade | Serum Calcium | Action |
|---|---|---|
| Mild | 10.5-11.9 mg/dL | Outpatient investigation, no urgent treatment |
| Moderate | 12.0-13.9 mg/dL | Urgent investigation + treat if symptomatic |
| Severe / Hypercalcemic crisis | ≥14 mg/dL | Emergency treatment regardless of symptoms |
Sources:
- Tietz Textbook of Laboratory Medicine, 7th Ed., Figs. 54.6A & B - Investigation algorithms for hypercalcemia
- Goldman-Cecil Medicine, Fig. 227 - Clinical approach diagram
- Textbook of Family Medicine, 9th Ed., Tables 35-22 to 35-24
- Brenner & Rector's The Kidney, Fig. 42.4 & 42.5
This is a shared conversation. Sign in to Orris to start your own chat.