Heat coagulation - pathology
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Searching Images
coagulative necrosis histology pathology
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have all the key content. Here is a comprehensive pathology overview of heat coagulation.
Heat Coagulation — Pathology
1. Mechanism: Why Heat Causes Coagulation
Thermal burns result from exposure to heat energy. Higher temperatures (starting as low as 41°C) denature cellular proteins. This protein denaturation affects both structural proteins (cytoskeletal elements, extracellular matrix) and enzymatic proteins (including the very proteases that would normally dissolve dead cells). The net result is that dead cells are "fixed in place" — a process called coagulative necrosis.
The critical insight from Robbins: "the injury denatures not only structural proteins but also enzymes, and so blocks the proteolysis of the dead cells." This is why the tissue architecture is paradoxically preserved even as cells are dead.
— Robbins, Cotran & Kumar: Pathologic Basis of Disease
2. Coagulative Necrosis — Pathological Features
Coagulative necrosis is the dominant form of cell death caused by heat (thermal) injury:
| Feature | Detail |
|---|---|
| Tissue architecture | Preserved for days to weeks after injury |
| Cell texture | Firm ("cooked" appearance) |
| Histology | Intensely eosinophilic (pink) cells; nuclei become pyknotic then disappear (anucleate ghost cells) |
| Cell outlines | Preserved but cytoplasm deeply eosinophilic |
| Eventual fate | Leukocytes infiltrate and lysosomal enzymes digest the debris; phagocytosis clears it |
On H&E: anucleate, eosinophilic "ghost" cells with intact cellular outlines but no viable nuclear detail — this is the hallmark.
3. Jackson's Thermal Wound Theory — Three Zones of Burn Injury
Heat does not produce a uniform injury. Jackson's model (1953) describes three concentric zones:
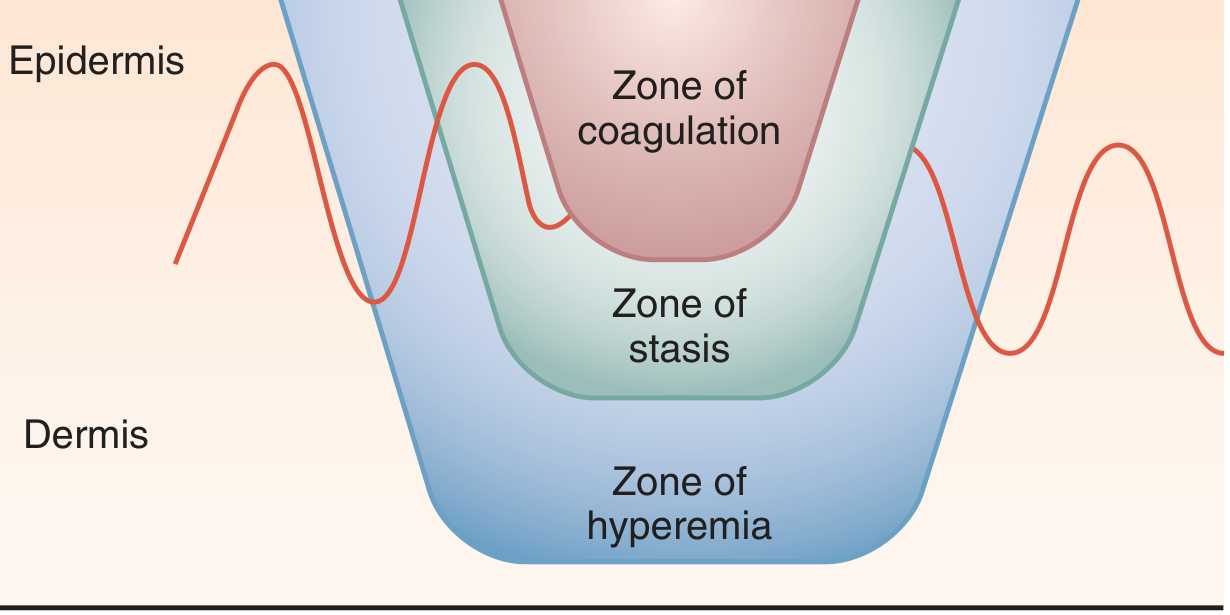
Zones of injury after a burn (Roberts & Hedges' Clinical Procedures in Emergency Medicine)
| Zone | Pathology | Clinical Significance |
|---|---|---|
| Zone of coagulation (centre) | Irreversible cell death; avascular; confluent coagulative necrosis | Must be debrided (eschar) |
| Zone of stasis (middle) | Impaired blood flow; cells injured but potentially viable | Can recover or progress to necrosis with desiccation, infection, or mechanical trauma |
| Zone of hyperemia (periphery) | Minimally injured; vasodilation and inflammation | Resolves in 7–10 days; can be mistaken for cellulitis |
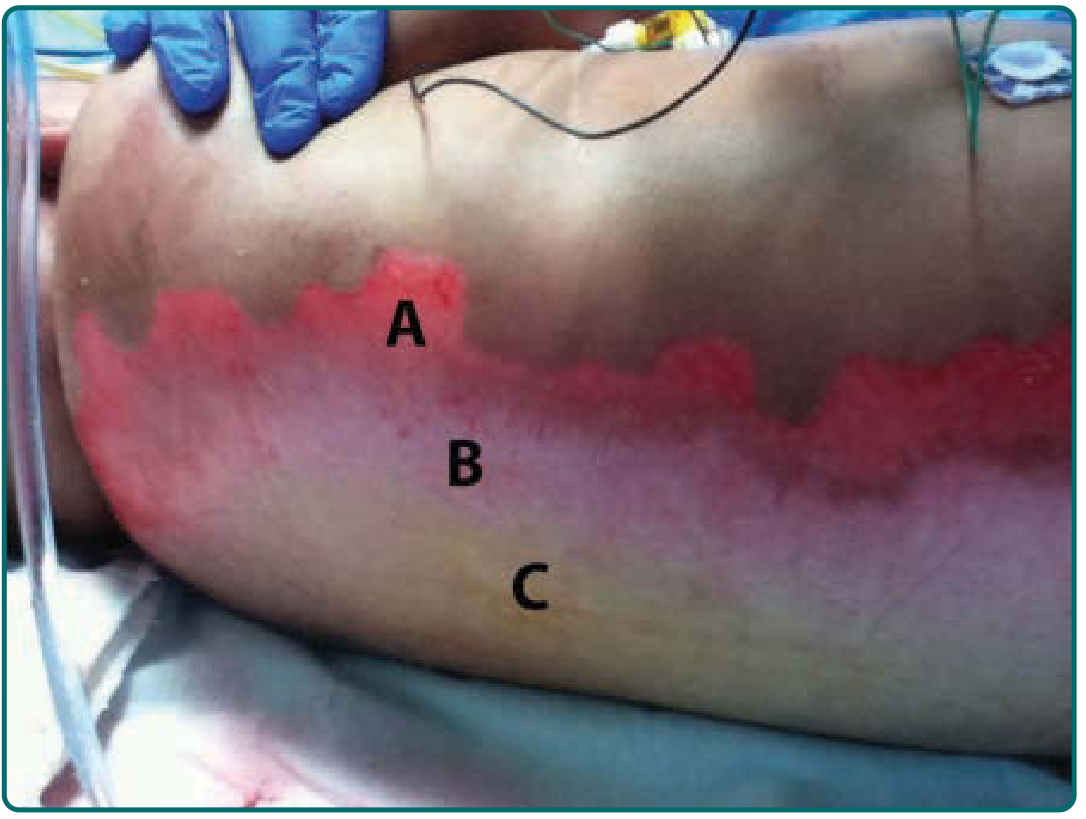
Full-thickness burn of the back demonstrating zones of injury (Fitzpatrick's Dermatology)
4. Histopathology of Burns in Depth
Full-thickness burns show:
- Confluent vascular thrombosis involving arterioles, venules, and capillaries
- Microvascular edema from direct thermal injury + release of vasoactive mediators (histamine, complement activation)
- Histamine activates xanthine oxidase → H₂O₂ and hydroxyl radicals → progressive vascular permeability and endothelial damage
- The eschar (denatured protein + cellular debris) provides a substrate for microbial proliferation
- Eschar sloughs spontaneously via bacterial proteolytic enzymes; bacteriostasis delays sloughing
Cellular mechanisms in the different zones include necrosis/necroptosis (with strong inflammatory response), autophagy (possibly protective), and early or delayed apoptosis (less inflammatory).
— Rosen's Emergency Medicine
5. Depth Classification and Correlation with Coagulation
| Burn Depth | Layers Involved | Heat Coagulation Pattern |
|---|---|---|
| Superficial (1st degree) | Epidermis only | Mild protein denaturation; no true coagulative necrosis |
| Superficial partial-thickness (2nd degree) | Epidermis + papillary dermis | Blistering; partial coagulative necrosis of upper dermis |
| Deep partial-thickness (2nd degree) | Down to reticular dermis | Deeper coagulative necrosis; high scar risk |
| Full-thickness (3rd degree) | All dermal layers + subcutaneous | Complete coagulative necrosis through dermis; insensate, leathery/eschar |
| 4th degree | Extends to muscle, tendon, bone | Charring; irreversible coagulative necrosis of all tissue planes |
6. Coagulative Necrosis vs. Other Forms of Necrosis
Heat-induced coagulative necrosis is best understood by contrast:
| Type | Cause | Architecture | Key Feature |
|---|---|---|---|
| Coagulative (heat, ischemia) | Protein denaturation blocks proteolysis | Preserved | Ghost cells, eosinophilic |
| Liquefactive | Bacterial enzymes / CNS hypoxia | Obliterated | Pus formation |
| Caseous | Tuberculosis | Obliterated | Friable, cheese-like; granuloma |
| Fat necrosis | Pancreatic lipases / trauma | Fat cells | Chalky white (saponification) |
| Fibrinoid | Immune complex vasculitis | Vessel wall | Bright pink, fibrin-like |
— Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease
Key Points Summary
- Heat ≥41°C denatures both structural and enzymatic proteins → coagulative necrosis
- Coagulative necrosis = preserved architecture, eosinophilic ghost cells, no nuclear detail
- Burns produce three concentric zones: coagulation (irreversible) → stasis (reversible) → hyperemia (recovers)
- Full-thickness burns show confluent vascular thrombosis, edema, and eschar formation
- The zone of stasis is the clinical target — preventing it from converting to coagulation is a major goal of burn management
This is a shared conversation. Sign in to Orris to start your own chat.