Urological trauma urology topic
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed for a comprehensive, well-structured answer. Let me compile it.
Urological Trauma - A Comprehensive Overview
Genitourinary (GU) organs are injured in approximately 5-10% of all trauma cases. Despite their relatively protected anatomical position, significant urological injuries are common in high-energy trauma and are frequently associated with other injuries. The full urinary tract - kidneys, ureters, bladder, urethra, and external genitalia - can each be involved.
1. Renal Trauma
Epidemiology and Mechanisms
The kidney is the most commonly injured GU organ. Injury mechanisms are blunt (most common: MVAs, falls, sports) and penetrating (stab/gunshot wounds). Children are anatomically more susceptible due to relatively larger kidneys and less perirenal fat. Penetrating injury to the flank carries a much higher incidence of renal vascular injury than blunt mechanisms.
Iatrogenic causes include PCNL (the most common iatrogenic cause, 0.9-3% of cases), renal biopsy, endopyelotomy, and open abdominal or endovascular surgery.
Clinical Features
- Flank pain, contusions, or ecchymosis
- Palpable flank mass or lower rib fractures
- Hematuria - the cardinal finding, but note: up to 50% of renal vascular/hilar injuries have no hematuria. Gross hematuria is more significant than microscopic.
- Microscopic hematuria alone after blunt trauma does not mandate imaging
Imaging
The gold standard is CT with IV contrast + delayed images (CT urogram), which delineates the collecting system, parenchyma, and vasculature.
Indications for CT imaging:
- Gross hematuria
- Microscopic hematuria + hypotension
- Significant deceleration mechanism, flank contusion, penetrating flank wound
AAST Renal Injury Grading System
| Grade | Description | Management |
|---|---|---|
| 1 | Contusion or non-enlarging subcapsular hematoma | Conservative |
| 2 | Perinephric hematoma without parenchymal laceration, or <1 cm cortical laceration | Conservative (stable patient) |
| 3 | >1 cm cortical laceration without collecting system involvement | Conservative (stable patient) |
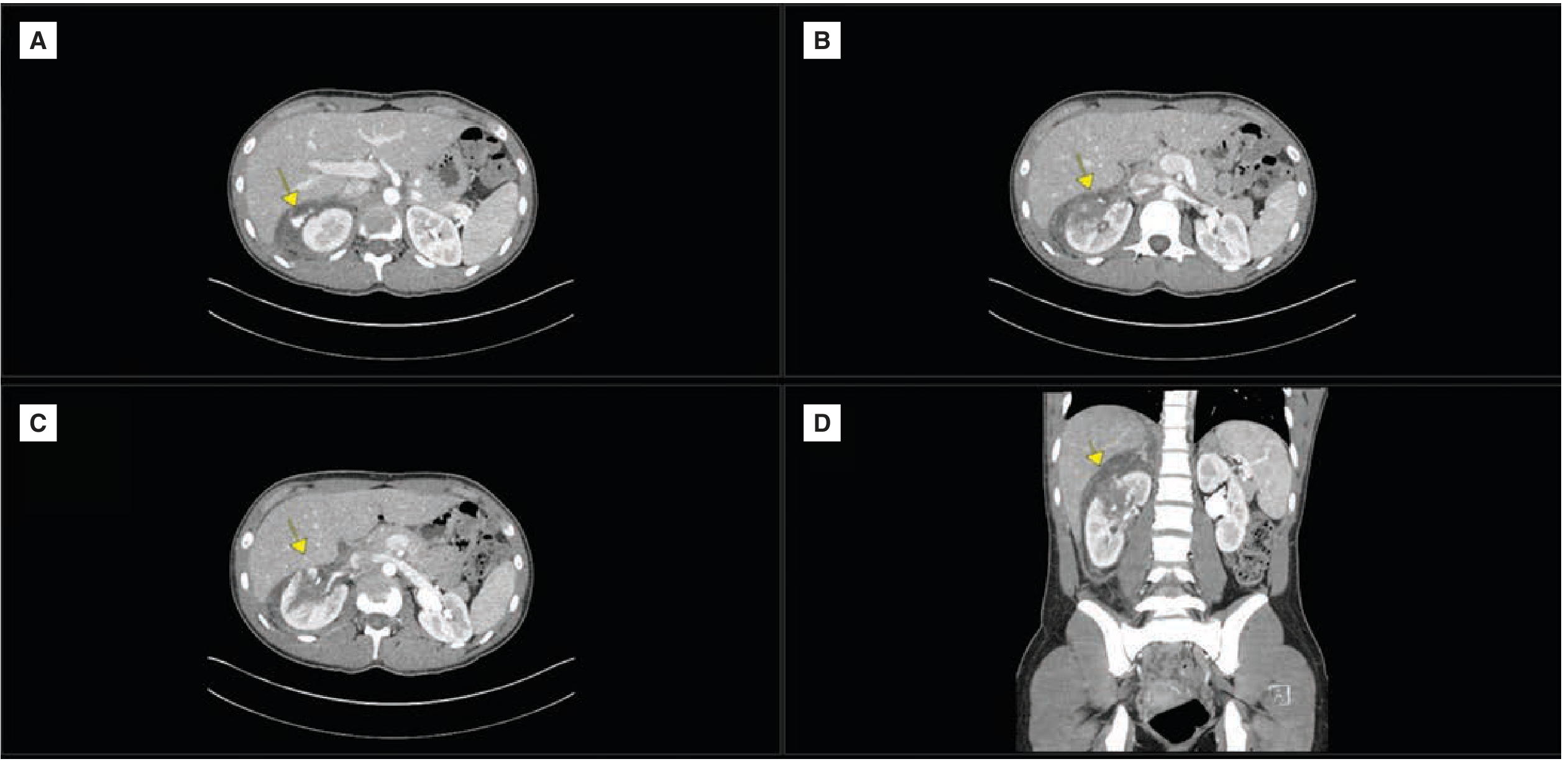
| 4 | Deep laceration into collecting system with urinary extravasation; OR segmental artery/vein injury, partial vessel laceration, vessel thrombosis | Expectant observation; may need urgent/delayed repair; angioembolization option |
| 5 | Renal pedicle injury ("shattered kidney"), multiple deep lacerations | Often surgical; stable patients with only parenchymal injury may be observed |
(Source: Schwartz's Principles of Surgery, 11th Ed.; Campbell-Walsh-Wein Urology)
Below is a representative CT image of a Grade 4 renal injury (arrows indicating laceration with perirenal hematoma):
Management
Conservative (non-operative) is the primary approach for the vast majority of renal injuries, including many high-grade injuries, in hemodynamically stable patients.
- Bed rest, hemodynamic monitoring
- Grade 4: repeat CT to confirm resolution of urinary extravasation; if persistent, ureteral stent or nephrostomy tube
- Grade 5 (stable, parenchymal only): may still be managed conservatively
Absolute indications for surgical/radiological intervention:
- Life-threatening hemorrhage
- Renal pedicle avulsion
- Pulsatile or expanding retroperitoneal hematoma
- Penetrating renal trauma + hemodynamic instability
Angioembolization (interventional radiology) is preferred over open surgery for vascular bleeding when possible, as it decreases renal parenchymal loss and morbidity. AUA guidelines recommend immediate intervention (surgery or angioembolization) only in hemodynamically unstable patients or those only transiently responsive to resuscitation.
Surgery (nephrorrhaphy / nephrectomy): When open exploration is required, early renal vascular control is obtained medially before opening the hematoma. Nephrorrhaphy where possible; nephrectomy for Grade 5 or uncontrollable bleeding.
Complications of renal trauma: Urinoma, abscess, hypertension (recognized late sequel - patients need regular BP monitoring), arteriovenous fistula.
2. Ureteral Trauma
Features
- No reliable correlation between degree of hematuria and severity of ureteral injury
- The ureter is more commonly injured iatrogenically than traumatically
- Common surgical procedures involved: gynecological, colorectal, and urological surgeries
- High index of suspicion is required
Diagnosis
- CT urogram (with delayed images)
- Intravenous pyelogram (IVP)
- Cystoscopy + retrograde pyelogram
Management
| Situation | Management |
|---|---|
| Iatrogenic, identified early | Ureteral stent placement (first-line) |
| Stenting not feasible, early presentation | Open repair |
| Delayed presentation, stenting not feasible | Nephrostomy tube placement, then delayed repair |
| Traumatic origin (penetrating), stable patient | Primary repair at index laparotomy |
| Hemodynamically unstable | Ligate ureter + nephrostomy tube; delayed repair when stable |
Repair technique depends on time since injury, location, and length of injured segment.
3. Bladder Trauma
Causes
Traumatic:
- Direct compression of a full bladder (RTA, fall, kick - often with alcohol)
- Associated with pelvic fractures (15% have concomitant urethral trauma)
Iatrogenic: Gynaecological surgery, colorectal surgery, urological surgery (TURBT, bladder biopsy), radiotherapy (e.g., post-cervical cancer radiation)
Types of Rupture
Intraperitoneal rupture:
- Follows direct violence to a full bladder
- Typically a longitudinal midline tear
- Presents with lower abdominal pain, tenderness, and features of peritonitis
- Diagnosis: CT cystogram or IVU showing intraperitoneal contrast extravasation
- Treatment: Open exploration (lower midline incision), two-layer non-absorbable suture closure, urethral catheter drainage for 10-14 days
Extraperitoneal rupture:
- Associated with pelvic fractures, usually RTA or crush injuries
- Haematuria or anuria (if combined urethral injury), blood at penile meatus
- Diagnosis: CT/cystogram; flexible cystoscopy under lignocaine if needed (supine, no GA required)
- Treatment: Small fresh rupture (<1 cm) without appreciable extravasation may be managed with urethral catheterization for 14 days + endoscopic check. All others require open repair, retroperitoneal drainage, urethral or suprapubic catheter for 10-14 days.
Indications for surgical repair of bladder injury:
- Urinary catheter not providing adequate drainage
- Associated rectal or vaginal injury
- Associated bladder neck injury
- Open pelvic fracture fixation (to avoid hardware contamination)
- Pelvic fracture with bone spicules in bladder lumen
4. Urethral Trauma
Urethral injuries are classified as anterior (bulbar/penile) or posterior (prostatic/membranous) - an important distinction because mechanisms, comorbid injuries, and management differ.
Posterior Urethral Injuries
- Involve the prostatic and membranous urethra
- Mechanism: major blunt deceleration (MVA, falls) causing shearing at the prostato-membranous junction
- Occur in 4-6% of pelvic fractures
- Classic triad: urinary retention + blood at urethral meatus + high-riding prostate
- For every 1 mm of symphysis pubis diastasis or inferomedial pubic bone fracture displacement, urethral injury risk increases by ~10%
Anterior Urethral Injuries
- Involve bulbar (more common) or penile urethra
- Mechanism: straddle injury (fall astride bicycle bar, manhole edge, fence), direct perineal blow, penetrating trauma, or penile fracture
- Bulbar segment most commonly affected
- May be missed initially and present later as urethral stricture
Diagnosis
- Retrograde urethrogram (RUG): Gold standard - inject 20-30 mL contrast, look for extravasation
- Partial laceration: extravasation at injury site + contrast seen proximal to it
- Complete laceration: extravasation at injury site with no proximal contrast
- Important: Perform RUG before CT if pelvic arterial embolization is being considered, as contrast can interfere. Discuss sequencing with the trauma team.
- Never forcibly insert a Foley catheter if urethral injury is suspected
Management
| Injury Type | Management |
|---|---|
| Posterior urethral injury (pelvic fracture) | Suprapubic catheter (immediate) + delayed surgical repair (weeks later) - avoids urethral manipulation and hematoma disruption |
| Anterior urethral penetrating | Surgical exploration and repair |
| Bulbar blunt (partial) | May be managed with urethral catheterization alone |
| Female urethral injuries | Urethroscopy preferred; concurrent bladder injury must be excluded with CT cystography |
Complications if missed or poorly managed: Urethral stricture, impotence, urinary incontinence, erectile dysfunction.
5. External Genital Trauma
Penile Injuries
- Penile fracture: Corpus cavernosum rupture from forcible bending (usually during intercourse). Hallmark: cracking sound, rapid swelling, discoloration, "eggplant deformity." Treat with immediate surgical repair.
- Amputation: Usually self-inflicted or industrial machinery. Reimplantation possible if prompt.
- Vacuum cleaner injuries: Extensive injury to glans and urethra.
- Strangulation injuries: From constricting rings used to enhance erections.
Scrotal and Testicular Injuries
-
50% of testicular trauma results from sporting activity
- Scrotal injuries: blunt, penetrating, burns, avulsions
- Ultrasound is the imaging of choice to assess for testicular rupture
- Significant blunt testicular trauma with suspected rupture: surgical exploration and repair
Physical Examination Key Points
- Inspect perineum during secondary survey
- Blood at the urethral meatus - suspect urethral injury
- High-riding or boggy prostate on rectal exam - presume membranous urethral disruption until proven otherwise
- In females: examine vaginal introitus for lacerations, hematomas (associated with pelvic fractures); missed vaginal injuries can lead to incontinence, fistula, or hemorrhage
- Never deeply probe perineal injuries (risks clot disruption)
6. Initial Assessment Principles
- Primary survey (ATLS): Airway, Breathing, Circulation first - GU trauma rarely takes precedence over life-threatening injuries
- History: Mechanism, forces involved, restraint use, ability to void, pre-existing GU dysfunction
- Urinalysis: Always obtain; gross hematuria = significant; microscopic hematuria alone in blunt trauma is a lower-yield finding
- CT with IV contrast + delayed phases is the cornerstone of upper GU injury staging
- Retrograde urethrogram before Foley placement if urethral injury is suspected
- Cystogram for bladder injury
- Children are at higher risk due to anatomy; multiorgan injuries are the rule
7. Special Populations
Elderly patients:
- More likely blunt trauma (falls are a leading cause; 26.5% GU injury rate from falls vs. 8.4% in younger adults)
- Higher comorbidity burden; greater use of embolization over surgery
- Higher rates of discharge to rehabilitation or nursing facilities
- Osteoporosis increases pelvic fracture risk and associated urethral/bladder injuries
Summary Table
| Structure | Classic Mechanism | Key Diagnostic Test | Primary Management |
|---|---|---|---|
| Kidney | Blunt deceleration, flank blow | CT urogram | Conservative (most); angioembolization; surgery if unstable |
| Ureter | Iatrogenic (gyne/colorectal/uro surgery) | CT urogram / retrograde pyelogram | Ureteral stent; open repair; nephrostomy |
| Bladder | Pelvic fracture; full-bladder direct blow | CT cystogram / IVU | Catheter drainage (small extra); open repair (intraperitoneal/large) |
| Urethra (posterior) | Pelvic fracture, deceleration | Retrograde urethrogram | Suprapubic catheter + delayed repair |
| Urethra (anterior) | Straddle injury, penetrating | Retrograde urethrogram | Surgical repair (penetrating); catheter (partial blunt) |
| Penis | Sexual intercourse (fracture), machinery | Clinical diagnosis | Immediate surgical repair |
| Testis | Sports impact | Scrotal ultrasound | Surgical exploration if rupture suspected |
Sources:
- Schwartz's Principles of Surgery, 11th Ed., Ch. 40
- Tintinalli's Emergency Medicine, Ch. 265
- Campbell-Walsh-Wein Urology, 12th Ed.
- Pye's Surgical Handicraft, 22nd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.