acute glomerulonephritis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute glomerulonephritis"[MeSH Terms]
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content. Let me synthesize a complete, well-organized answer.
Acute Glomerulonephritis (AGN)
Acute glomerulonephritis (AGN) refers to a syndrome of sudden-onset inflammation of the glomeruli, most classically presenting as the nephritic syndrome. The paradigmatic and most common form is acute poststreptococcal glomerulonephritis (PSGN).
Definition & Nephritic Syndrome
The hallmark presentation — nephritic syndrome — consists of:
| Feature | Mechanism |
|---|---|
| Hematuria (gross or microscopic) | Capillary wall injury → RBC leakage |
| Oliguria / reduced GFR | Glomerular inflammation → ↓ filtration |
| Azotemia | Impaired filtration + fluid retention |
| Hypertension | Fluid retention + renin release from ischemic kidneys |
| Edema (periorbital, facial, peripheral) | Na⁺ and water retention |
| Proteinuria (mild–moderate) | Capillary wall damage |
— Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 839
Etiology
While streptococcal infection is the classic cause, AGN has many triggers:
Bacterial:
- Group A β-hemolytic Streptococcus (pharyngitis or impetigo) — nephritogenic strains: M types 1, 4, 12, 49, and others
- Staphylococcus (especially in older adults with active infection)
- Pneumococcus, infective endocarditis (subacute bacterial endocarditis)
Viral: Hepatitis B and C, mumps, measles, varicella (chickenpox)
Other GN types with acute presentation: IgA nephropathy, lupus nephritis (class III/IV), MPGN, crescentic (rapidly progressive) GN
— Robbins & Kumar Basic Pathology, p. 510; Brenner and Rector's The Kidney, p. 1378
Epidemiology (PSGN)
- Peak incidence: children 2–10 years of age; males more frequently than females
- Adults >40 years and children <2 years account for only ~15% of cases
- Subclinical disease (microscopic hematuria) is 4× more common than overt AGN
- Clinical attack rate during epidemic streptococcal infections: ~12–38%
- On the decline in developed countries due to early antibiotic therapy; >90% of cases now occur in lower-income countries
- Cyclic outbreaks roughly every 10 years in endemic regions
— Brenner and Rector's The Kidney, p. 1378
Pathogenesis
PSGN is an immune complex-mediated disease:
- Nephritogenic streptococci (typing via M protein) secrete streptococcal pyogenic exotoxin B (SpeB) — the principal antigen in most cases
- SpeB is exogenously planted in subendothelial locations → in situ immune complex formation (IgG + antigen)
- Complexes activate complement (predominantly the alternative and lectin pathways; C3 and properdin ↓, C1q/C2/C4 relatively preserved)
- Complexes later migrate across the GBM to the subepithelial space, forming the characteristic "humps"
- Complement activation → neutrophil and monocyte infiltration → glomerular injury
Evidence supporting immune basis:
- Latent period (7–21 days) = time for antibody production
- ↑ Anti-streptolysin O (ASO) titers in majority of patients
- Hypocomplementemia (↓ CH-50, ↓ C3)
- Granular immune deposits on immunofluorescence
— Robbins, Cotran & Kumar, p. 840; Brenner and Rector's The Kidney, p. 1379
Morphology (Biopsy)
Light Microscopy
Diffuse endocapillary hypercellularity affecting virtually all glomeruli — proliferation of endothelial and mesangial cells plus infiltrating neutrophils and monocytes. Occasional necrosis of capillary walls. Crescents may be seen in severe cases.
Immunofluorescence
Granular ("starry sky") deposits of IgG and C3 along capillary walls and in mesangium — coarsely granular pattern.
Electron Microscopy
Characteristic subepithelial electron-dense "humps" (deposits nestled against the GBM). Subendothelial and intramembranous deposits also present. Deposits clear over ~2 months after resolution.
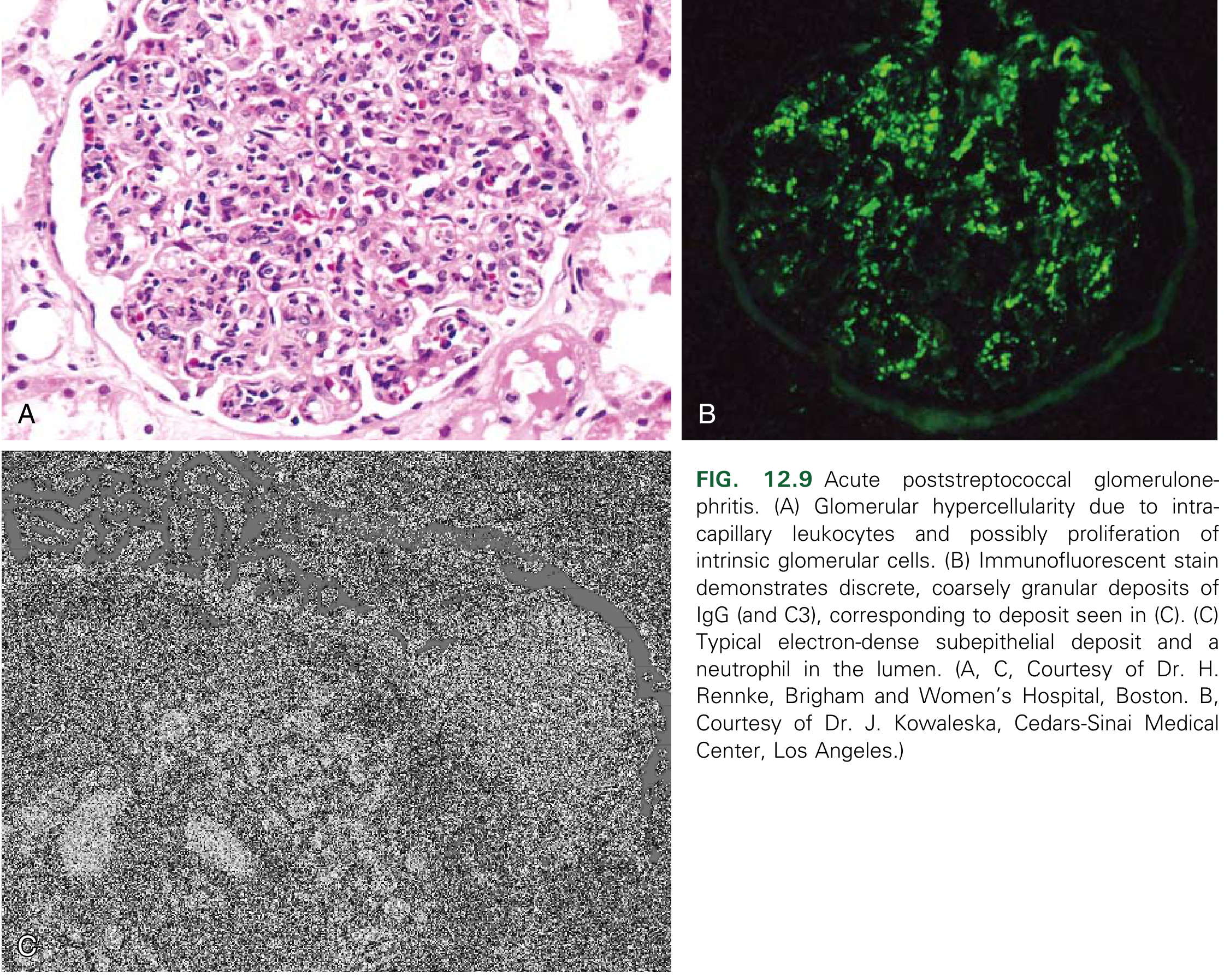
Fig. 12.9 — Robbins & Kumar Basic Pathology
Clinical Features
Latent period:
- Post-pharyngitis: 7–21 days (average 10 days)
- Post-impetigo: 14–21+ days
Symptoms and signs:
- Hematuria: microscopic in >2/3 of cases; gross ("cola-colored" urine) in ~1/3
- Edema: presenting symptom in ~2/3; present in up to 90% — facial/periorbital predominance
- Hypertension: mild-to-moderate in >75%; usually resolves with diuresis
- Azotemia / oliguria: GFR decline common, especially in adults >55 years (~60%)
- Proteinuria: mild–moderate; occasionally nephrotic-range
- Encephalopathy (confusion, headache, convulsions): uncommon but more frequent in children
- Heart failure symptoms: in up to 40% of older patients (jugular venous distention, S3 gallop, pulmonary congestion)
— Brenner and Rector's The Kidney, p. 1381
Laboratory Findings
| Test | Expected Finding |
|---|---|
| Urinalysis | Hematuria, dysmorphic RBCs, RBC casts (pathognomonic), leukocytes, granular casts |
| Serum creatinine / BUN | Elevated (azotemia) |
| Serum C3, CH-50 | Decreased (returns to normal within 6–8 weeks) |
| C1q, C2, C4 | Normal or mildly reduced (alternative + lectin pathway activation) |
| ASO titer | Elevated in ~90% with pharyngeal infection; ~1/3 with impetigo |
| Anti-DNase B, antihyaluronidase | Better markers for skin infection-associated PSGN |
| Throat/skin culture | Positive in as few as 25% of patients |
| Serum potassium | Mild hyperkalemia (transient hyporeninemic hypoaldosteronism) |
| Urinary sodium & calcium | Markedly reduced |
Key complement pattern: ↓ C3 + ↓ CH-50, with normal/near-normal C1q, C2, C4 → points to alternative/lectin pathway activation
Complement levels normalize within 8 weeks — failure to normalize should prompt search for other diagnoses (e.g., MPGN, lupus, C3 glomerulopathy).
Differential Diagnosis
- IgA nephropathy — no latent period; hematuria appears during/immediately after infection ("synpharyngitic")
- IgA vasculitis (Henoch-Schönlein purpura) — purpuric rash, arthritis, abdominal pain
- MPGN / C3 glomerulopathy — complement does not normalize
- Rapidly progressive (crescentic) GN — persistent anuria/oliguria, rapidly worsening renal function
- Lupus nephritis — ↓ C3 AND ↓ C4, positive ANA/anti-dsDNA
- Infective endocarditis-associated GN — consider if fever persists
Treatment & Prognosis
Treatment is largely supportive:
- Antibiotics (penicillin): treat residual streptococcal infection; do not alter the course of nephritis but reduce spread to contacts
- Salt and fluid restriction + loop diuretics: for edema and hypertension
- Antihypertensives: needed in ~50% of patients
- Dialysis: rarely required; reserved for severe AKI, severe hyperkalemia, or pulmonary edema unresponsive to diuretics
Prognosis:
-
95% of children recover fully with spontaneous resolution within 1–2 weeks (edema, hypertension)
- Microscopic hematuria and proteinuria may persist for months but usually resolve within 1 year
- In adults, prognosis is less favorable — higher rates of persistent proteinuria, hypertension, and progression to CKD
- Crescentic transformation → worse prognosis, requires aggressive immunosuppression
— Robbins & Kumar Basic Pathology, p. 510; Brenner and Rector's The Kidney, pp. 1381–1382
Summary Table
| Feature | PSGN |
|---|---|
| Pathogenesis | Immune complex (IgG + SpeB) → complement activation |
| Pattern | Diffuse endocapillary proliferative GN |
| IF | Granular IgG + C3 ("starry sky") |
| EM | Subepithelial "humps" |
| Complement | ↓ C3, ↓ CH-50; normal C4 |
| Latent period | 1–3 weeks |
| Prognosis | Excellent in children; guarded in adults |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology; Brenner and Rector's The Kidney
This is a shared conversation. Sign in to Orris to start your own chat.