Explain myasthenia gravis
Reading File
Finding Sources
Searching PubMed
"myasthenia gravis"[MeSH Terms] AND treatment
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I have thorough coverage across all major domains. I can now compile the full, well-cited answer.
Myasthenia Gravis - A Comprehensive Overview
Definition
Myasthenia gravis (MG) is the most common primary disorder of neuromuscular transmission (NMT). Autoantibodies bind to proteins at the postsynaptic neuromuscular junction (NMJ) - most commonly the nicotinic acetylcholine receptor (AChR) - disrupting the conversion of nerve impulses into muscle fiber action potentials. The result is fatigable muscle weakness that worsens with activity and improves with rest.
- Bradley and Daroff's Neurology in Clinical Practice, p. 2770
Epidemiology
-
US prevalence: ~20/100,000 (approx. 60,000 patients)
-
Prevalence has increased over the past 50 years (better ascertainment, reduced mortality, aging population)
-
Sex and age pattern: Women are affected ~3x more often than men before age 40; incidence is higher in males after age 50; roughly equal during puberty
-
Today, the majority of US MG patients are over age 50 and more men are now affected than women overall
-
Bradley and Daroff's Neurology in Clinical Practice, p. 2770
Pathophysiology
The NMJ has no blood-nerve barrier, making it uniquely vulnerable to circulating immune factors. Three antibody mechanisms have been described:
| Antibody Target | Mechanism | Prevalence |
|---|---|---|
| AChR (alpha-1 subunit) | Complement activation destroying the postjunctional membrane; antigenic modulation (cross-linking + receptor internalization); direct functional blockade | ~85% of generalized MG |
| MuSK (muscle-specific kinase) | IgG4 antibodies inhibit clustering of AChRs on the postsynaptic surface | Up to 50% of AChR-negative generalized MG |
| LRP4 (lipoprotein receptor-related protein 4) | Interferes with signals maintaining NMJ integrity | Minority; less well understood |
| Seronegative | No detectable antibodies by standard testing | ~10% |
The net result is a reduced density of functional AChRs at the motor endplate. With repeated nerve stimulation, the normal presynaptic quantal release of ACh decrements against a shrinking pool of available receptors, producing the characteristic fatigable weakness.
The thymus is central to pathogenesis:
-
Early-onset MG (mostly women): thymic hyperplasia with active germinal centers suggests a thymus-initiated breakdown in immune tolerance
-
Thymoma-associated MG (~10-15% of patients): deficiency of the autoimmune regulatory protein AIRE leads to reduced regulatory T cells and increased autoreactivity
-
There is also a genetic component - ~5% of patients have an affected family member, with a heritability index of 0.65
-
Goldman-Cecil Medicine, p. 4111; Bradley and Daroff's Neurology in Clinical Practice
Clinical Presentation
Cardinal Features
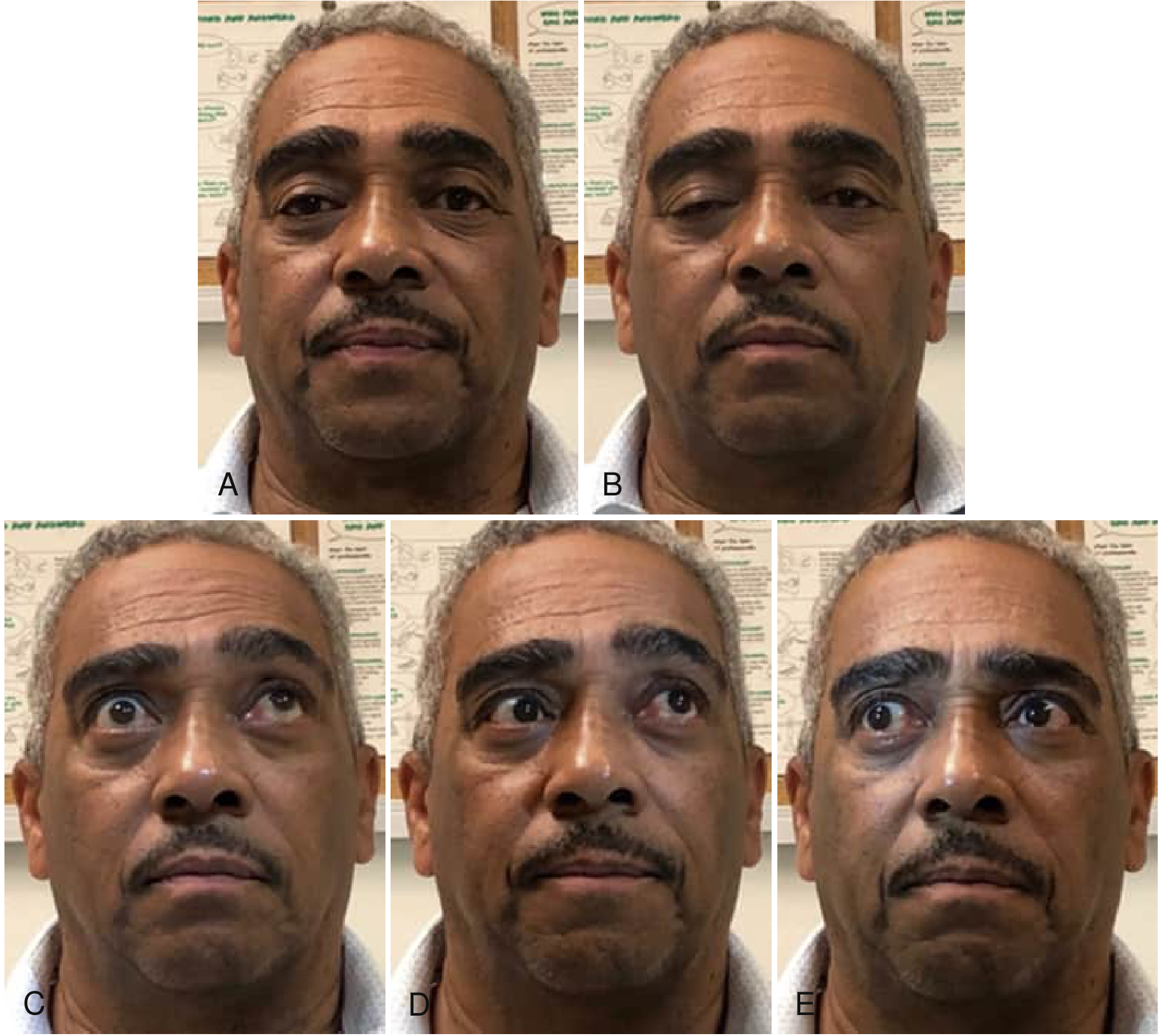
Fig: Ocular motility abnormalities in MG. A-B: Progressive right lid ptosis on sustained forward gaze. C: Incomplete superior movement on attempted upward gaze. D-E: Skew deviation and incomplete lateral gaze from multiple periocular muscle weakness. (Bradley and Daroff's Neurology in Clinical Practice)
- Ptosis and/or diplopia are the initial symptoms in up to 85% of patients; nearly all develop both within 2 years
- Weakness worsens with activity and improves with rest; typically least severe in the morning
- Bulbar symptoms (dysphagia, dysarthria, jaw fatigue) affect up to 30% at onset
- Limb weakness (proximal > distal) occurs in ~10% at onset
- Respiratory muscles can be involved - leading to myasthenic crisis
Distribution Patterns by Subtype
| Subtype | Key Features |
|---|---|
| Ocular MG (OMG) | Confined to ocular muscles; 10-15% in Caucasians, up to 58% in Asian populations; if ocular only after 2 years, 90% chance it won't generalize |
| Early-onset generalized (EOMG) | Women, <50 y, AChR-Ab+, thymic hyperplasia |
| Late-onset generalized (LOMG) | Men, >50 y, AChR-Ab+, normal/atrophic thymus; anti-titin and anti-ryanodine receptor Abs common; more crises |
| MuSK-MG | Predominantly female; prominent bulbar/facial/neck/respiratory weakness; often muscle atrophy; may worsen with pyridostigmine |
| Thymoma-associated | Equal sex; peak onset ~50 y; striated muscle Abs common |
- Bradley and Daroff's Neurology in Clinical Practice, p. 2771-2774
Diagnosis
1. Clinical recognition: Fatigable weakness in a characteristic distribution - ptosis worsening on sustained upgaze, fatigable proximal limb weakness, bulbar findings.
2. Serological testing:
- AChR antibodies (binding, blocking, modulating) - positive in ~85% of generalized MG, ~50% of ocular MG
- MuSK antibodies - checked when AChR-Ab negative
- LRP4 antibodies - emerging test
3. Edrophonium (Tensilon) test: IV injection of this short-acting acetylcholinesterase inhibitor produces transient improvement in ocular or bulbar weakness; now less used due to cardiac risks.
4. Electrodiagnostic studies:
- Repetitive nerve stimulation (RNS): Decremental response (>10% decrement) at 3 Hz is characteristic
- Single-fiber EMG (SFEMG): Most sensitive test; increased "jitter" reflects variable NMJ transmission; required when RNS and antibodies are negative (especially in OMG)
5. Imaging:
-
CT or MRI of chest to detect thymoma or thymic hyperplasia - required in all newly diagnosed MG patients
-
Wills Eye Manual; Bradley and Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine
Myasthenic Crisis
A myasthenic crisis is respiratory failure from respiratory or oropharyngeal muscle weakness requiring ventilatory support. It is a medical emergency. Common triggers include:
- Infection (especially respiratory)
- Aspiration/dysphagia (precipitant in 56% of crises in one study)
- Medication errors or non-compliance
- Aminoglycosides, fluoroquinolones, beta-blockers, magnesium, neuromuscular blocking agents (all can worsen MG)
- Surgery, pregnancy, stress
Management requires ICU admission, ventilatory support, plasmapheresis or IVIg (begin before high-dose steroids to prevent early steroid-associated worsening), and treatment of the underlying trigger.
Treatment
Treatment is individualized by extent (ocular vs. generalized) and severity. The goal defined by the MG Foundation of America Task Force: "no symptoms or functional limitations from MG, with no more than mild side effects requiring no intervention."
1. Symptomatic: Cholinesterase Inhibitors (ChEIs)
- Pyridostigmine (Mestinon): 30-60 mg orally every 4-8 hours; first-line symptomatic therapy for most patients
- Inhibits acetylcholinesterase, increasing ACh availability at the NMJ
- Muscarinic side effects: nausea, diarrhea, cramps, increased secretions - can be managed with glycopyrrolate
- Caution: MuSK-MG patients may worsen with ChEIs
2. Short-term Immunotherapy (rapid but transient benefit)
- Plasma exchange (plasmapheresis): Removes circulating antibodies; response within days; used pre-operatively, pre-thymectomy, and in crisis
- IVIg: Comparable efficacy to plasma exchange; mechanism includes Fc receptor saturation and immune modulation; given as 2 g/kg over 2-5 days
3. Long-term Immunosuppression
| Agent | Mechanism | Notes |
|---|---|---|
| Prednisone | Broad immunosuppression | First-line; start low (15-25 mg/d) and increase to 50-60 mg/d; taper slowly once controlled; watch for early worsening |
| Azathioprine | Purine synthesis inhibition | RCT evidence; steroid-sparing; onset 12+ months; check TPMT enzyme; avoid with allopurinol |
| Mycophenolate mofetil (MMF) | Selective lymphocyte purine synthesis inhibition | 1000-1500 mg twice daily; widely used; teratogenic - stop 4 months before pregnancy |
| Cyclosporine | Calcineurin inhibitor (inhibits IL-2) | RCT evidence; limited by nephrotoxicity and drug interactions |
| Tacrolimus | Calcineurin inhibitor | Approved for MG in Japan; useful in refractory cases; less nephrotoxic than cyclosporine |
| Rituximab | Anti-CD20 B-cell depletion | Particularly effective in MuSK-MG; a 2025 Cochrane review (PMID: 40607605) assessed its evidence base |
| Cyclophosphamide | Alkylating cytotoxic agent | Reserved for refractory cases; RCT evidence for pulse IV dosing |
4. Thymectomy
- Recommended for all patients with thymoma
- Also recommended for AChR-Ab+ generalized MG patients aged 18-65, even without thymoma (MGTX trial evidence)
- Effect is gradual - maximal benefit may not appear for years
5. Novel Biologics (emerging/approved)
Recent network meta-analyses (PMID: 40346603, PMID: 39470879) have evaluated newer agents:
- Eculizumab (complement C5 inhibitor): FDA-approved for refractory generalized AChR-Ab+ MG
- Efgartigimod (FcRn antagonist): Reduces IgG antibody levels by blocking neonatal Fc receptor recycling; FDA-approved
- Rozanolixizumab, nipocalimab: Also FcRn antagonists under study
- Zilucoplan: Subcutaneous complement C5 inhibitor; FDA-approved 2023
These agents represent a mechanistic shift from broad immunosuppression to targeted pathway blockade.
- Bradley and Daroff's Neurology in Clinical Practice, pp. 2775-2790; Harrison's Principles of Internal Medicine 22E, p. 3674
Prognosis
The prognosis has dramatically improved in the past 50 years due to advances in ICU care and immunotherapy. With modern treatment:
- The majority of patients achieve minimal manifestation status or complete stable remission
- Mortality from MG itself is now rare in specialized centers
- Spontaneous remission occurs in a subset, more common in early-onset ocular MG
- Patients with thymoma have a more guarded prognosis related to the underlying neoplasm
Summary Table: MG vs. Lambert-Eaton (key differential)
| Feature | Myasthenia Gravis | Lambert-Eaton Myasthenic Syndrome |
|---|---|---|
| Antibody target | AChR / MuSK / LRP4 | VGCC (voltage-gated calcium channel) |
| Weakness pattern | Ocular, bulbar, proximal limb | Proximal limb (legs >> arms); spares ocular |
| Fatigability | Worsens with use | Improves transiently with brief exercise |
| Reflexes | Normal | Reduced, may augment after exercise |
| RNS | Decremental at low frequency (3Hz) | Incremental at high frequency (>10Hz) |
| Autonomic features | Absent | Common (dry mouth, constipation) |
| Association | Thymic disease | Small cell lung cancer (60%) |
Recent evidence note: A 2025 Cochrane systematic review (PMID: 40607605) examined rituximab specifically in MG, and a 2025 network meta-analysis (PMID: 40346603) compared novel biologics (complement inhibitors, FcRn antagonists) - both informing the rapidly evolving treatment landscape for generalized MG.
This is a shared conversation. Sign in to Orris to start your own chat.