I now have comprehensive information from multiple authoritative textbooks and rich images. Let me compile the full detailed response.
Fibromyalgia Syndrome (FMS) - Comprehensive Orthopedic Review
Definition
Fibromyalgia (FM) is a chronic, widespread musculoskeletal pain syndrome characterized by central sensitization - an augmented processing of pain and sensory stimuli within the central nervous system - for which no alternative structural, inflammatory, or metabolic cause can be identified. It is now classified under the umbrella of "nociplastic pain" or "centralized pain", distinct from nociceptive and neuropathic pain.
The term was coined by Smythe and Moldofsky after Graham introduced the concept of "pain syndrome" in the absence of specific organic disease in 1950.
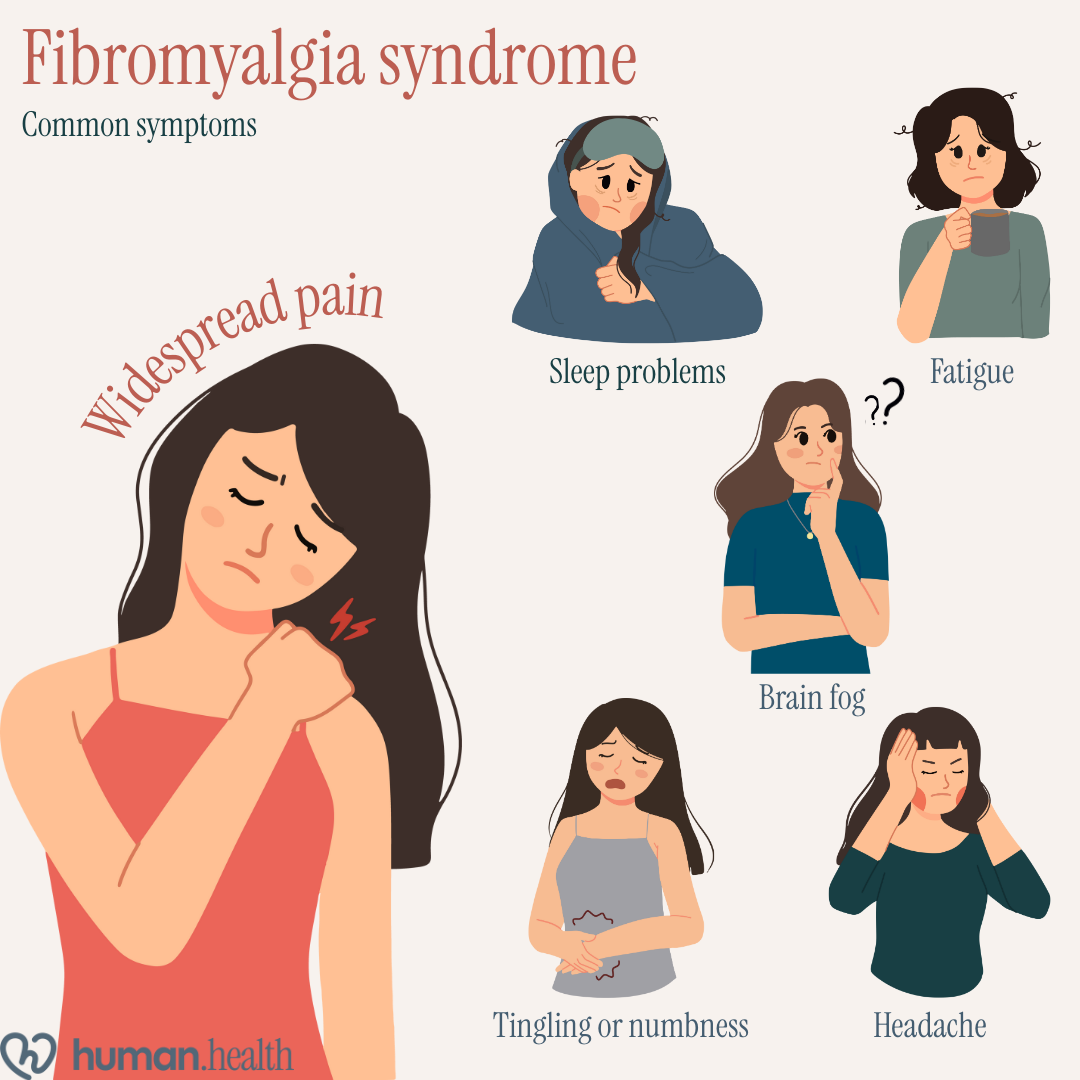
Figure: Common symptoms of fibromyalgia syndrome - widespread pain, sleep problems, fatigue, brain fog, tingling/numbness, and headache.
Epidemiology
| Parameter | Data |
|---|
| Prevalence (general population) | 2-8% worldwide |
| Chronic widespread pain (population) | 4-12% at any given time |
| Female:male ratio | Previously 9:1; revised to ~3:1 with modern criteria |
| Peak onset | Multiple age ranges; symptoms often begin in childhood/adolescence |
| Comorbidity with RA/OA/SpA | 15-25% of patients with inflammatory arthritis also have FM |
Etiology and Risk Factors
FM is a multifactorial disorder with no single causative agent. Etiology involves a complex interplay of genetic, neurobiological, psychological, and environmental factors.
Genetic Predisposition
- First-degree relatives of FM patients have an 8-fold higher risk
- Polymorphisms in serotonin transporter gene (5-HTT), COMT (catechol-O-methyltransferase), and dopamine receptor genes have been implicated
- Symptom clustering within families suggests heritable neurobiological traits
Triggering Factors (Environmental Stressors)
| Category | Examples |
|---|
| Physical trauma | Motor vehicle accidents, orthopedic injuries, surgeries |
| Infections | Viral illnesses (hepatitis C, HIV, Lyme disease, EBV) |
| Psychological stress | PTSD, physical/emotional abuse, adverse childhood events |
| Sleep disruption | Alpha-delta sleep anomaly (intrusion of alpha waves into Stage 4 sleep) |
| Hormonal changes | Menopause, dysmenorrhea |
| Inflammatory disease onset | RA, SLE, OA - can trigger FM-like centralization of pain |
Classification of Pain Mechanisms (Orthopedic Context)
| Pain Type | Cause | Clinical Feature |
|---|
| Nociceptive | Inflammation or tissue damage | Well localized; predictable with activity |
| Neuropathic | Nerve damage or entrapment | Dermatomal; burning/shooting |
| Centralized/Nociplastic (FM) | CNS dysregulation | Poorly localized; widespread; fatigue; cognitive issues |
Pathology and Pathophysiology
1. Central Sensitization - The Hallmark
The pathophysiologic hallmark of FM is augmented central pain processing. Patients are more tender everywhere in the body, not just at classic "tender points." This results from:
- Decreased activity of descending analgesic pathways (reduced serotonin and norepinephrine in the spinal cord)
- Increased excitatory neurotransmission - elevated CSF glutamate, substance P (3-fold elevated), and nerve growth factor
- Wind-up phenomenon - temporal summation of repeated painful stimuli causing progressive amplification
- Diffuse sensitization - not just pain, but all sensory stimuli (sound, light, smell) are amplified
2. Neuroimaging Evidence
Functional MRI (fMRI) findings:
- In FM patients, mild pressure or heat that normal individuals perceive as touch is processed as pain
- Posterior insula is consistently hyperactive - a key region for sensory integration and emotional processing of pain
- Machine learning paradigms using fMRI data can distinguish FM patients from controls with >90% accuracy
- Increased connectivity between pain-transmission brain regions and non-pain neural networks
- Decreased connectivity between antinociceptive regions
Proton spectroscopy:
- Elevated brain glutamate concentrations in the insula - levels predict pregabalin responsiveness
- Pregabalin therapy normalizes fMRI findings when effective
Neurotransmitter abnormalities:
- Decreased mu-opioid receptor availability in FM (possibly due to increased endogenous opioid release) - explains why opioids are ineffective
- Increased substance P in CSF
- Reduced serotonin and norepinephrine (basis for SNRI treatment)
3. Peripheral Mechanisms
Recent evidence has challenged the purely central model:
- Autoantibodies directed to satellite cells within dorsal root ganglia (DRG) can increase peripheral nociceptor sensitivity
- Binding of antibodies to Fc receptors on peripheral sensory neurons increases sensitivity
- Widespread small fiber neuropathy - demonstrated in skin punch biopsies of FM subgroups
- Ongoing peripheral nociceptive input from comorbid OA, myofascial pain, or obesity can drive or worsen central sensitization
4. Neuroendocrine and Autonomic Dysfunction
- HPA axis dysregulation - low-grade hypothalamic-pituitary-adrenal response
- Autonomic nervous system imbalance - increased sympathetic tone, reduced parasympathetic activity
- Abnormal growth hormone secretion (reduced somatomedin C/IGF-1)
5. Sleep Pathology
- Alpha-delta sleep anomaly - intrusion of alpha (awake) rhythms into Stage 3/4 (delta) NREM sleep
- Subjects experimentally deprived of Stage 4 sleep develop musculoskeletal pain and tenderness resembling FM
Signs and Symptoms
Core Clinical Features
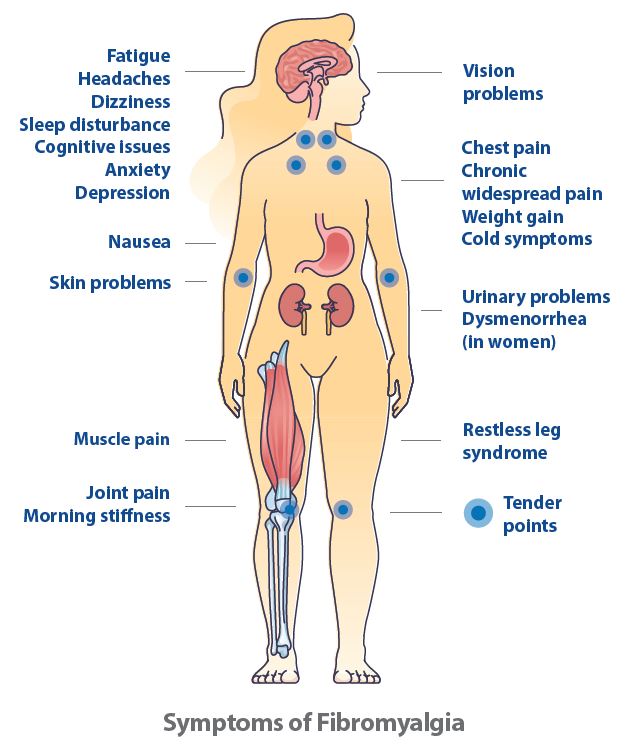
Figure: Fibromyalgia symptoms map showing tender points and widespread systemic manifestations.
Figure: Fibromyalgia symptom overview - musculoskeletal and neuropsychiatric features (Cleveland Clinic)
1. Musculoskeletal Symptoms (Primary - Orthopedic)
| Symptom | Features |
|---|
| Chronic widespread pain | Above and below waist; bilateral; axial skeleton involved; ≥3 months |
| Morning stiffness | Typically 60-90 minutes (vs. RA which is >1 hour but decreases with activity) |
| Tender points | Exquisite tenderness at specific musculotendinous sites with 4 kg pressure |
| Allodynia | Pain from normally non-painful stimuli |
| Hyperalgesia | Exaggerated pain response to normally painful stimuli |
| Muscle spasms | Taut bands, myofascial trigger points |
2. Sleep Disturbance
- Non-restorative sleep (wake up feeling unrefreshed)
- Sleep onset insomnia, frequent awakening
- Alpha-delta sleep anomaly on polysomnography
- Associated with restless legs syndrome
3. Fatigue
- Profound, disproportionate fatigue - the overlap with chronic fatigue syndrome is substantial
- Worsens with minimal activity
- "Fibro fatigue" - distinct from depression-related fatigue
4. Cognitive Dysfunction ("Fibro Fog")
- Difficulty concentrating, memory lapses
- Reduced processing speed
- Cognitive impairment worsens with pain flares and poor sleep
5. Associated Comorbid Conditions
| System | Manifestation |
|---|
| Gastrointestinal | Irritable bowel syndrome, non-ulcer dyspepsia, esophageal dysmotility |
| Genitourinary | Interstitial cystitis, chronic prostatitis, vulvodynia |
| Neurological | Chronic headaches/migraines, temporomandibular disorders, paresthesias |
| Psychiatric | Depression (~30%), anxiety disorders, PTSD |
| Cardiovascular | Non-cardiac chest pain, palpitations |
| Gynaecological | Dysmenorrhea, pelvic pain |
6. Sensory Amplification
- Hyperacusis (sound sensitivity)
- Photophobia (light sensitivity)
- Chemical sensitivity
- Skin hypersensitivity
Tender Points - Historical Diagnostic Criteria
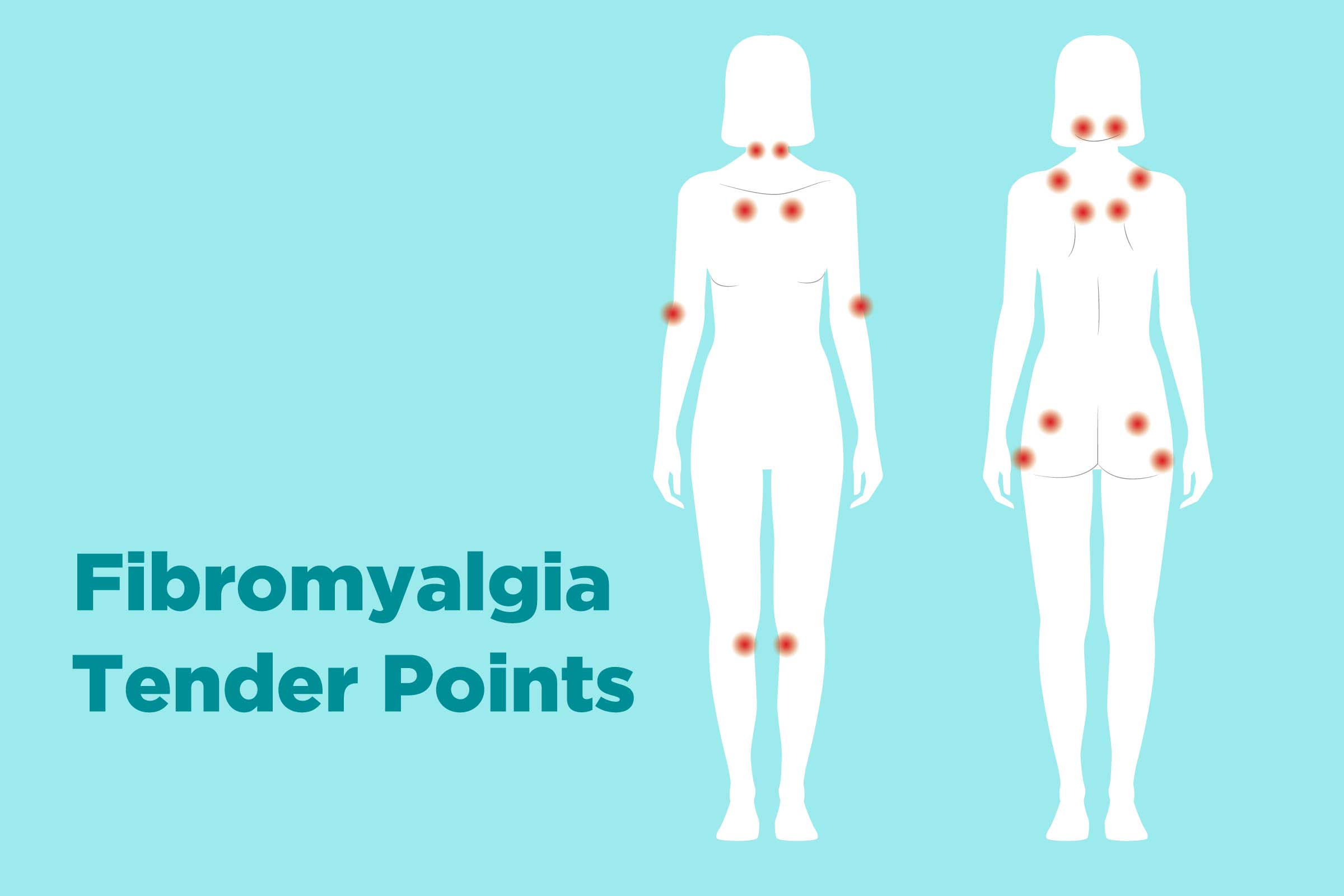
The 1990 ACR criteria required tenderness at ≥11 of 18 designated sites with approximately 4 kg pressure (enough to turn the thumbnail white).
Figure: The 18 ACR 1990 fibromyalgia tender points shown on front and back body views.
The 9 bilateral tender point pairs (18 sites total):
- Occiput - suboccipital muscle insertions
- Low cervical - anterior intertransverse spaces C5-C7
- Trapezius - midpoint of upper border
- Supraspinatus - above medial scapular spine border
- Second rib - second costochondral junctions
- Lateral epicondyle - 2 cm distal to epicondyle
- Gluteal - upper outer quadrant of buttock
- Greater trochanter - posterior to trochanteric prominence
- Knee - medial fat pad proximal to joint line
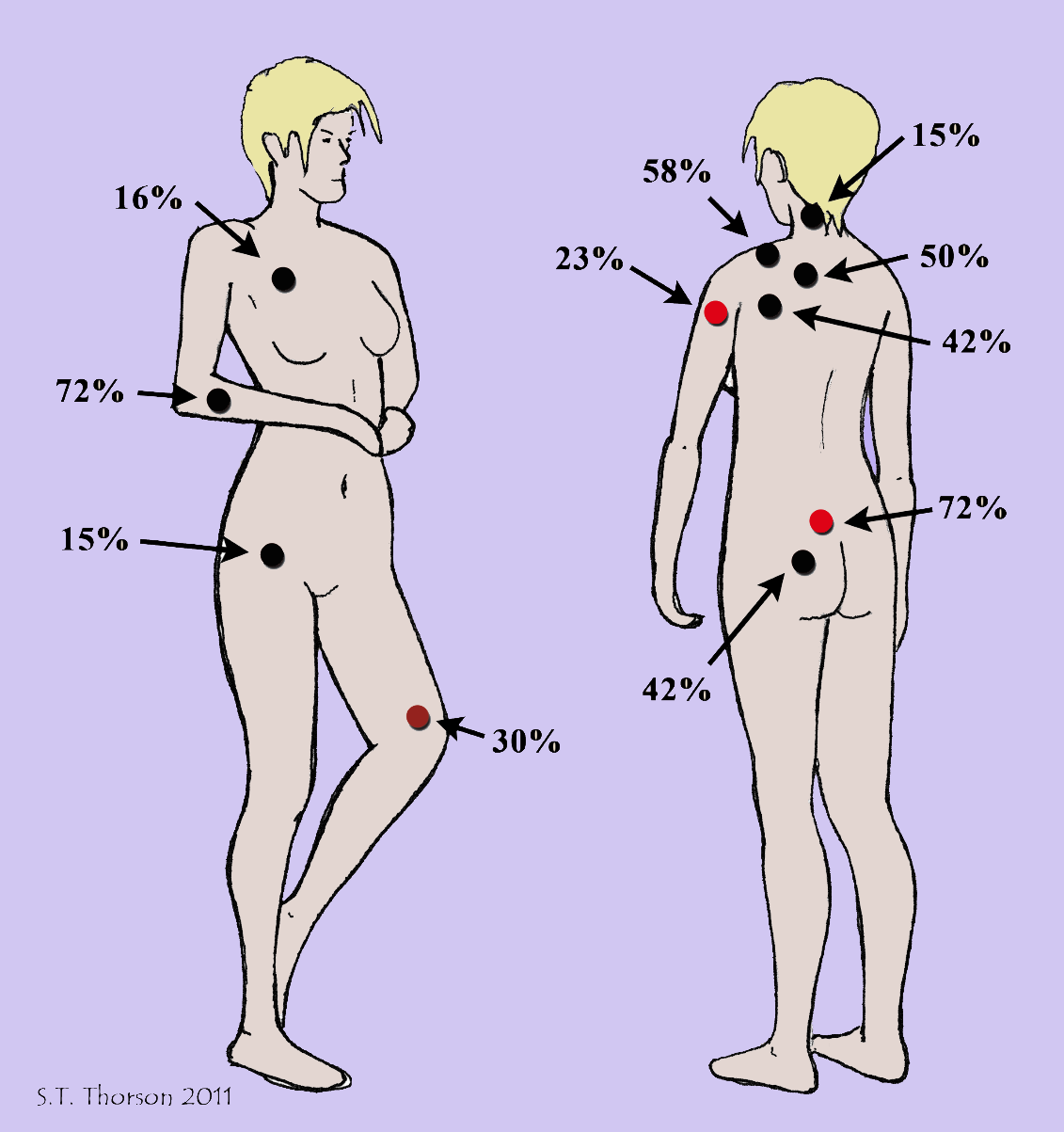
Figure: Fibromyalgia tender point frequency distribution showing percentage of patients affected at each location.
Diagnostic Criteria
ACR 2010/2016 Updated Criteria (Current Standard)
The tender point count has been replaced in modern criteria. Diagnosis now requires ALL of the following:
Figure: Widespread Pain Index (WPI) body regions used in the ACR 2010 diagnostic criteria.
1. Widespread Pain Index (WPI) ≥7 + Symptom Severity Scale (SS) ≥5
OR WPI 4-6 + SS ≥9
2. Pain in at least 4 of 5 body regions (neck, upper back, lower back; left and right shoulder girdle/arm; left and right hip/leg)
3. Symptoms at a similar level for ≥3 months
4. No other disorder that would otherwise fully explain the pain
Symptom Severity Scale (SS) Components
| Domain | Score (0-3) |
|---|
| Fatigue | 0-3 |
| Waking unrefreshed | 0-3 |
| Cognitive symptoms | 0-3 |
| Somatic symptom burden | 0-3 (0=no; 1=few; 2=moderate; 3=many) |
| Total SS | 0-12 |
Investigations
Fibromyalgia is a diagnosis of exclusion - investigations aim to rule out conditions with similar presentations, not to confirm FM.
Routine Laboratory Tests (Harrison's 22E Table 385-2)
| Test | Purpose |
|---|
| ESR or CRP | Rule out inflammatory arthritis, vasculitis |
| CBC | Rule out anemia, infection, hematological disease |
| TSH | Rule out hypothyroidism (causes widespread pain and fatigue) |
| CPK | Rule out inflammatory myopathy (polymyositis) |
| Transaminases | Hepatic disease, medication monitoring |
Guided by History and Examination
| Test | Indication |
|---|
| ANA | If systemic lupus erythematosus suspected |
| Anti-SSA/SSB | Sjögren's syndrome workup |
| RF + anti-CCP | Rheumatoid arthritis |
| Viral serologies | Hepatitis C, HIV, Lyme disease |
| Complete metabolic panel | Electrolyte disturbances, renal disease |
| Spine and joint radiographs | Rule out structural orthopedic pathology |
Key Point:
- All routine labs are typically NORMAL in FM - normal ESR, CRP, and CBC help confirm the FM diagnosis
- Elevated inflammatory markers suggest an alternative or comorbid inflammatory diagnosis
Specialized Investigations (Selected Cases)
| Investigation | Purpose |
|---|
| Polysomnography | Demonstrate alpha-delta sleep anomaly |
| fMRI | Research tool; shows insula hyperactivation |
| Skin punch biopsy | Intraepidermal nerve fiber density - document small fiber neuropathy |
| Quantitative sensory testing | Document hyperalgesia/allodynia objectively |
| Fibromyalgia Impact Questionnaire (FIQ/FIQR) | Measure severity and functional impact |
| Polysymptomatic Distress (PSD) Scale | Quantify fibromyalgianess; monitor treatment |
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|
| Rheumatoid arthritis | Elevated CRP/ESR, positive RF/anti-CCP, synovitis on examination |
| Systemic lupus erythematosus | Positive ANA, multi-organ involvement, rash |
| Hypothyroidism | Elevated TSH; fatigue and myalgia respond to thyroxine |
| Polymyositis/Dermatomyositis | Elevated CPK, proximal muscle weakness, EMG changes |
| Ankylosing spondylitis | Sacroiliitis on MRI, elevated CRP, HLA-B27 positive |
| Myofascial pain syndrome | Regional pain, specific trigger points with referred pain patterns |
| Somatization disorder | No objective musculoskeletal findings; psychiatric comorbidity dominant |
| Chronic fatigue syndrome | Fatigue is primary; less musculoskeletal pain |
| CRPS | Usually unilateral; post-traumatic; trophic changes |
Treatment
Treatment requires a multimodal, multidisciplinary approach. No single therapy is universally effective. The goal is improved function and quality of life, not elimination of pain.
Key principle from Harrison's 22E: Glucocorticoids and NSAIDs are NOT effective for FM-related symptoms. Strong opioids have NO demonstrated efficacy and worsen outcomes.
1. Patient Education and Psychosocial Support
- Explaining the genetics, triggers, and physiology of FM reduces anxiety and healthcare resource use
- Validate the reality of pain (fMRI provides objective evidence)
- Set realistic expectations - focus on function, not pain elimination
- Discourage illness behaviors (frequent physician visits, excessive rest)
2. Non-Pharmacological Treatment (First-Line)
Exercise (Most Effective Single Intervention)
| Type | Notes |
|---|
| Aerobic exercise | Begin low-intensity; advance slowly and consistently; most effective long-term |
| Water-based/hydrotherapy | Ideal for physically inactive or obese patients to start |
| Strength training | After aerobic goals are reached |
| Tai Chi, Yoga, Qigong | Meditative movement therapies - proven benefit |
Physical Therapy
| Intervention | Notes |
|---|
| TENS (Transcutaneous Electrical Nerve Stimulation) | FDA-approved; large RCT showed reduction in movement-evoked pain and fatigue |
| Laser therapy device | FDA-approved |
| Acupuncture | Modest evidence for pain reduction |
| Myofascial release, massage | Symptom relief in some patients |
| Heat therapy | Muscle relaxation; improves stiffness |
Cognitive and Behavioral Therapies
- Cognitive Behavioral Therapy (CBT) - most evidence for psychological comorbidities
- Sleep hygiene interventions - critical given the alpha-delta sleep anomaly
- Biofeedback, hypnosis - pain rehabilitation adjuncts
- Mindfulness-based stress reduction (MBSR) - evidence for quality of life improvement
3. Pharmacological Treatment
FDA-Approved Agents for Fibromyalgia
| Drug | Dose | Mechanism | Notes |
|---|
| Duloxetine (Cymbalta) | 60 mg/day (start 30 mg/day x 1 week) | SNRI - ↑ serotonin + norepinephrine | FDA-approved; especially if depression/anxiety comorbid |
| Milnacipran (Savella) | 50 mg BID (titrate over 7 days) | SNRI | FDA-approved; especially useful for fatigue |
| Pregabalin (Lyrica) | 150-450 mg/day (start 75 mg BID) | α2δ calcium channel ligand; ↓ glutamate | FDA-approved; best for sleep disturbance and pain |
Evidence-Based Non-FDA-Approved Agents
| Drug | Dose | Notes |
|---|
| Amitriptyline | 10-50 mg at bedtime | TCA; excellent for sleep + pain; first-line in many guidelines |
| Cyclobenzaprine | 10-40 mg/day (bedtime or divided) | Muscle relaxant; structurally similar to TCA; good for sleep |
| Gabapentin | Individualized | α2δ ligand; reduces glutamatergic activity |
| Tramadol | 37.5 mg + 325 mg acetaminophen, up to 4x/day | Mild SNRI + weak opioid; use with caution; opioid concerns |
Drug Selection by Symptom Complex
| Dominant Symptom | Preferred Agent |
|---|
| Pain + sleep disturbance | Pregabalin, amitriptyline, cyclobenzaprine |
| Pain + fatigue + anxiety/depression | Duloxetine or milnacipran |
| Pain + anxiety | Pregabalin |
| Pain alone (mild) | Low-dose amitriptyline at bedtime |
AVOID: Strong opioids (no evidence, worsen outcomes), glucocorticoids, NSAIDs (no FM-specific benefit), benzodiazepines long-term.
4. Treatment of Comorbid Conditions
| Comorbidity | Intervention |
|---|
| Inflammatory arthritis (RA, SpA) | Biologics/DMARDs for underlying disease; FM symptoms persist despite inflammation control |
| Osteoarthritis | Arthroplasty may help joint pain but FM predicts worse pain outcomes post-surgery |
| Depression | SNRI (duloxetine), CBT |
| Irritable bowel syndrome | Low-FODMAP diet, antispasmodics |
| Sleep apnea | CPAP therapy (may improve FM symptoms significantly) |
5. Diet and Lifestyle
- Anti-inflammatory, Mediterranean-style diet
- Avoid caffeine, alcohol, processed foods (may worsen sleep and pain)
- Weight management - obesity drives peripheral nociceptive input
- Vitamin D supplementation (often deficient)
Orthopedic Relevance
Fibromyalgia has specific implications for orthopedic practice:
-
Arthroplasty outcomes: Fibromyalgia predicts worse pain outcomes after total knee/hip replacement compared to patients without FM, though significant functional improvement still occurs. Pre-operative FM screening is recommended.
-
Post-traumatic FM: Physical trauma (fractures, surgeries, MVA) can act as a trigger for FM onset in genetically predisposed individuals.
-
Masquerade as orthopedic conditions: Widespread joint and muscle pain mimics polyarthralgia, early RA, OA, and ankylosing spondylitis. FM must be excluded before attributing symptoms to structural disease.
-
Increased sensitivity to post-operative pain: FM patients have amplified pain processing. Peri-operative pain management must anticipate higher analgesia requirements; opioids are particularly problematic.
-
Comorbidity with inflammatory arthritis: 15-25% of spondyloarthropathy patients have comorbid FM; FM score is more predictive of pain/disability than objective inflammation markers in many patients.
-
Soft tissue pain diagnosis: Tendinopathies, bursitis, and myofascial pain syndromes coexist with or mimic FM and must be carefully separated.
Prognosis
- FM rarely resolves completely but follows a waxing-and-waning course
- With education and multimodal therapy, significant functional improvement is achievable
- Predictors of poor outcome: high baseline pain, psychiatric comorbidity, low socioeconomic status, litigation/work disability claims
- FM is associated with significant healthcare utilization and work disability
Treatment Algorithm Summary
Suspected FM: Widespread pain ≥3 months + fatigue + sleep disturbance
|
Exclude organic disease
(CBC, CRP, ESR, TSH, CPK, ANA)
|
Apply 2016 ACR Criteria
(WPI + SS score; ≥4 body regions)
|
FIRST LINE THERAPY
┌────────────────────────────┐
│ Patient Education │
│ Aerobic Exercise │
│ Sleep Hygiene │
│ Low-dose Amitriptyline │
└────────────────────────────┘
|
ADD AS NEEDED (based on symptoms)
┌──────────────┬───────────────┬────────────┐
│Pain+Fatigue │Pain+Sleep │Pain+Anxiety│
│Duloxetine/ │Pregabalin/ │Pregabalin │
│Milnacipran │Cyclobenzaprine│ │
└──────────────┴───────────────┴────────────┘
|
REFRACTORY / SEVERE CASES
CBT + Physiotherapy + Pain Clinic referral
Sources: Goldman-Cecil Medicine 22E (9780323930345); Harrison's Principles of Internal Medicine 22E (9781265977061); Firestein & Kelley's Textbook of Rheumatology (9780323935364); Rheumatology 2-Volume Set 5e (9780702081330);
Jurado-Priego et al., Biomedicines 2024 PMID 39062116;
HAS Clinical Practice Guideline, June 2025;
Iannuccelli et al., Clin Exp Rheumatol 2025 PMID 40470564;
Carrasco-Vega et al., Clin Exp Rheumatol 2024 PMID 38966940.