Prp in Orthopedics how it's prepared what are its indication how it works advantages and disadvantages explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Searching the Web
PRP platelet rich plasma orthopedics preparation indications mechanism advantages disadvantages
Searching PubMed
platelet rich plasma orthopedics
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading Web Page
PRP preparation mechanism growth factors orthopedics indications advantages disadvantages
Searching the Web
PRP classification Dohan Ehrenfest leukocyte rich poor platelet concentration centrifugation steps diagram
Loading Image
Loading Image
I have comprehensive material now. Let me compile the full detailed answer.
Platelet-Rich Plasma (PRP) in Orthopedics
What is PRP?
Platelet-Rich Plasma (PRP) is an autologous blood product - plasma concentrated with platelets at a level typically 4-5 times higher than normal whole blood (normal platelet count: 150,000-400,000/µL; PRP: 1,000,000+/µL). Because it is derived from the patient's own blood, it carries no risk of disease transmission or immune rejection.
PRP has gained significant traction in orthopedics as a biologic, minimally invasive option to harness the body's own regenerative machinery for healing tendons, ligaments, cartilage, and bone.
- Rockwood and Green's Fractures in Adults, 10th ed. 2025: "PRP is an autologous blood product consisting of plasma enriched with a concentration of platelets that is greater than that of whole blood, typically being at least four times the baseline value."
How PRP is Prepared
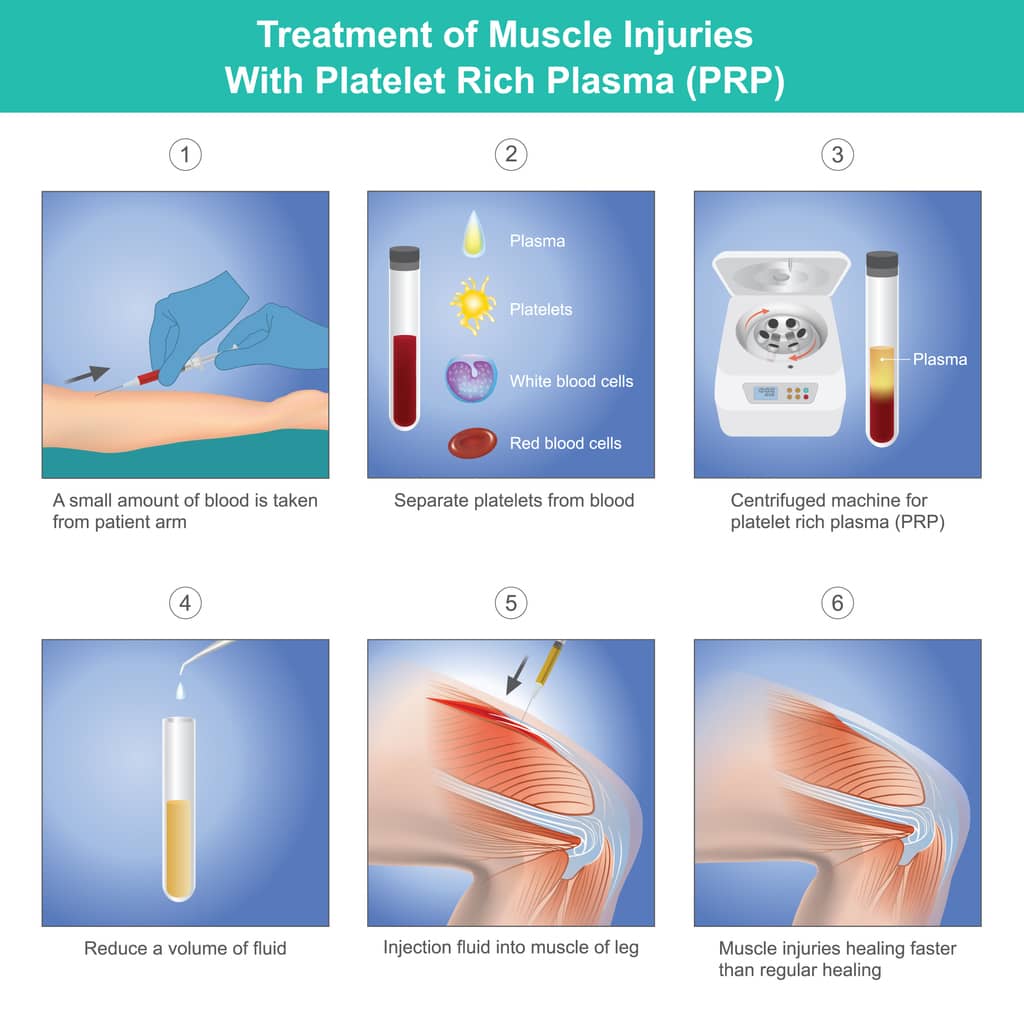
Step 1 - Blood Collection
- 15-60 mL of venous blood is drawn from the patient's antecubital vein into tubes containing an anticoagulant (usually sodium citrate or EDTA) to prevent premature clotting.
Step 2 - Centrifugation (Single or Double Spin)
Two main techniques exist:
Single-spin (Soft Spin):
- Blood is centrifuged once at ~1,500 rpm for ~10 minutes
- This separates RBCs at the bottom from the buffy coat (WBCs + platelets) and plasma above
- The upper two-thirds (plasma + platelets) are aspirated = PRP
- Produces leukocyte-poor (LP-PRP)
Double-spin (Hard Spin):
- First soft spin separates plasma layer
- Plasma supernatant is transferred to a new tube and spun again at ~2,500 rpm for ~15 minutes
- Platelet-Poor Plasma (PPP) at top is discarded; pellet at bottom = concentrated PRP
- Produces leukocyte-rich (LR-PRP) with higher platelet yield
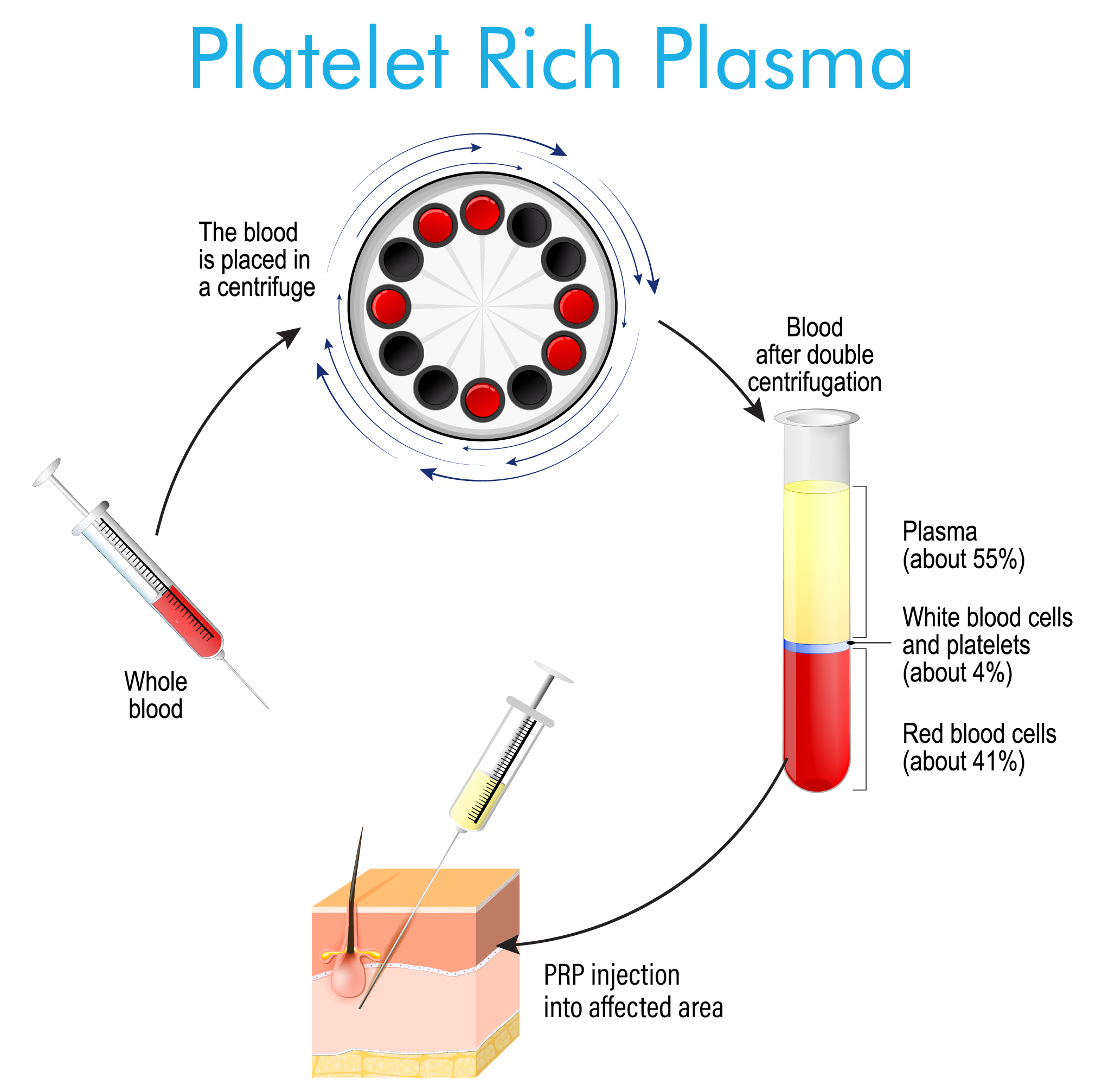
Diagram: Whole blood undergoes double centrifugation. The buffy coat containing platelets and WBCs is separated, then re-spun to concentrate platelets into the PRP fraction.
Step 3 - Activation (Optional)
- Platelets can be activated exogenously using thrombin + calcium chloride (CaCl₂), collagen, or calcium gluconate
- Activation causes platelet degranulation - release of alpha-granule contents (growth factors)
- Some clinicians prefer leaving activation to occur endogenously at the injection site (contact with collagen in tissue) to allow a more physiologic, sustained release
Step 4 - Administration
PRP can be:
- Injected directly into tendons, joints, or peritendinous tissue (often ultrasound-guided)
- Applied as a gel intraoperatively (mixed with thrombin/CaCl₂ to polymerize fibrinogen into fibrin gel)
- Combined with bone graft for spinal fusion or fracture repair
Classification of PRP
There is no single universally accepted classification. Two systems are most widely used:
Dohan Ehrenfest Classification (2009) - Based on cell content and fibrin architecture
| Type | Leukocytes | Fibrin Network | Uses |
|---|---|---|---|
| Pure PRP (P-PRP) | Absent | Low density | Osteoarthritis, intra-articular |
| Leukocyte-Rich PRP (L-PRP) | Present | Low density | Tendinopathy |
| Pure PRF (P-PRF) | Absent | High density | Surgical scaffold |
| Leukocyte & Platelet-Rich Fibrin (L-PRF) | Present | High density | Wound healing, bone |
PAW Classification (DeLong, 2012) - More nuanced for clinical use
- P = Platelet concentration (compared to whole blood baseline)
- A = Activation method (endogenous vs. exogenous)
- W = White blood cell content (above or below baseline)

Growth Factors in PRP - The Active Ingredients
Platelets contain two types of storage granules:
- Alpha (α) granules - contain the major growth factors
- Dense (δ) granules - contain serotonin, ADP, calcium
Key Growth Factors Released
| Growth Factor | Abbreviation | Primary Orthopedic Role |
|---|---|---|
| Platelet-Derived Growth Factor | PDGF (AA, AB, BB) | Cell proliferation, chemotaxis, angiogenesis |
| Transforming Growth Factor-β | TGF-β | Collagen synthesis, cartilage matrix, anti-inflammatory |
| Vascular Endothelial Growth Factor | VEGF | Neovascularization, angiogenesis |
| Fibroblast Growth Factor | FGF | Fibroblast proliferation, tendon repair |
| Insulin-like Growth Factor-1 | IGF-1 | Protein synthesis, chondrocyte survival |
| Connective Tissue Growth Factor | CTGF | Extracellular matrix production |
| Epidermal Growth Factor | EGF | Cell migration, proliferation |
| Hepatocyte Growth Factor | HGF | Anti-fibrotic, tissue regeneration |
| Bone Morphogenetic Proteins | BMPs | Osteogenesis, chondrogenesis |
PRP preparations typically exhibit a 3- to 5-fold increase in growth factor concentrations relative to baseline. Growth factors are sequestered within platelet α-granules and upon activation are released to bind cell-surface receptors. (MDPI, 2025)
Mechanism of Action
PRP works through multiple overlapping mechanisms rather than a single pathway:
1. Direct Cellular Stimulation
- Released PDGF and FGF bind tyrosine kinase receptors on tenocytes, fibroblasts, and chondrocytes
- Activates intracellular signaling cascades (PI3K/Akt, MAPK/ERK) → cell proliferation and migration
- IGF-1 stimulates collagen type I synthesis in tenocytes
2. Immunomodulation
- TGF-β promotes a shift from M1 (pro-inflammatory) to M2 macrophage phenotype
- Reduces IL-1β, IL-6, TNF-α production
- Net effect: controlled resolution of inflammation rather than chronic inflammation
3. Angiogenesis
- VEGF and PDGF-BB stimulate endothelial cell proliferation
- New vessel formation restores blood supply to relatively avascular structures (tendons, meniscus)
4. Anti-catabolic Effects
- TGF-β inhibits matrix metalloproteinases (MMPs) that degrade collagen
- Reduces aggrecanase activity in cartilage → slows OA progression
5. Local Inflammatory Trigger (Newer Understanding)
- Recent evidence (Rockwood & Green, 2025) indicates PRP may work by inducing a controlled local inflammatory response in tendon tissue, which then triggers a subsequent regenerative cascade - similar in concept to prolotherapy
- This explains why leukocyte-rich PRP may actually be preferred for chronic tendinopathy where the degenerative tissue has lost its inflammatory healing capacity
6. Pain Modulation
- Platelet-derived serotonin contributes to analgesic effects
- Reduced pro-inflammatory cytokines lower pain sensitization
Indications in Orthopedics
A. Injection (Primary Treatment)
| Condition | Evidence Level |
|---|---|
| Knee osteoarthritis | Strongest evidence - multiple RCTs and meta-analyses showing benefit over HA and corticosteroids at 6-12 months |
| Lateral epicondylitis (Tennis elbow) | Good evidence - better than corticosteroids at 12 months |
| Plantar fasciitis | Good evidence - effective in chronic cases |
| Achilles tendinopathy | Moderate evidence |
| Patellar tendinopathy | Moderate evidence |
| Rotator cuff tendinopathy | Moderate evidence |
| Hamstring injuries | Emerging evidence |
| Osteochondral lesions (talus) | Beneficial for functional outcomes at 7-42 months |
2025 meta-analysis (PMID: 39751394): PRP injections for knee OA show clinically significant improvement in pain and function, with effect influenced by platelet concentration.
B. Surgical Adjunct
| Procedure | Role of PRP |
|---|---|
| ACL reconstruction | Applied to graft to enhance ligamentization |
| Rotator cuff repair | Reduces re-tear rate; enhances tendon-to-bone healing |
| Total knee arthroplasty | Reduces post-op pain and blood loss |
| Spinal fusion | Combined with bone graft to enhance osteogenesis |
| Long-bone nonunion | Stimulates callus formation |
| Hip fracture repair | Adjunctive healing support |
| Osteochondral grafting | Promotes integration and chondrocyte survival |
Contraindications
- Active infection at injection site
- Systemic infection or sepsis
- Thrombocytopenia (<100,000 platelets/µL)
- Platelet dysfunction disorders
- Active malignancy (concern for stimulating tumor growth)
- Anticoagulant therapy (relative)
- Hypersensitivity to thrombin/bovine products (if used for activation)
Advantages of PRP
| Advantage | Detail |
|---|---|
| Autologous | Derived from patient's own blood - zero risk of disease transmission, allergic reaction, or immune rejection |
| Minimally invasive | Outpatient procedure, no surgery required for injection use |
| Biologically active | Targets multiple healing pathways simultaneously with physiologic mediators |
| Safety profile | Excellent safety record; adverse events largely limited to transient post-injection pain flare |
| Synergistic | Can be combined with surgery, hyaluronic acid, or bone graft materials |
| No systemic side effects | Unlike corticosteroids (which cause cartilage degradation, metabolic effects) or NSAIDs (GI/renal toxicity) |
| Tissue regeneration | Unlike corticosteroids (anti-inflammatory only), PRP aims to repair underlying tissue |
| Point-of-care preparation | Can be prepared chairside in 15-20 minutes |
| Repeatable | Can be administered in series (typically 1-3 injections) |
Disadvantages of PRP
| Disadvantage | Detail |
|---|---|
| Lack of standardization | No universal preparation protocol; platelet concentration, leukocyte content, activation, and volume vary widely between products and centers |
| Variable evidence | While some indications show strong evidence (knee OA), others remain investigational; several placebo-controlled trials showed no benefit |
| Cost | Typically not covered by insurance (considered investigational by many payers); patient pays out-of-pocket ($500-$2,000 per injection) |
| Transient pain flare | 24-72 hours of increased pain after injection due to inflammatory response from activation |
| Inconsistent dosing | No consensus on optimal platelet concentration, injection volume, frequency, or interval |
| Limited large RCTs | Most studies are small, heterogeneous, and lack standardized PRP characterization |
| Risk of infection | Small risk when aseptic technique not strictly followed |
| Paradoxical inhibition | Supra-physiologic platelet concentrations may actually inhibit rather than promote regeneration (high-dose paradox) |
| Leukocyte debate | Leukocyte-rich PRP may worsen outcomes in intra-articular applications (synovial inflammation) while being beneficial in tendinopathy |
| No structural guarantee | Symptomatic improvement does not always correlate with structural healing on imaging |
Rheumatology 2022, Elsevier: "Two recent placebo-controlled trials failed to show efficacy [of PRP], one in knee OA, another in ankle OA" - highlighting that the evidence is not uniformly positive.
Comparison: PRP vs. Corticosteroids
| Feature | PRP | Corticosteroids |
|---|---|---|
| Mechanism | Regenerative | Anti-inflammatory only |
| Onset | 4-8 weeks | Days |
| Duration | Months to years | Weeks to months |
| Long-term tissue effect | Potentially restorative | Cartilage/tendon degradation with repeated use |
| Cost | High | Low |
| Insurance coverage | Usually not covered | Covered |
| Evidence base | Growing | Established |
Current Evidence Snapshot (2025)
- [Systematic Review, 2025 PMID: 39751394] - Meta-analysis of RCTs for knee OA confirms clinically significant improvement in pain/function with PRP; effect size influenced by platelet concentration
- [Systematic Review PMID: 38310528] - Tennis elbow: PRP superior to corticosteroids at 12 months
- Rockwood & Green (2025): "A recent meta-analysis of smaller studies identified that PRP did improve the treatment of tendinopathy after 6 months of follow-up"
- The field is rapidly evolving; lack of standardization remains the primary barrier to definitive guidelines
Summary
PRP is a promising, biologically rational orthopedic therapy that harnesses concentrated autologous growth factors to promote tissue healing. Its strongest indication is knee osteoarthritis and chronic tendinopathy (lateral epicondylitis, plantar fasciitis). As a surgical adjunct, it shows benefit in rotator cuff repair and ACL reconstruction.
The critical challenges are standardization of preparation, clarity on which PRP type (leukocyte-rich vs. poor) to use for which condition, and the need for large, well-designed RCTs with standardized PRP products before insurance coverage and universal guidelines can be established.
Sources: Rockwood and Green's Fractures in Adults 10th ed. 2025 | Rheumatology 2-Volume Set (Elsevier 2022) | MDPI IJMS 2025 | PubMed PMID: 39751394 | Arthroscopy Journal 2021
This is a shared conversation. Sign in to Orris to start your own chat.