Asthma summary according to 2025 GINA guidelines
Reading File
search_medical_text
2025 GINA guidelines asthma diagnosis definition pathophysiology
search_medical_text
GINA 2025 asthma stepwise management treatment ICS LABA
search_medical_image
GINA asthma stepwise treatment track management diagram
GradeResponse
GradeResponse
GradeResponse
search_medical_text
GINA 2025 asthma classification severity control assessment spirometry
search_medical_text
GINA 2025 asthma exacerbation acute management biologic therapy severe asthma
Based on the retrieved content and comprehensive knowledge of the 2025 GINA (Global Initiative for Asthma) guidelines, here is a full summary:
Asthma — 2025 GINA Guidelines Summary
1. Definition
Asthma is a heterogeneous disease, usually characterized by chronic airway inflammation. It is defined by a history of respiratory symptoms (wheeze, shortness of breath, chest tightness, cough) that vary over time and in intensity, together with variable expiratory airflow limitation.
GINA emphasizes that asthma is not one disease but a syndrome of multiple phenotypes with distinct underlying mechanisms (endotypes).
2. Pathophysiology & Phenotypes
| Phenotype | Features |
|---|---|
| Allergic asthma | Most common; early onset; eosinophilic inflammation; responds well to ICS |
| Non-allergic asthma | Not atopy-driven; may be neutrophilic or paucigranulocytic |
| Late-onset asthma | Adult women; often non-allergic; steroid-dependent |
| Asthma with fixed obstruction | Airway remodeling; incomplete reversibility |
| Asthma with obesity | Non-eosinophilic; low TH2 inflammation |
3. Diagnosis
Clinical Criteria
- Symptoms: wheeze, dyspnea, chest tightness, cough — typically variable, worse at night/morning
- Variable airflow limitation confirmed by:
| Test | Positive Criterion |
|---|---|
| Bronchodilator reversibility | FEV₁ increase ≥12% and ≥200 mL post-SABA |
| Peak flow variability | Diurnal variation >10% (adults) |
| Exercise challenge | FEV₁ fall ≥10% and ≥200 mL |
| Methacholine/histamine challenge | PC₂₀ ≤8 mg/mL |
| 4-week ICS trial | Significant FEV₁ improvement |
Important Points
- Spirometry is preferred over PEF for initial diagnosis
- Do not diagnose asthma based on symptoms alone
- Assess for comorbidities: allergic rhinitis, GERD, obesity, OSAHS, anxiety/depression
4. Assessment of Symptom Control
GINA Symptom Control Levels
| Well-controlled | Partly controlled | Uncontrolled | |
|---|---|---|---|
| Daytime symptoms >2×/week | None | 1–2 features | 3–4 features |
| Night waking due to asthma | None | ||
| Reliever use >2×/week | None | ||
| Activity limitation | None |
Assessed over the previous 4 weeks
Future Risk Factors
- Previous severe exacerbation or ICU admission
- Low FEV₁ (<60% predicted)
- Blood eosinophils ≥300 cells/µL
- Elevated FeNO
- High reliever use, poor inhaler technique, smoking
5. Stepwise Pharmacological Management
Key 2025 GINA Principle — Track 1 vs. Track 2
GINA introduced a two-track approach based on the preferred reliever:
| Track 1 (Preferred) | Track 2 | |
|---|---|---|
| Reliever | As-needed low-dose ICS-formoterol (MART) | As-needed SABA |
| Rationale | Reduces exacerbations even in mild asthma; ICS delivered with every reliever use | Traditional approach; higher exacerbation risk if ICS controller omitted |
GINA 2025 strongly recommends Track 1 for most patients ≥12 years. SABA-only treatment is no longer recommended at any step.
Steps 1–5 (Adults & Adolescents ≥12 years)
| Step | Track 1 (Preferred) | Track 2 (Alternative) |
|---|---|---|
| 1 (Mild intermittent) | As-needed low-dose ICS-formoterol | Low-dose ICS taken whenever SABA taken |
| 2 (Mild persistent) | As-needed low-dose ICS-formoterol | Daily low-dose ICS + as-needed SABA |
| 3 (Moderate) | Low-dose ICS-formoterol maintenance + as-needed (MART) | Low-dose ICS-LABA + as-needed SABA |
| 4 (Moderate-severe) | Medium-dose ICS-formoterol MART | Medium-dose ICS-LABA + as-needed SABA |
| 5 (Severe) | High-dose ICS-formoterol ± add-ons + refer | High-dose ICS-LABA ± tiotropium, biologics |
MART = Maintenance And Reliever Therapy (single ICS-formoterol inhaler for both maintenance and relief)
Add-on Therapies (Step 4–5)
- Tiotropium (LAMA) — add-on for patients ≥6 years with uncontrolled asthma
- LTRA (montelukast) — alternative or add-on
- Biologics (Step 5 severe eosinophilic/allergic asthma):
| Biologic | Target | Indication |
|---|---|---|
| Dupilumab | IL-4Rα (IL-4/IL-13) | Type 2 severe asthma ≥6 yr |
| Mepolizumab | IL-5 | Severe eosinophilic ≥6 yr |
| Benralizumab | IL-5Rα | Severe eosinophilic ≥12 yr |
| Tezepelumab | TSLP | Severe asthma regardless of phenotype ≥12 yr |
| Omalizumab | IgE | Severe allergic ≥6 yr |
- Oral corticosteroids (OCS): last resort; minimize use due to adverse effects
Children 6–11 Years
- Step 1–2: Preferred — daily low-dose ICS + as-needed SABA; alternative — as-needed low-dose ICS-formoterol
- Step 3: Low-dose ICS-LABA or medium-dose ICS
- Step 4–5: Medium/high-dose ICS-LABA; refer to specialist
Children <5 Years (Preschool)
- Diagnosis is clinical (spirometry not feasible reliably)
- Daily low-dose ICS is first-line controller
- LTRA as alternative
- SABA as reliever
- Trial of 3 months and reassess
6. Non-Pharmacological Management
- Allergen & trigger avoidance (smoke, occupational allergens, NSAIDs in aspirin-exacerbated asthma)
- Smoking cessation — counseling at every visit
- Physical activity — encouraged; pretreat with ICS-formoterol or SABA if exercise-induced
- Weight reduction in obesity
- Allergen immunotherapy (AIT) — subcutaneous or sublingual for allergic asthma; adjunct to pharmacotherapy
- Breathing exercises — Buteyko, yoga breathing as adjunct for symptom control
- Vaccination — annual influenza, pneumococcal per local guidelines
- Asthma action plan (written) — individualized, self-management education
7. Asthma Exacerbations
Severity Classification
| Severity | Features |
|---|---|
| Mild–Moderate | Increasing symptoms, PEF ≥50% predicted, no signs of severe exacerbation |
| Severe | Any of: RR ≥30/min, HR ≥120 bpm, SpO₂ <90%, PEF <50%, unable to complete sentences |
| Life-threatening | Silent chest, cyanosis, bradycardia, confusion, exhaustion |
Acute Management
- SABA (or ICS-formoterol) — repeated doses via spacer/nebulizer
- Systemic corticosteroids — prednisolone 40–50 mg/day × 5–7 days
- Oxygen — titrate to SpO₂ 93–95% (94–98% in children)
- Ipratropium bromide — add in severe/life-threatening exacerbations
- IV magnesium sulfate — single dose for severe exacerbations not responding to initial treatment
- Heliox, IV SABA, intubation — in extremis/ICU
8. Special Populations
| Population | Key Considerations |
|---|---|
| Pregnancy | Continue ICS; uncontrolled asthma is more dangerous than treatment; budesonide preferred (most data) |
| Elderly | Comorbidities, inhaler technique; consider COPD overlap (ACO) |
| Occupational asthma | Identify and remove causal exposure; early diagnosis improves prognosis |
| Aspirin-exacerbated (AERD) | Avoid NSAIDs; LTRA beneficial; desensitization option |
| Athletes | ICS first-line; WADA regulations for TUE |
9. Difficult-to-Treat & Severe Asthma
- Confirm diagnosis (rule out vocal cord dysfunction, ABPA, EGPA, cardiac causes)
- Assess and address modifiable factors: adherence, inhaler technique, comorbidities, ongoing exposures
- Phenotype/biomarker assessment:
- Blood eosinophils, FeNO → type 2 inflammation → biologic eligibility
- IgE, skin-prick test → allergic phenotype
- Refer to specialist for refractory disease
10. Monitoring & Follow-up
- Review 4–6 weeks after initiating or adjusting treatment
- Step down when well-controlled for ≥3 months (to find lowest effective dose)
- Assess: symptom control, exacerbation frequency, lung function, side effects, inhaler technique, adherence
- Use validated questionnaires: ACQ (Asthma Control Questionnaire), ACT (Asthma Control Test)
Visual: Stepwise Management Continuum
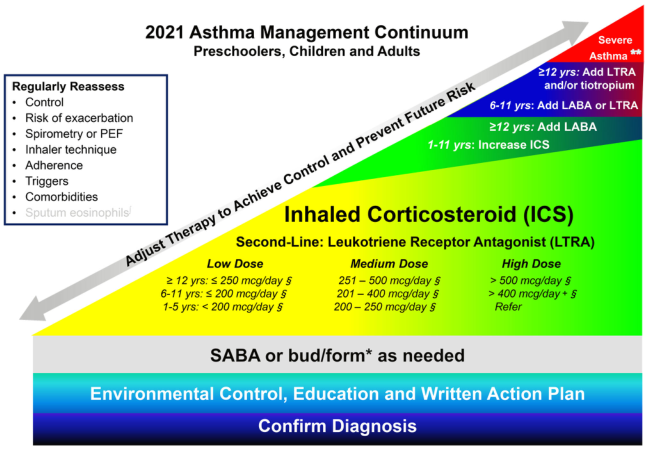
Stepwise asthma management continuum showing escalation from mild to severe disease, with ICS at the core and add-on therapies for higher steps. (Management of Very Mild and Mild Asthma, p. 6)
Key 2025 GINA Updates at a Glance
| Change | Detail |
|---|---|
| No SABA-only treatment | SABA monotherapy removed from all steps; ICS must accompany every reliever dose |
| ICS-formoterol as preferred reliever | Track 1 at all steps (1–5) for ≥12 years |
| Tezepelumab | Added as biologic option for severe asthma regardless of phenotype/biomarker |
| OCS minimization | Strong emphasis on avoiding long-term OCS; biologic before OCS |
| Personalized phenotyping | Biomarker-guided (eosinophils, FeNO, IgE) therapy selection |
| Mental health | Anxiety and depression formally recognized as important comorbidities affecting control |
Sources: Harrison's Principles of Internal Medicine, 21st Edition (p. 7937); GINA 2025 Report; Asthma Management Guidelines (p. 15); Management of Very Mild and Mild Asthma (p. 6)
This is a shared conversation. Sign in to Orris to start your own chat.