Variant types of thyroid malignancy, pathology, management, staging follow up
Reading File
Finding Sources
Finding Sources
Searching PubMed
"thyroid cancer" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the complete response.
Thyroid Malignancy: Variants, Pathology, Management, Staging & Follow-up
Overview
Thyroid carcinoma is the most common malignancy of the endocrine system. Malignant tumors are classified by cell of origin:
| Type | % of cases | Cell of origin |
|---|---|---|
| Papillary Thyroid Carcinoma (PTC) | ~84% | Follicular epithelium |
| Follicular Thyroid Carcinoma (FTC) | ~11% | Follicular epithelium |
| Oncocytic (Hürthle cell) Carcinoma (OCA) | ~3–4% | Follicular epithelium |
| Poorly Differentiated TC (PDTC) | ~1–2% | Follicular epithelium |
| Medullary Thyroid Carcinoma (MTC) | ~2–5% | Parafollicular C cells |
| Anaplastic Thyroid Carcinoma (ATC) | ~1% | Follicular epithelium (dedifferentiated) |
| Primary Thyroid Lymphoma | Rare | Lymphoid tissue |
(Sabiston Textbook of Surgery, p. 1509; Harrison's Principles of Internal Medicine 22E, p. 3088)
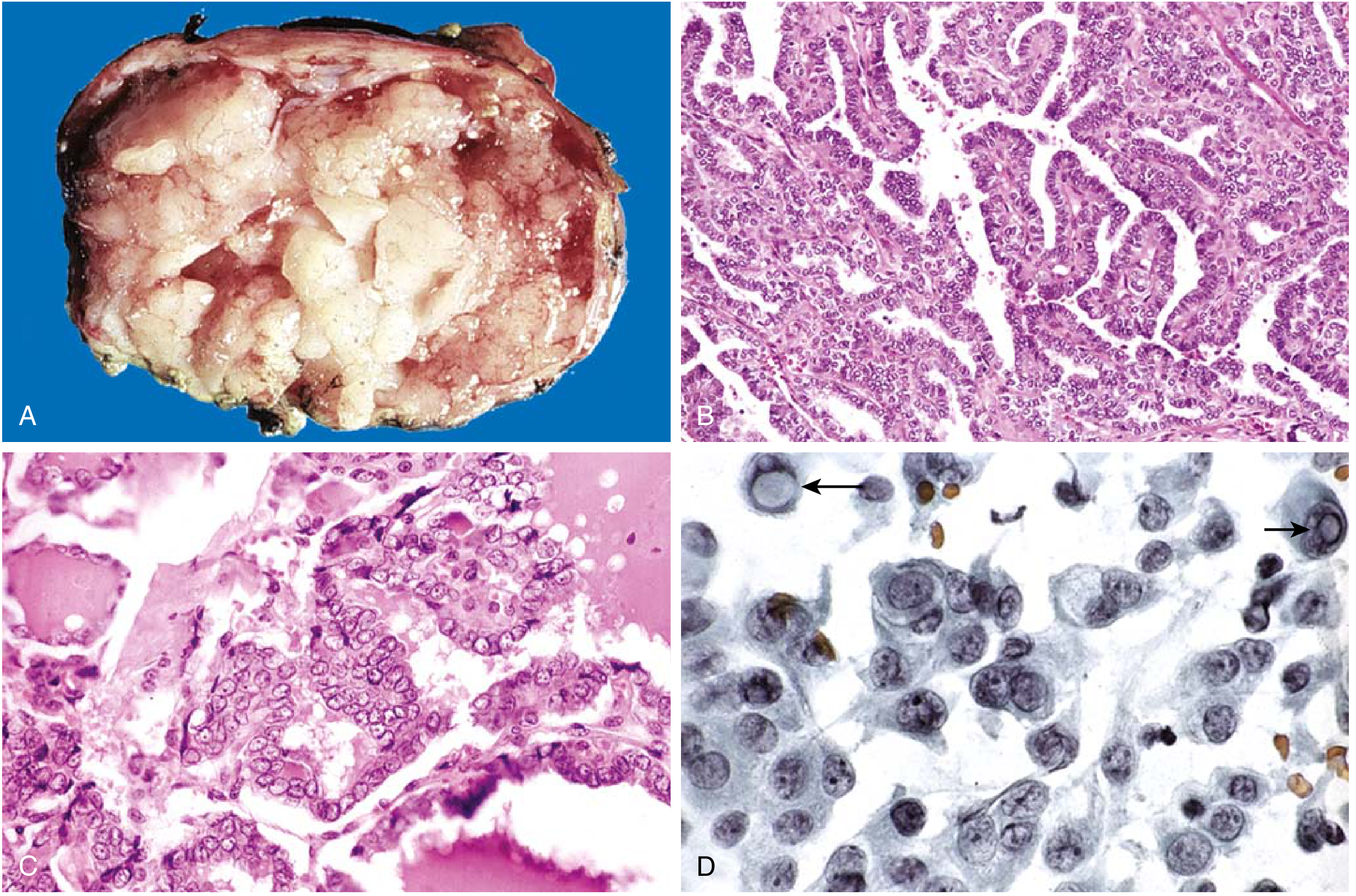
1. Papillary Thyroid Carcinoma (PTC)
Pathology
PTC accounts for the vast majority of radiation-associated thyroid cancers. Tumors may be solitary or multifocal, well-circumscribed or infiltrative.
Histologic hallmarks (Robbins Pathology, p. 737):
- Branching papillae with fibrovascular stalks covered by cuboidal epithelium
- Ground-glass (Orphan Annie) nuclei - optically clear appearance due to finely dispersed chromatin
- Intranuclear pseudoinclusions and nuclear grooves (cytoplasmic invaginations)
- Psammoma bodies - concentric calcifications in papillary cores; almost never in follicular or medullary carcinomas
- Lymphatic invasion common; blood vessel invasion uncommon in smaller lesions
- Cervical lymph node metastases in up to 50% of cases
Molecular alterations:
- BRAF V600E - most common point mutation (~45% of PTC), activates MAPK pathway, associated with aggressive features and RAI resistance
- RAS mutations - 20-30%, more common in follicular variant PTC; activates both MAPK and PI3K-AKT
- RET/PTC rearrangements - 5-10%, characteristic of radiation-induced PTC; multifocal, more extrathyroidal extension
- TERT promoter mutations - up to 27%, especially co-occurring with BRAF; associated with RAI resistance and high recurrence risk
- PAX8-PPARG - seen in follicular variant PTC
Variants of PTC (>12 described):
- Classical/conventional
- Follicular variant (encapsulated vs infiltrative) - most common variant; almost totally follicular architecture but PTC nuclear features
- Tall cell variant - aggressive, occurs in older patients
- Columnar cell variant - aggressive
- Diffuse sclerosing variant
- Solid/trabecular variant
- Hobnail variant - high recurrence risk
- Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) - reclassified as non-malignant
Spread: Primarily lymphatic to cervical nodes (central level VI, then lateral II-IV). Hematogenous spread to lung and bone in 3-5% of cases. Micrometastases (<2 mm in lymph nodes) do not affect prognosis; gross metastases to multiple 2-3 cm nodes indicate ~25-30% recurrence risk.
2. Follicular Thyroid Carcinoma (FTC)
Pathology
More common in women (3:1), peak incidence 40-60 years. More prevalent in iodine-deficient regions; incidence is declining in iodine-sufficient areas.
Gross: Single nodule, well-circumscribed or widely infiltrative; may be indistinguishable from follicular adenoma on gross examination.
Microscopy (Robbins Pathology, p. 738): Uniform cells forming small follicles resembling normal thyroid. The distinction from follicular adenoma requires extensive histologic sampling of the tumor-capsule interface for capsular and/or vascular invasion - this cannot be determined by FNA alone.
Classification by invasion:
- Minimally invasive - capsular invasion only; very low metastatic risk; <10% die within 10 years
- Widely invasive/angioinvasive - blood vessel invasion; metastases to lung, bone, liver; up to 50% die within 10 years
Molecular alterations: PI3K/AKT pathway mutations, PTEN loss-of-function (associated with Cowden syndrome), RAS mutations, PAX8-PPARG fusion.
Spread: Hematogenous (lungs, bone, liver, CNS). Regional lymph node metastases are uncommon - in contrast to PTC.
3. Oncocytic (Hürthle Cell) Carcinoma (OCA)
Previously classified as a variant of FTC but now a distinct entity in AJCC 8th edition. Composed of oncocytes (cells with mitochondria-rich eosinophilic cytoplasm). More likely to be RAI-resistant than classic FTC. Diagnosed by capsular/vascular invasion same as FTC. Managed similarly to FTC/PTC.
4. Medullary Thyroid Carcinoma (MTC)
Pathology
Arises from parafollicular C cells (neuroendocrine cells), not follicular epithelium. Accounts for ~2-5% of thyroid cancers. Does not take up radioiodine.
Histology (Sabiston, p. 1516): Plasmacytoid morphology with eccentric round nuclei, "salt-and-pepper" chromatin, small nucleoli, and amyloid infiltrate (from polymerized calcitonin). Calcitonin immunostaining is positive.
Tumor marker: Serum calcitonin (marker of residual/recurrent disease). Serum CEA is also elevated and has prognostic significance.
Molecular alterations:
- RET proto-oncogene (chromosome 10q11.2) - germline mutations in virtually all hereditary MTC; somatic (acquired) RET mutations in ~50% of sporadic MTC
- Codon C634 mutations are most common in hereditary MTC
Forms:
- Sporadic (~75%) - unifocal; usually presents 4th-6th decade; up to 50% have palpable neck mass; cervical nodal metastases in >70% with palpable tumor; distant mets (liver, mediastinum, lungs, bone) in 10-15%
- Familial (~25%):
- MEN 2A (Sipple syndrome) - MTC + pheochromocytoma + primary hyperparathyroidism; codon 634 RET mutation; presents 3rd decade
- MEN 2B - MTC + pheochromocytoma + marfanoid habitus + mucosal neuromas + intestinal ganglioneuromatosis; codon M918T mutation; most aggressive; presents before 2nd decade
- Familial MTC - MTC without other MEN features
ATA Risk Classification for Hereditary MTC (2015 guidelines):
- Highest risk (MEN 2B, M918T mutation) - prophylactic thyroidectomy within first 6 months of life
- High risk (C634F/G/R/S/W/Y, C609, C611, etc.) - thyroidectomy before age 5 years
- Moderate risk - thyroidectomy timing guided by calcitonin levels/imaging
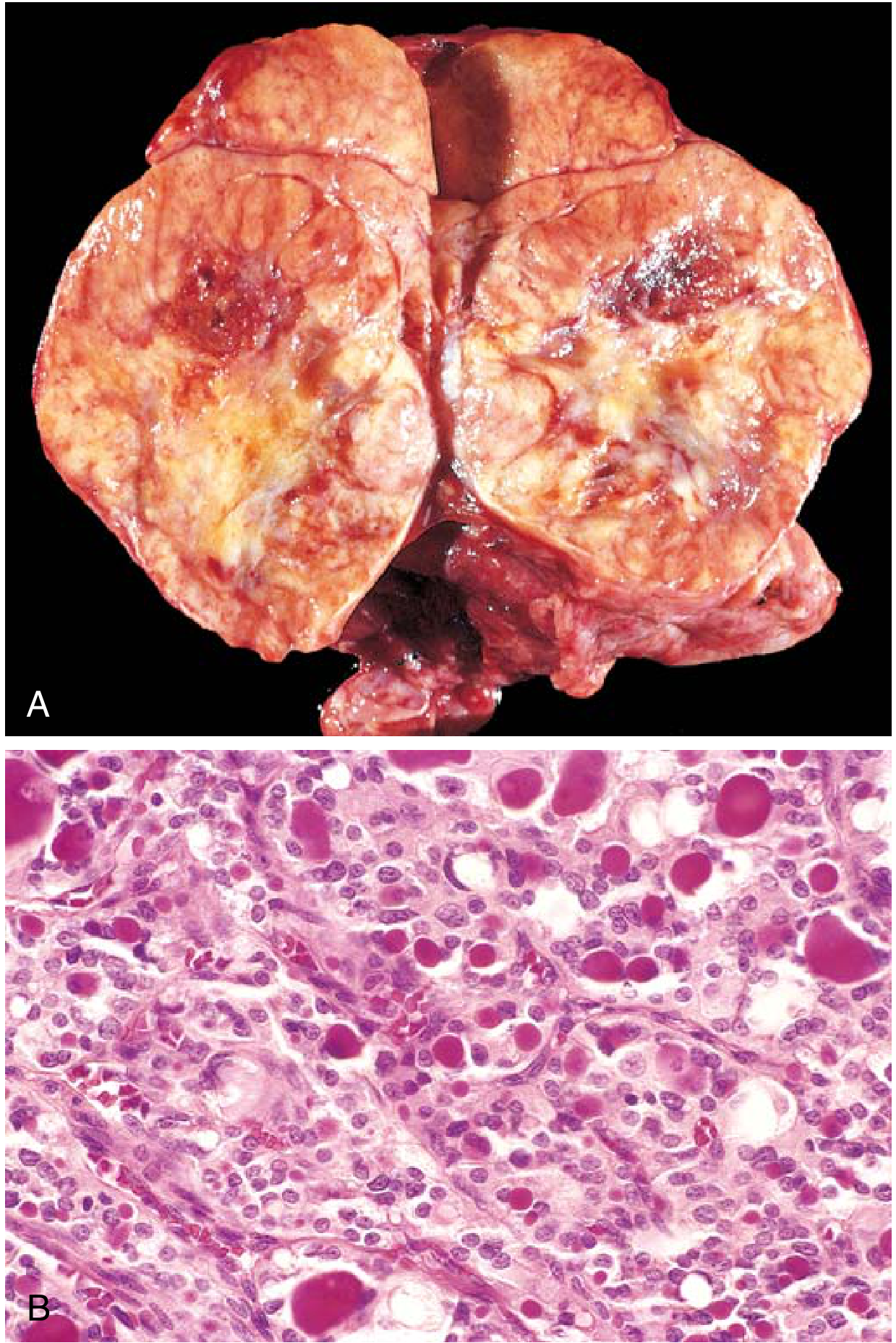
5. Anaplastic Thyroid Carcinoma (ATC)
Pathology
Undifferentiated tumors of follicular epithelium. Near-100% mortality; median survival ~3-6 months from diagnosis. Mean age at presentation: 65 years. Approximately 25% arise from pre-existing well-differentiated carcinoma (PTC or FTC); another 25% harbor a concurrent differentiated tumor.
Histology: Three morphologic patterns - spindle cell, giant cell (most common), and squamoid. Extreme nuclear pleomorphism, brisk mitotic activity, tumor necrosis.
Molecular alterations: Loss-of-function TP53 mutations (most specific to ATC), plus mutations shared with differentiated carcinoma (RAS, PIK3CA, BRAF V600E). BRAF V600E present in ~40-45% of ATC cases, which has therapeutic implications.
6. TNM Staging (AJCC 8th Edition)
Primary Tumor (T)
| Stage | Description |
|---|---|
| T1a | ≤1 cm, limited to thyroid |
| T1b | >1 cm, ≤2 cm, limited to thyroid |
| T2 | >2 cm, ≤4 cm, limited to thyroid |
| T3a | >4 cm, limited to thyroid |
| T3b | Gross extrathyroidal extension into strap muscles only (any size) |
| T4a | Gross ETE into subcutaneous tissue, larynx, trachea, esophagus, or recurrent laryngeal nerve |
| T4b | Gross ETE into prevertebral fascia, or encasing carotid artery or mediastinal vessels |
Regional Lymph Nodes (N)
| Stage | Description |
|---|---|
| N1a | Metastasis to level VI or VII (pretracheal, paratracheal, prelaryngeal/Delphian, upper mediastinal) |
| N1b | Metastasis to lateral neck (levels I-V) or retropharyngeal nodes |
Stage Grouping - Differentiated TC (PTC/FTC/OCA/PDTC)
Age <55 years:
| Stage | TNM |
|---|---|
| I | Any T, Any N, M0 |
| II | Any T, Any N, M1 |
Age ≥55 years:
| Stage | TNM |
|---|---|
| I | T1-T2, N0, M0 |
| II | T1-T2 N1 M0, or T3a/T3b any N M0 |
| III | T4a, any N, M0 |
| IVA | T4b, any N, M0 |
| IVB | Any T, any N, M1 |
Key point: The 8th edition significantly shifted the age cutoff from 45 to 55 years, which downstaged many patients. Expected 10-year disease-specific survival for Stage I = 98-100%.
Anaplastic TC: All cases are classified as Stage IVA (disease confined to thyroid), IVB (gross ETE), or IVC (distant metastases) - regardless of age.
(Cummings Otolaryngology, p. 2372; Harrison's Principles, p. 3090)
Additional Risk-Stratification Systems
- MACIS (Mayo Clinic): Score based on Metastasis + Age + Completeness of resection + Invasion + Size. Score <6.0 = 99% 20-year survival
- AMES: Age, Metastases, Extent of tumor, Size - divides into low-risk and high-risk groups
- ATA Dynamic Risk Stratification - assigns response-to-therapy categories after treatment:
- Excellent response - no clinical, biochemical, or structural evidence of disease (1-4% recurrence risk)
- Biochemical incomplete response - abnormal Tg or rising anti-Tg antibodies, no structural disease (50% achieve NED spontaneously or with Rx)
- Structural incomplete response - persistent locoregional or distant disease (mortality up to 50% with distant mets)
- Indeterminate response - nonspecific findings (15-20% develop structural disease)
7. Management
Differentiated Thyroid Cancer (PTC, FTC, OCA)
Surgery - Primary Treatment:
-
Thyroid lobectomy - acceptable for low-risk, unilateral DTC 1-4 cm, no ETE, no metastatic disease; recommended for <1 cm DTC (after active surveillance discussion)
-
Total thyroidectomy - preferred for (Sabiston, p. 1515):
- Tumor ≥4 cm
- Clinically evident nodal metastases
- Gross extrathyroidal extension
- Evidence of distant metastatic disease
- Radiation-induced DTC
- Familial non-medullary TC
- Multifocal bilateral DTC
-
Active surveillance - an option for small (<1.5 cm) intrathyroidal micropapillary cancers without cervical LN mets, ETE, or proximity to the recurrent laryngeal nerve
Lymph Node Dissection:
- Therapeutic compartment-based dissection for clinically/radiographically evident nodal disease
- Central compartment (level VI ± VII) dissection for ipsilateral central nodal involvement
- Lateral neck dissection (levels II-V) for proven lateral neck metastases
- Prophylactic central neck dissection remains controversial
Radioiodine (RAI / ¹³¹I):
- Not indicated for T1 tumors ≤2 cm confined to thyroid (no recurrence/survival benefit)
- No benefit demonstrated for larger (>2 cm but <4 cm) low-risk tumors
- Indicated for higher risk patients: larger tumors, aggressive variants, vascular invasion, ETE, large-volume lymph node metastases, older patients
- Low-dose ¹³¹I (1100 MBq / 30 mCi) for remnant ablation; high-dose (up to 5500 MBq / 150 mCi) for adjuvant treatment of residual/metastatic disease
- Requires TSH stimulation (TSH >25 mIU/L) - achieved by either thyroid hormone withdrawal or recombinant human TSH (rhTSH, thyrotropin alfa)
- Preceded by low-iodine diet for 1-2 weeks
TSH Suppression:
- Levothyroxine to suppress TSH - rationale: differentiated TCs express TSH-R and remain responsive to TSH stimulation
- Degree of suppression tailored to risk: high-risk patients aim for TSH <0.1 mIU/L; low-risk patients can maintain low-normal TSH
Targeted Therapy - Radioiodine-Refractory Disease:
- Lenvatinib and sorafenib (multi-kinase inhibitors) - approved for RAI-refractory progressive differentiated TC
- BRAF inhibitors (dabrafenib + trametinib) for BRAF V600E-mutant RAI-refractory DTC
Medullary Thyroid Carcinoma
- Surgery is the mainstay - total thyroidectomy with central neck dissection; lateral neck dissection if lateral nodal disease
- Exclude pheochromocytoma first in all RET mutation carriers before surgery (risk of hypertensive crisis)
- No RAI - MTC does not take up radioiodine
- External beam radiation - palliative for unresectable or metastatic disease
- Vandetanib and cabozantinib - approved kinase inhibitors (targeting RET, VEGFR, EGFR) for advanced/metastatic MTC; provide improved progression-free survival
- Selpercatinib - selective RET inhibitor with high response rates in RET-mutant MTC (2020 FDA approval); pralsetinib is an alternative
- Genetic testing - all patients with MTC should be tested for RET germline mutations; positive results trigger cascade testing of first-degree relatives
Anaplastic Thyroid Carcinoma
- Prognosis is dismal - median survival 3-6 months; nearly 100% mortality (Harrison's, p. 3092)
- RAI is usually ineffective (loss of iodine uptake)
- Multimodal approach:
- Surgery (if resectable) - debulking may relieve airway obstruction
- External beam radiation therapy - can be continued if tumors are responsive; often combined with chemotherapy
- Chemotherapy - anthracyclines (doxorubicin), paclitaxel, cisplatin; generally ineffective as monotherapy
- BRAF V600E + MEK inhibitor - dabrafenib + trametinib received FDA approval (2018) for BRAF V600E-mutant ATC; response rates ~69%, some durable responses; the first effective regimen for ATC
- Clinical trial enrollment is strongly encouraged
Thyroid Lymphoma
- Most arise in background of Hashimoto's thyroiditis
- Most common type: diffuse large B-cell lymphoma (DLBCL)
- Highly sensitive to external beam radiation when localized
- Surgery should be avoided as initial therapy (may spread localized disease)
- For disseminated disease: systemic lymphoma protocols (R-CHOP)
8. Follow-up
Differentiated Thyroid Cancer
Serum Thyroglobulin (Tg):
- Sensitive marker for residual or recurrent disease after total thyroidectomy + RAI ablation
- Modern assays with functional sensitivity ~0.1 ng/mL
- Anti-Tg antibodies must be measured simultaneously (interfere with Tg assay)
- Rising Tg or anti-Tg antibodies after initial ablation indicate recurrence
Neck Ultrasound:
- Performed approximately 6 months after thyroid ablation; more sensitive than whole-body scan for detecting cervical LN recurrence
- Continued at regular intervals based on risk
Whole-body RAI scan (WBS):
- Post-treatment WBS after ¹³¹I therapy confirms uptake and identifies metastatic disease
- Stimulated WBS (with TSH elevation) used in high-risk or biochemical-incomplete-response patients
Dynamic Risk Stratification at follow-up (Sabiston, p. 1521):
- Excellent response - 1-4% recurrence risk; follow-up can be relaxed
- Biochemical incomplete - 50% achieve NED with time or additional therapy
- Structural incomplete - disease-specific mortality up to 11% (locoregional) to 50% (distant)
- Indeterminate - 15-20% develop structural disease; continued monitoring
Interval summary:
- Years 1-2: Tg every 6-12 months + neck ultrasound at ~6 months then annually
- Years 3-5: Annual Tg + ultrasound (longer intervals if excellent response)
- Long-term: Low-risk patients with undetectable Tg after lobectomy only require TSH + Tg annually
Medullary Thyroid Carcinoma
- Serum calcitonin - primary marker for residual/recurrent disease; measured at 2-3 months post-op, then every 6 months
- CEA - concurrent monitoring; rapid CEA rise without calcitonin rise suggests dedifferentiation
- Neck ultrasound - every 6 months
- CT chest/abdomen, bone scan, MRI liver - for elevated calcitonin or suspected distant metastases
- RET mutation-positive family members - annual calcitonin screening; prophylactic thyroidectomy timing based on ATA risk category
Anaplastic Thyroid Carcinoma
- Imaging (CT neck/chest/abdomen) every 2-3 months given the aggressive disease course
- Follow-up for treatment response and palliative needs
Sources: Robbins & Kumar Basic Pathology, pp. 736-741 | Harrison's Principles of Internal Medicine 22E, pp. 3088-3095 | Sabiston Textbook of Surgery, pp. 1509-1525 | Cummings Otolaryngology, pp. 2368-2375
Recent evidence note: A 2026 systematic review (PMID 41791888) supports active surveillance as a viable approach for locoregional recurrent differentiated thyroid cancer in selected patients, aligning with the current trend toward less aggressive management for low-risk disease.
Detailed notes on minimally invasive procedures for thyroid surgery and list out recent advances in thyroid surgery (malignant and non malignant)
Reading File
Finding Sources
Finding Sources
Searching PubMed
"thyroid surgery" AND "minimally invasive" AND "robotic"
Searching the Web
recent advances minimally invasive thyroid surgery 2024 2025 techniques robotic endoscopic
Finding Sources
Finding Sources
Reading Article
PMID: 41173534
Reading Article
PMID: 41182840
Reading File
Reading File
Searching PubMed
"thermal ablation" AND "thyroid" AND "radiofrequency"
Reading File
Finding Sources
Reading Article
PMID: 37604507
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC12385003
Finding Sources
Reading File
Searching PubMed
"fluorescence" AND "parathyroid" AND "thyroidectomy"
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC12799353
Finding Sources
Finding Sources
Searching PubMed
"active surveillance" AND "thyroid microcarcinoma"
Reading File
Reading File
Reading File
I now have comprehensive information from multiple sources. Let me compile the complete, detailed notes.
Minimally Invasive Thyroid Surgery: Detailed Notes & Recent Advances
PART 1: MINIMALLY INVASIVE PROCEDURES FOR THYROID SURGERY
Historical Background
Minimally invasive thyroid surgery dates to 1996 when Gagner performed the first endoscopic parathyroidectomy, using 5 mm laparoscopic instruments placed between the platysma and strap muscles with CO2 insufflation. This was followed by minimally invasive video-assisted thyroidectomy (MIVAT), which evolved through cervical, axillary, and anterior chest wall approaches. (Scott-Brown's Otorhinolaryngology Vol 3, p. 521)
The fundamental goal of all minimally invasive techniques is to reduce the cosmetic impact of the standard 5-8 cm anterior cervicotomy incision. Approaches are broadly categorized as:
- Cervical minimally invasive - smaller incision in standard location
- Remote access - incision placed away from the neck entirely
A. Cervical Minimally Invasive Approaches
1. Mini-Open / Small-Incision Thyroidectomy
- Cervicotomy reduced from 6-8 cm to 3-4 cm using standard instruments
- With endoscopic assistance: 1.5-2.5 cm incision
- Terminology: minimally invasive, video-assisted, videoscopic/endoscopic, mini-open
- All demonstrate reasonable feasibility and safety in carefully selected patients
2. Minimally Invasive Video-Assisted Thyroidectomy (MIVAT)
- Introduced by Miccoli (Italy) in 1999
- Incision: 1.5-2 cm suprasternal central cervical incision
- Uses 5 mm 30-degree endoscope + conventional instruments (no gas insufflation needed)
- Patient selection: Thyroid nodule ≤3.5 cm, total gland volume ≤25 mL, no previous neck surgery/irradiation, no thyroiditis
- Advantages: Direct access, no remote flap dissection, preserves cosmetic benefit of small scar
- The endoscope provides excellent magnified visualization of RLN, superior laryngeal nerve, and parathyroid glands (see illustration below)
(Cummings Otolaryngology, p. 2391)
B. Remote Access Approaches
All remote access techniques place incisions in anatomically hidden areas, requiring subcutaneous/subplatysmal tunneling with laparoscopic or robotic instruments. They can be performed with CO2 gas insufflation or gasless technique using custom long-tunneled retractors.
The four principal remote access approaches are:
- Transaxillary
- Bilateral Axillo-Breast Approach (BABA)
- Retroauricular (facelift/hairline)
- Transoral (TOETVA)
(2025 International Consensus Statement - PMID 41173534)
1. Transaxillary Thyroidectomy
History: Transaxillary thyroidectomy using laparoscopic instruments was first described in Japan in 2000 but gained traction in the United States in 2007 based on excellent South Korean results using a robotic gasless technique with a single axillary incision. The first robotic thyroidectomy using this approach was reported in 2009.
Technique:
- Single 5-6 cm incision in the axilla (or hairline of axilla)
- Gasless technique: subcutaneous tunnel created with long custom retractors
- CO2-assisted variant also used
- Robotic arms + endoscope traverse tunnel from axilla to thyroid
- Da Vinci system provides 3D visualization, 540° of wristed instrumentation, motion scaling
Outcomes (North American series, n=301):
- Conversion to open thyroidectomy: 1 case
- Permanent RLN injury: 1.3%
- Permanent hypoparathyroidism: 1.1%
- Neck hematoma: 0.3%
- Approach-specific complication (arm lymphedema): 1 case, resolved conservatively
- Zero cancer recurrences among 133 patients with histologic malignancy (Sabiston, p. 1529)
Initial setbacks in the US: Upsurge of complications (brachial plexus injury, tracheoesophageal injury, lymph leak, hematoma) due to inadequate surgeon training and aggressive device marketing. FDA issued warnings in 2013, and Intuitive Surgical withdrew support. Reintroduction followed at high-volume centers.
Patient selection criteria (from 2025 International Consensus):
- Benign or malignant thyroid disease without ETE or lateral nodal metastases
- Thyroid volume not excessively large (varies by guideline, typically <10 cm in dominant dimension)
- No prior neck surgery
- Patient preference for cosmetic outcome
2. Bilateral Axillo-Breast Approach (BABA)
- Three or four small port incisions: one in each axilla + one or two periareolar incisions
- Creates working space over anterior chest/subcutaneous tissue with CO2 insufflation or gasless retraction
- Advantage: Bilateral thyroid access possible from symmetric ports; symmetric cosmetic incisions hidden in natural creases
- Disadvantage: Larger skin flap area than transaxillary; longer dissection tunnel
- Widely adopted in East Asia; growing use with robotic assistance (robotic BABA)
- Has been used for total thyroidectomy + central neck dissection
3. Retroauricular / Facelift Approach
Technique:
- Single incision in the retroauricular hairline (facelift incision)
- Tunnel dissection over the sternocleidomastoid to the thyroid
- Robotic assistance (Terris 2012 series, n=15): demonstrated shorter operative time vs transaxillary; amenable to outpatient setting
Advantages:
- Incision hidden in hairline - not visible frontally
- Shorter operative tunnel than transaxillary
- Can be performed ambulatory/outpatient
Disadvantages:
- Unilateral access; contralateral lobe access more limited
- Risk of greater auricular nerve injury
- Requires familiarity with facelift dissection planes
(Scott-Brown's Otorhinolaryngology Vol 3, p. 521; Sabiston, p. 1529)
4. Transoral Endoscopic Thyroidectomy Vestibular Approach (TOETVA)
The only approach that eliminates any skin incision.
Technique (popularized in Thailand by Anuwong):
- Three port incisions in the oral vestibule (inside the lower lip) - not through oral mucosa
- Uses CO2 gas insufflation
- Central 10 mm trocar + two 5 mm lateral trocars
- Standard laparoscopic instruments or robotic adaptation
- Mental nerve at risk during lateral trocar placement (must stay medial to canine teeth)
Largest published series (n=425, Thailand):
- Permanent RLN injury: 0%
- Permanent hypoparathyroidism: 0%
- Neck hematoma requiring open thyroidectomy: 1 case
- Intraoperative conversion: 3 cases
- Transient mental nerve palsy: 0.7% (3 patients)
- Postoperative infection: 0% (Sabiston, p. 1530)
Concerns addressed: Initial fears about oral flora contamination and infection have not been borne out in large series. Strict antibiotic prophylaxis and preoperative oral decontamination are used.
Robotic TOETVA (TORT - Transoral Robotic Thyroidectomy): Da Vinci SP (single-port) system adaptation is being studied. The flexible 3D endoscope + 3 wristed instruments in a single 2.5 cm cannula allows this approach.
Indications: Benign nodules/goiter, low-risk differentiated TC without ETE or large nodal disease. NOT recommended for T3b/T4 tumors.
Comparison of Remote Access Approaches
| Feature | Transaxillary | BABA | Retroauricular | TOETVA |
|---|---|---|---|---|
| Skin incision | Axilla | Axilla + areola | Hairline | None |
| Gas/gasless | Both | CO2 or gasless | Both | CO2 |
| Bilateral access | Limited | Yes | Limited | Yes |
| Cosmesis | Excellent | Excellent | Excellent | Best (no scar) |
| Approach complications | Brachial plexus, lymphedema | Skin flap seroma | Greater auricular nerve | Mental nerve palsy |
| Central neck dissection | Yes (with robotic) | Yes | Limited | Yes |
| Learning curve | High | High | Moderate | High |
| Adoption | US, Korea | Korea, China | US (niche) | Thailand, Asia, growing globally |
(Sabiston Textbook of Surgery, p. 1529-1530; 2025 International Consensus [PMID 41173534])
C. Non-Surgical Ablative Procedures (Percutaneous Minimally Invasive)
These image-guided techniques avoid surgery entirely and are performed under ultrasound guidance.
1. Ethanol (Alcohol) Ablation
- 95-99% dehydrated ethanol injected under US guidance
- Mechanism: coagulative necrosis (cellular dehydration) + ischemic necrosis (small vessel thrombosis)
- Best indication: predominantly cystic thyroid nodules (recurrence after aspiration alone is common)
- Very effective for cystic lesions; less effective for solid nodules
- Low cost; minimal equipment
2. Radiofrequency Ablation (RFA)
Mechanism: High-frequency alternating current (200-1200 kHz) agitates tissue ions causing friction-induced heat, leading to coagulative necrosis. Performed via a single internally cooled electrode using a "moving shot" technique under US guidance.
Indications (established):
- Symptomatic benign nonfunctional thyroid nodules with ATA very low to low suspicion (ACR TI-RADS 1-3) or intermediate suspicion (TI-RADS 4) with benign cytology - two benign biopsies required
- Autonomous functioning nodules (toxic adenoma) with contraindications to RAI or surgery (resolution of hyperthyroidism is less predictable)
Outcomes:
- Nodule volume reduction: 65% at 6 months, 77% at 12 months
- Improvement in compressive symptoms and cosmesis
- Better preservation of thyroid function vs surgery
- Better health-related quality of life vs surgery (Sabiston, p. 1530)
For malignant disease: RFA has been explored for recurrent papillary TC and papillary thyroid microcarcinoma (PTmC) but is not first-line treatment. A systematic review and meta-analysis (n=36 studies, PMID 37604507) found:
- Local recurrence: 2% (RFA), 2% (microwave), 3% (laser)
- Lymph node metastasis: 1% (RFA, lowest)
- No distant metastasis events
- RFA showed superior outcomes in most measures for T1N0M0 PTC
- Not recommended for indeterminate nodules (no histology, risk of tumor progression with incomplete treatment)
Complications: Voice change (1.4%), thyroid nodule rupture, hematoma, tracheal necrosis (rare).
3. Microwave Ablation (MWA)
- Electromagnetic field (900-2500 MHz) oscillates polar water molecules to generate heat
- Achieves higher temperatures and larger ablation zones faster than RFA
- Advantage: Less susceptible to heat-sink effect near blood vessels
- Complication rate higher than RFA (13% minor complications in meta-analysis)
- Complete disappearance rate: 71% vs 93% for laser
4. Laser Ablation (LA)
- Single or multiple optical fibers deliver focused laser energy causing thermal coagulation
- Higher complete disappearance rate (93%) than RFA or MWA in meta-analysis
- Local recurrence: 3%
- Minor complication rate 6%
5. High-Intensity Focused Ultrasound (HIFU)
- Ultrasound waves focused to generate heat at target location
- Microbubble formation via cavitation causes hemorrhagic necrosis
- Non-invasive - no needle/probe insertion; entirely external device
- Limited penetration depth; precise targeting required
- Approved in Europe; growing evidence base
PART 2: RECENT ADVANCES IN THYROID SURGERY (2023-2026)
A. Surgical Technique Advances
1. Single-Port (SP) Robotic Thyroidectomy (da Vinci SP System)
The most significant recent robotic development. The da Vinci SP system combines a flexible 3D endoscope + 3 wristed instruments in a single 2.5 cm cannula, eliminating external arm collisions that were the main limitation of multiport robotic systems.
Access routes available:
- SP Transaxillary - most studied; STAR-RND (Single-port Transaxillary Radical Neck Dissection) and GOSTA-RND approaches allow radical neck dissection with lymph node yields of 25-30, operative times 180-220 minutes
- SP Areolar (SPRA) - periareolar single-port approach
- SP Hairline (retroauricular) - single-port variant
- SP Transoral (TORT) - under development
Clinical outcomes (as of November 2025): SP thyroidectomy is feasible and safe in well-selected patients with high cosmetic satisfaction. Learning curve data suggest proficiency after 20-30 cases for experienced robotic surgeons. (PMC12799353)
2. 2025 International Consensus Statement on Remote-Access Surgery
A landmark 2025 consensus (PMID 41173534) from 6 major international societies (Asia-Pacific Society of Thyroid Surgery, ATA, AHNS, AAES, ESES, LATS) established 23 consensus statements covering:
- Minimum surgeon volume requirements for safe practice
- Structured training pathways including cadaveric dissection and proctoring
- Patient eligibility criteria based on disease characteristics
- Oncologic outcomes comparable to open surgery with experienced surgeons
- Improved cosmetic satisfaction
- Development of high-volume centers of excellence recommended
3. 2025 ATA Guidelines Update - Surgical Management Changes
Key surgical management updates in the 2025 ATA DTC Guidelines:
- Lobectomy increasingly preferred for low-risk DTC, expanding beyond prior 2015 thresholds
- Active surveillance recommendations for very low-risk papillary microcarcinoma - avoidance of immediate surgery for select patients
- Detailed guidance on intraoperative parathyroid management (Recommendation 24) - devascularized glands should undergo autotransplantation with frozen section confirmation
- Therapeutic central neck dissection (level VI + upper VII) for clinically involved central nodes (strong recommendation, moderate certainty)
B. Intraoperative Technology Advances
4. Near-Infrared Autofluorescence (NIRAF) for Parathyroid Identification
- Parathyroid tissue emits autofluorescence at 820 nm when excited with near-infrared laser (discovered ~2008; now FDA-approved devices)
- FDA-approved products: PTeye (probe-based; AiBiomed) and Fluobeam-800 (image-based; Fluoptics)
- Sensitivity and accuracy >90% for parathyroid detection
- Limitation: Cannot differentiate healthy vs diseased parathyroid; cannot assess viability; penetration limited to ~5 mm (only useful once gland is exposed)
- Replaces intraoperative frozen section/aspiration for PTH in many centers, potentially reducing operative time
- NOT yet routine but gaining adoption (Fischer's Mastery of Surgery, p. 1172; Schwartz's, p. 1686)
5. Indocyanine Green (ICG) Perfusion Angiography
- IV injection of ICG used with near-infrared camera to generate intraoperative perfusion map of parathyroid glands and their vascular pedicles
- Predicts which parathyroid glands will remain viable after thyroidectomy
- Helps decide which devascularized glands require autotransplantation
- Evidence: reduces permanent hypoparathyroidism rates post-thyroidectomy
- Meta-analysis (PMID 40225464): Image-based NIRAF showed superior sensitivity vs probe-based for parathyroid identification
6. Continuous Intraoperative Neuromonitoring (CIONM)
- Evolution from intermittent to continuous RLN monitoring during thyroidectomy
- Intermittent: periodic direct stimulation and laryngeal palpation
- CIONM: EMG-based continuous system via endotracheal tube electrodes provides real-time warning before impending RLN injury
- Allows the surgeon to pause and reposition before permanent injury occurs
- Current evidence: Multiple studies confirm feasibility; however, no large RCT has proven superiority over intermittent monitoring in reducing injury rates when RLN is routinely visualized (Schwartz's, p. 1686)
- Most useful in reoperative thyroid surgery, large goiters, and thyroid malignancy with ETE
C. Non-Surgical Minimally Invasive Advances (Ablation for Malignancy)
7. Thermal Ablation for Low-Risk Papillary Thyroid Microcarcinoma (PTmC)
A major paradigm shift for low-risk disease:
Evidence base:
- Systematic review and meta-analysis (PMID 37604507, n=36 studies): RFA, MWA, and laser ablation all reliable for T1N0M0 PTC; RFA shows best overall outcomes
- 3-year follow-up RFA meta-analysis for PTmC (PMID 38870871): Low local recurrence (~2%), no distant metastases
- 2026 Ontario Health Technology Assessment (PMID 42311839): Ablative technologies for thyroid nodules formally assessed; supports use for benign disease; evidence for malignancy still maturing
Current guideline position: Not yet first-line for malignancy per ATA/ETA; recommended only for patients who refuse surgery or have contraindications. Ongoing international trials comparing active surveillance vs ablation vs surgery for PTmC.
8. Thermal Ablation for Indeterminate Nodules (Bethesda III/IV)
- 2025 systematic review (PMID 40658618): Thermal ablation for indeterminate nodules reduces nodule volume and symptoms
- Major caveat: absence of histology means malignancy cannot be fully excluded; close follow-up mandatory
- Being studied as a bridge or alternative to diagnostic lobectomy in selected Bethesda III cases
9. Quality of Life Data for Benign Disease
- 2025 systematic review (PMID 41213637): Thermal ablation of benign nodules results in significant QoL improvement; comparable or superior to surgical outcomes for symptom control
D. Advances in Management Strategy
10. Active Surveillance for Papillary Thyroid Microcarcinoma
- Japanese Kuma Hospital and Cancer Institute Hospital data (20+ years) established that most PTmC (<1 cm) grow very slowly and rarely progress
- Now incorporated into ATA 2025 guidelines as an accepted alternative to immediate surgery for selected low-risk PTmC
- Criteria: unifocal, intrathyroidal, no LN/distant mets, not adjacent to RLN or trachea, no aggressive histologic features
- A 2026 meta-analysis (PMID 41452620, JAMA Otolaryngol) comparing patient-reported outcomes across treatment strategies (active surveillance, ablation, surgery) for PTmC supports active surveillance as having excellent outcomes with lower treatment burden
11. Active Surveillance for Locoregional Recurrent DTC
- 2026 systematic review and meta-analysis (PMID 41791888, Thyroid): Active surveillance is viable for selected patients with locoregional recurrent DTC, particularly small (<1 cm) cervical nodal metastases with low growth kinetics
12. Lobectomy vs Total Thyroidectomy - Expanding Lobectomy Indications
- Large observational data (SEER, NCDB) confirmed equivalent survival between lobectomy and total thyroidectomy for DTC 1-4 cm without high-risk features
- ATA 2025 guidelines expand lobectomy indications; total thyroidectomy reserved for high-risk disease
- 2025 systematic review (PMID 40915491) on lobectomy vs total thyroidectomy specifically in pediatric DTC shows comparable oncologic outcomes
E. Molecular and Technological Advances
13. Molecular Profiling to Guide Surgery
- ThyroSeq v3, Afirma GSC, ThyGenX/ThyraMIR - gene expression classifiers for indeterminate (Bethesda III/IV) FNA cytology
- Allows "rule out" malignancy → avoidance of diagnostic lobectomy for benign nodules
- Allows "rule in" high-risk mutations (BRAF, TERT, RET fusions) → guide extent of surgery (lobectomy vs total thyroidectomy)
- High-risk molecular profiles (BRAF + TERT co-mutation) favor total thyroidectomy even for smaller tumors
14. Fluorescence-Guided Sentinel Lymph Node Biopsy
- ICG-based sentinel node mapping for thyroid cancer being explored
- May reduce extent of central neck dissection in low-risk PTC by accurately identifying sentinel nodes
- Still investigational; not yet standard of care
15. AI-Assisted Ultrasound and Surgical Navigation
- AI-based ultrasound risk stratification systems increasingly validated
- Computer vision tools for intraoperative RLN recognition being developed
- Augmented reality overlay systems for thyroid surgery orientation under investigation
F. Energy Devices for Hemostasis
16. Advanced Energy Devices
- Harmonic scalpel (ultrasonic coagulation) and LigaSure (vessel sealing) now standard in most thyroid centers
- Reduce operative time, decrease blood loss, and reduce need for suture ligation of inferior thyroid artery branches
- Meta-analyses confirm reduced operative time by ~20-30 minutes and lower drain output compared to traditional cold-knife/suture technique
- Thermal spread is the key safety concern near RLN - energy devices must be kept >3 mm from the nerve
Summary Table: Recent Advances at a Glance
| Domain | Advance | Year / Status |
|---|---|---|
| Robotic surgery | Single-port da Vinci SP thyroidectomy | 2020s - actively studied |
| Remote access | 2025 International Consensus Statement | 2025 - published |
| Guidelines | 2025 ATA DTC Management Guidelines | 2025 - major update |
| Parathyroid preservation | NIRAF + ICG angiography | FDA approved; growing adoption |
| Nerve protection | Continuous intraoperative RLN monitoring | Widely available; evidence accumulating |
| Ablation - benign | RFA, MWA, laser, HIFU for benign nodules | Established; guideline-endorsed |
| Ablation - malignant | RFA/MWA for PTmC | Promising; not yet first-line per ATA |
| Ablation - indeterminate | Thermal ablation for Bethesda III/IV | Under investigation |
| Strategy - benign | Expanded active surveillance for low-risk PTC | 2025 ATA guidelines |
| Strategy - malignant | Lobectomy preferred for low-risk DTC 1-4 cm | Expanded in 2025 ATA |
| Molecular | Gene expression classifiers guiding surgery | Established (ThyroSeq v3, Afirma GSC) |
| Oncology | Dabrafenib + trametinib for BRAF+ ATC | FDA approved 2018; changing ATC outcomes |
Sources:
- Sabiston Textbook of Surgery, pp. 1529-1530
- Scott-Brown's Otorhinolaryngology (Vol 3), p. 521
- Schwartz's Principles of Surgery 11E, p. 1686
- Fischer's Mastery of Surgery 8E, p. 1172
- Cummings Otolaryngology, p. 2391
- 2025 International Consensus on Remote-Access Thyroidectomy (PMID 41173534)
- Thermal ablation for T1N0M0 PTC - Meta-analysis (PMID 37604507)
- RFA for PTmC 3-year follow-up (PMID 38870871)
- Patient-reported outcomes in PTmC treatment (PMID 41452620)
- Single-port robotic thyroidectomy review 2025 (PMC12799353)
This is a shared conversation. Sign in to Orris to start your own chat.