Complications of tb full details for md exam answer 15 marks
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed. Let me compile the comprehensive MD exam answer.
Complications of Tuberculosis — MD Exam Answer (15 Marks)
Introduction
Tuberculosis (TB), caused by Mycobacterium tuberculosis, produces a wide spectrum of complications — both pulmonary (local) and extrapulmonary (systemic). Complications arise from direct tissue destruction, immune-mediated injury, haematogenous dissemination, and sequelae of healed disease. Understanding them is critical for management and prognosis.
A. PULMONARY COMPLICATIONS
1. Hemoptysis
The most common and clinically urgent pulmonary complication. Two forms:
- Minor hemoptysis: Rupture of blood vessels within areas of lung parenchymal destruction — very common in active disease.
- Massive hemoptysis (≥600 mL/24 h): Life-threatening. Mechanisms include:
- Rasmussen aneurysm: Erosion of a tuberculous cavity into a pulmonary artery → pseudoaneurysm formation → potentially fatal bleeding
- Aspergilloma superinfection of a healed TB cavity (see below)
- Tumor development in scarred lung eroding bronchial/pulmonary vessels
Management of massive hemoptysis: Large-bore ET tube (≥8 mm), position bleeding lung dependently, selective bronchus intubation, emergency bronchoscopy, surgical resection, or selective bronchial artery embolization.
2. Pneumothorax
Occurs in <5% of patients with severe cavitary disease. Mechanisms:
- Rupture of a tuberculous cavity into the pleural space
- Rupture of a subpleural bleb
- Formation of bronchopleural fistula
Untreated pneumothorax → progressive pleural infection → fibrosis → trapped lung. Treatment: tube thoracostomy with suction.
3. Pleural Effusion (Tuberculous Pleuritis)
- Occurs early after primary infection or late in post-primary cavitary disease
- Often self-limiting but 65% relapse rate if untreated; active TB develops within 5 years
- Fluid characteristics: Exudate, protein >50% serum protein, WBC 500–2500 cells/mL (lymphocyte predominant), low glucose; AFB smear rarely positive, cultures positive in only 25–30%
- Late complication: empyema necessitans — empyema eroding through chest wall forming sinus tract
4. Empyema
- Extensive parenchymal disease and cavitation → cavity ruptures into pleural space
- More common late in the disease; often catastrophic; associated with bronchopleural fistula
- Untreated: spontaneous pleuro-cutaneous fistula, chest wall mass, rib and vertebral destruction
5. Airway Tuberculosis (Endobronchial TB)
When a cavity drains into the bronchial tree:
- Bronchiectasis: Most common complication of endobronchial TB
- Bronchial stenosis: From endobronchial TB or direct extension from tuberculous adenitis
- Radiographic appearances: persistent segmental/lobar collapse, lobar hyperinflation, obstructive pneumonia
- Laryngeal TB: Highly infectious; proximal extension of lower airway disease; patients almost always have active pulmonary TB
6. Superinfection with Fungi (Aspergilloma)
- Healed TB leaves open cavities and areas of bronchiectasis prone to colonization
- Aspergilloma (fungus ball): Aspergillus fumigatus most common; ball of fungal mycelium within cavity, shows the "air crescent sign" on CXR/CT
- Clinical significance: can cause massive fatal hemoptysis

7. Respiratory Failure / Cor Pulmonale
- Extensive bilateral disease → progressive destruction of lung parenchyma → restrictive and obstructive defects → hypoxia → pulmonary hypertension → cor pulmonale → right heart failure
- ARDS may develop in fulminant miliary TB
B. EXTRAPULMONARY COMPLICATIONS
Extrapulmonary TB is more common in infants, elderly, and immunocompromised (especially HIV). Sites in decreasing frequency: lymphatic > pleural > bone/joint > genitourinary > meningeal > peritoneal > others.
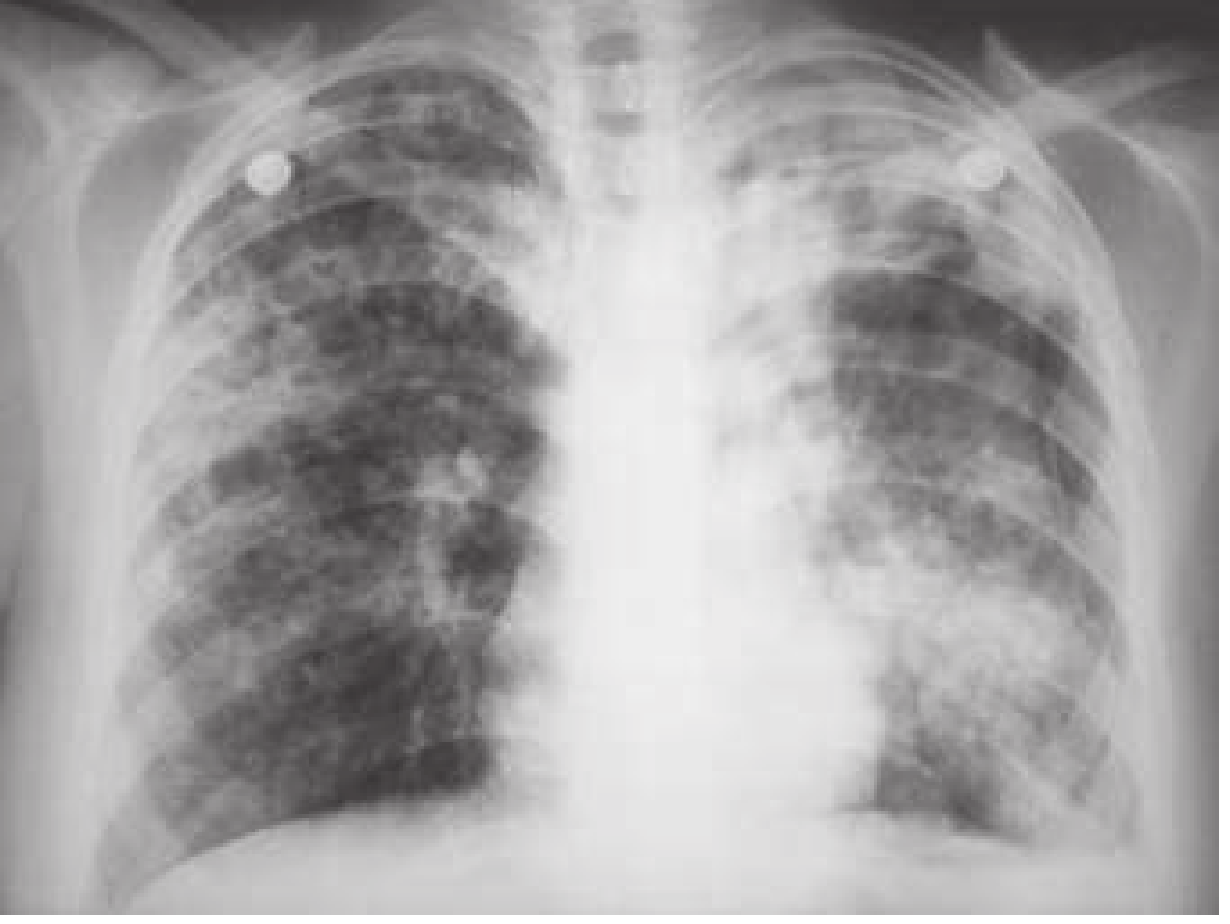
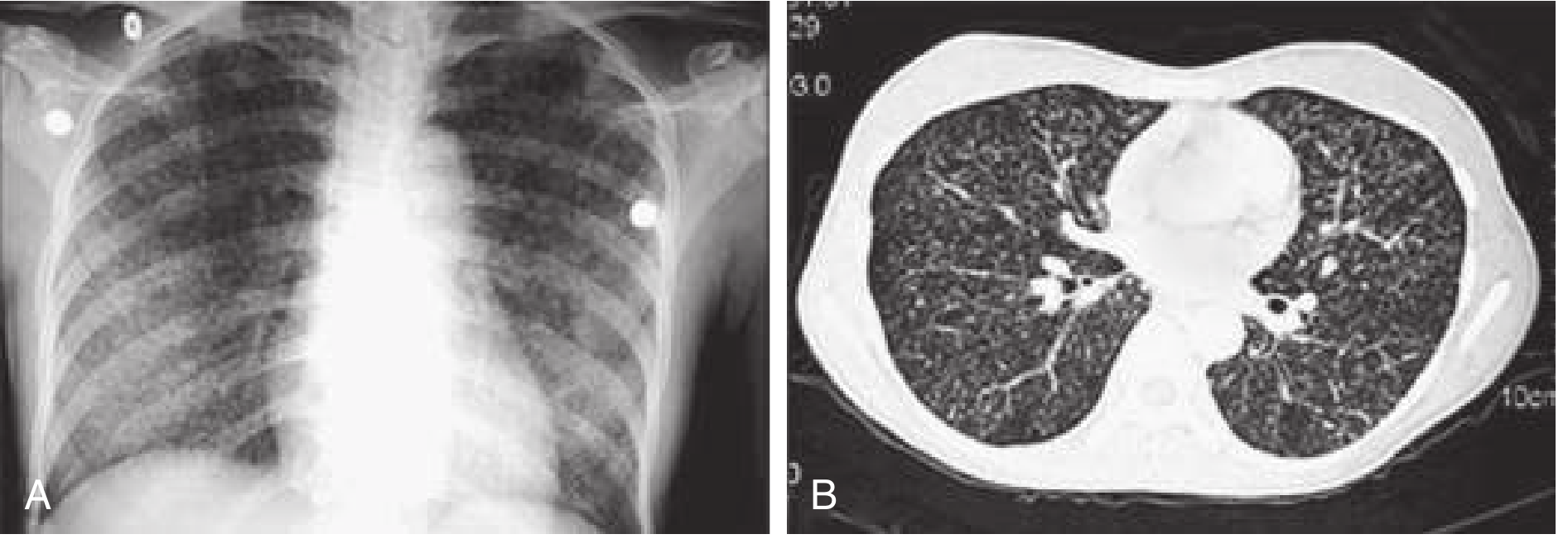
8. Miliary (Disseminated) Tuberculosis
- Haematogenous dissemination → seeding of multiple organs simultaneously
- Classic CXR: 1–3 mm discrete "millet seed" opacities uniformly distributed bilaterally
- Mortality ~21% (high due to delayed treatment)
- Fulminant form: ARDS + DIC
- Treatment must be initiated on clinical suspicion — do not await confirmation
9. Tuberculous Meningitis (CNS TB)
Accounts for ~6% of extrapulmonary TB. Peak incidence: neonates to 4-year-olds.
Pathogenesis: Rupture of a subependymal tubercle into the subarachnoid space (not direct haematogenous seeding). In miliary TB, meningitis develops within weeks.
Pathological changes at base of brain:
- Vasculitis → aneurysm, thrombosis, haemorrhagic infarction
- Basal ganglia vessel involvement → lacunar infarcts, movement disorders
- Middle cerebral artery → hemiplegia
Clinical stages:
| Stage | Features |
|---|---|
| Prodromal (1–2 wk) | Malaise, intermittent headache, low-grade fever |
| Meningitic (2–3 wk) | Protracted headache, vomiting, meningismus |
| Coma stage | Focal signs, cranial nerve palsies, coma |
Key features:
- Diplopia from basilar exudate in up to 70%
- SIADH → hyponatremia (common)
- CSF: lymphocytic pleocytosis (0–1500 WBC/mL), elevated protein, low glucose
- Classic CT/MRI triad: basal meningeal enhancement + hydrocephalus + cerebral/brainstem infarction
- Tuberculomas may be seen as round parenchymal lesions
10. Tuberculous Pericarditis
- From direct extension of infection from tracheobronchial tree, mediastinal/hilar lymph nodes, sternum, or spine; or haematogenous seeding in miliary TB
- Leading cause of pericarditis in HIV-infected patients in the US
Complications:
- Pericardial effusion → cardiac tamponade
- Constrictive pericarditis (most feared) → fibrous obliteration of pericardial space → impaired diastolic filling → right heart failure
- Myocarditis
- Aortic regurgitation (rare)
Corticosteroids are used to reduce the risk of constriction (evidence-based adjunct).
11. Lymphadenitis (Scrofula)
- Most common form of extrapulmonary TB
- Most commonly in young women and children
- Site: anterior/posterior cervical chain or supraclavicular fossa
- Stages: discrete rubbery nodes → matted → fluctuant → collar-stud abscess → sinus tract
- Diagnosis: fine-needle aspiration (sensitivity 77%, specificity 93%)
- Complication: permanent sinus formation if incision and drainage performed
12. Skeletal TB (Pott's Disease)
- Spinal TB (Pott's disease): 50–70% of skeletal TB; usually thoracic/lumbar vertebrae
- Hip/knee: 15–20%; other joints: 15–20%
- Pathogenesis: reactivation of dormant lesions seeded during primary bacteraemia; or contiguous spread from paravertebral nodes
Features of Pott's disease:
- Back pain/stiffness; kyphosis (gibbus deformity)
- Paraspinal cold abscess in >50% → sinus tract formation
- Skip lesions (abscess tracking up/down spine sparing vertebral bodies)
- Main complication: spinal cord compression → paraplegia (Pott's paraplegia)
- Intervertebral disc space narrowing on imaging (loss of disc height) — hallmark finding
13. Genitourinary TB
- Haematogenous seeding → granulomas, scarring, obstruction anywhere in urinary tract
- Classic finding: sterile pyuria (pyuria in acidic urine with no organisms on culture)
- Urinalysis: pyuria, hematuria, albuminuria
Complications:
- Nephrolithiasis
- Ureteral obstruction or reflux
- Recurrent bacterial UTIs
- Hypertension
- Papillary necrosis
- Renal insufficiency
- Autonephrectomy (complete calcification and destruction of kidney — "putty kidney")
- Rare: transitional cell carcinoma in scarred tissue
- Males: tuberculous epididymo-orchitis (commonest form of male genital TB)
14. Gastrointestinal and Peritoneal TB
GI TB:
- Most common site: ileocaecal region (owing to abundance of lymphoid tissue and slow transit)
- Features: pain, anorexia, diarrhea, obstruction, hemorrhage, palpable mass
- Can mimic: appendicitis, Crohn's disease, carcinoma, acute abdomen
- Anal TB: fissures, fistulae, perirectal abscesses
Tuberculous Peritonitis:
- From local spread (lymph node/intestinal focus/infected fallopian tube) or miliary seeding
- Features: abdominal pain, distension, fever, anorexia, weight loss
- Ascites: exudative, 500–2000 cells/mL, lymphocyte predominant; AFB smear low yield
- Can mimic alcoholic hepatitis or cirrhosis with ascites
- Peritoneal biopsy often required for diagnosis
15. Other Extrapulmonary Sites
| Site | Complication |
|---|---|
| Adrenal glands | Bilateral adrenal destruction → Addison's disease (adrenal insufficiency) |
| Eye | Choroiditis, iritis, phlyctenular conjunctivitis |
| Skin | Lupus vulgaris, erythema nodosum, scrofuloderma |
| Liver/spleen | Hepatosplenomegaly in miliary disease |
| Larynx | Highly contagious, hoarseness, dysphagia |
C. COMPLICATIONS RELATED TO IMMUNE RESPONSE
Immune Reconstitution Inflammatory Syndrome (IRIS)
- Occurs in HIV-positive patients starting antiretroviral therapy while on TB treatment
- Paradoxical worsening of TB symptoms despite adequate treatment
- Due to restored immune response attacking residual mycobacterial antigens
D. COMPLICATIONS RELATED TO TREATMENT
| Drug | Complication |
|---|---|
| Isoniazid (INH) | Peripheral neuropathy (pyridoxine deficiency), hepatotoxicity, drug-induced lupus, seizures (overdose) |
| Rifampicin | Hepatotoxicity, drug interactions (CYP450 inducer), orange discolouration of secretions, thrombocytopenia |
| Pyrazinamide | Hepatotoxicity, hyperuricemia, arthralgia |
| Ethambutol | Retrobulbar neuritis → colour vision defects, reduced visual acuity |
| Streptomycin | Ototoxicity (VIII nerve), nephrotoxicity |
Summary Classification Table
| Category | Complications |
|---|---|
| Pulmonary | Hemoptysis (Rasmussen), pneumothorax, pleural effusion, empyema, bronchopleural fistula, endobronchial TB, bronchiectasis, aspergilloma, cor pulmonale, ARDS |
| Extrapulmonary | Miliary TB/DIC, TB meningitis (hydrocephalus, infarction), pericarditis (constrictive), lymphadenitis (scrofula), Pott's disease (paraplegia), GU TB (autonephrectomy), GI/peritoneal TB, Addison's disease |
| Treatment-related | Hepatotoxicity, peripheral neuropathy, retrobulbar neuritis, ototoxicity, IRIS |
Sources: Rosen's Emergency Medicine (9th Ed.), Goldman-Cecil Medicine, Murray & Nadel's Respiratory Medicine, Adams & Victor's Principles of Neurology, Robbins & Cotran Pathologic Basis of Disease, Jawetz Medical Microbiology.
This is a shared conversation. Sign in to Orris to start your own chat.