I am a medical student currently in 4th year in semey medical kazakstan and today my topic is Malformations of musculoskeletal system Congenital dislocation of the hip-D so give me details of this topic for class discussion
congenital dislocation of the hip developmental dysplasia etiology pathology classification
congenital hip dislocation clinical features diagnosis treatment management
congenital hip dislocation developmental dysplasia imaging diagnosis
Congenital Dislocation of the Hip (CDH) / Developmental Dysplasia of the Hip (DDH)
Note on Terminology: The older term "Congenital Dislocation of the Hip (CDH)" has largely been replaced by Developmental Dysplasia of the Hip (DDH), as the condition represents a spectrum — not just a fixed congenital dislocation — and may develop or worsen postnatally.
1. Definition & Spectrum
- Dysplasia — shallow acetabulum, femoral head in joint but unstable
- Subluxation — partial loss of contact between femoral head and acetabulum
- Dislocation — complete loss of contact (irreducible = Ortolani negative)
- Dislocatable (Barlow positive) — hip is reduced at rest but can be dislocated with provocation
2. Epidemiology
| Parameter | Detail |
|---|---|
| Incidence | ~1–2 per 1,000 live births (frank dislocation); up to 10/1,000 for instability |
| Sex | Females >> Males (6:1 ratio) — due to greater ligamentous laxity under maternal estrogen |
| Laterality | Left > Right > Bilateral (left because of common LOA fetal position pressing left hip against sacrum) |
| Race | More common in Native Americans, Lapps; less common in Africans |
3. Etiology & Risk Factors
Primary Causes:
- Genetic/Familial — positive family history (12× increased risk)
- Ligamentous laxity — maternal relaxin/estrogen crosses placenta, more pronounced in female fetuses
- Acetabular dysplasia — shallow acetabulum fails to adequately cover femoral head
Risk Factors (Mechanical/Positional):
- Breech presentation — most important mechanical risk (10× increased risk)
- First-born child — uterine wall tighter, less amniotic fluid space
- Oligohydramnios
- Swaddling with extended hips (e.g., traditional Navajo or Kazakh swaddling with legs extended)
- Associated conditions: torticollis, clubfoot, metatarsus adductus (other "packaging" defects)
4. Pathological Anatomy
Changes in the Acetabulum:
- Shallow, steeply inclined (increased acetabular index)
- Filled with fibrofatty tissue (pulvinar)
- Limbus (labrum) may be inverted, blocking reduction
Changes in the Femoral Head:
- Small, hypoplastic, delayed ossification
- Coxa valga (increased neck-shaft angle)
- Excessive anteversion of femoral neck
Changes in Soft Tissues:
- Capsule becomes elongated and hourglass-shaped
- Iliopsoas tendon crosses the capsular neck, obstructing reduction
- Short adductors
- Tight contracted ligamentum teres (elongated)
5. Classification
Graf Classification (Ultrasound — Infants <6 months)
| Type | Description | Management |
|---|---|---|
| Type I | Normal hip (α ≥60°) | Observe |
| Type II | Immature or mildly dysplastic (α 43–59°) | Splint if >3 months |
| Type III | Subluxated (cartilaginous roof displaced) | Brace/harness |
| Type IV | Dislocated | Active treatment |
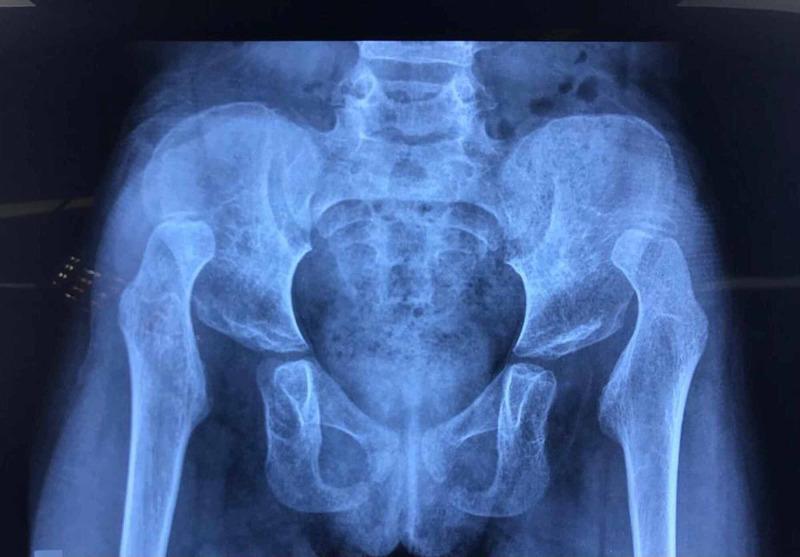
Tönnis Classification (X-ray)
| Grade | Finding |
|---|---|
| I | Femoral head ossification nucleus medial to Perkin's line |
| II | Nucleus below acetabular edge |
| III | Nucleus at level of acetabular edge |
| IV | Nucleus above acetabular edge — complete dislocation |
6. Clinical Features by Age
Newborn / Neonate (0–3 months)
- Ortolani Test ✅ (Reduction test)
- Baby supine, hips flexed 90°, abduct hip — "clunk" felt as dislocated head reduces back in
- Positive = dislocated hip that CAN be reduced
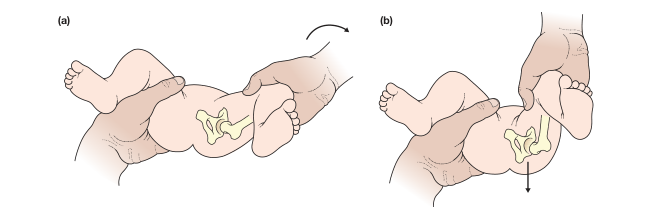
- Barlow Test ✅ (Provocation test)
- Adduct and posteriorly press hip — "clunk" felt as head dislocates out
- Positive = located hip that CAN be dislocated
⚠️ Both tests lose sensitivity after 3 months as soft tissues tighten
Infant (3–18 months)
- Limited hip abduction (<60°) on the affected side — most reliable sign
- Galeazzi sign (Allis sign) — knee on affected side appears lower when hips and knees flexed (femoral shortening)
- Asymmetric skin folds (less reliable)
- Leg length discrepancy
Toddler (Walking age, 1–3 years)
- Trendelenburg gait — trunk lurches to affected side (weak abductors)
- Trendelenburg sign positive — pelvis drops on opposite side when standing on affected leg
- Short limb + waddling gait (bilateral DDH → classic "duck waddle")
- Lumbar lordosis (bilateral)
Older Child / Adult (Late presentation)
- Exercise-induced groin/hip pain
- Early osteoarthritis
- Limp
7. Investigations
Ultrasound (Gold standard <4–6 months)
- Hip not ossified at birth — ultrasound is the imaging of choice
- Measures α angle (acetabular bony roof) — normal ≥60°
- Measures β angle (cartilaginous roof)
- Dynamic assessment of hip stability
Plain X-ray (>4–6 months)
| Line | Description | Significance |
|---|---|---|
| Hilgenreiner's line | Horizontal line through both triradiate cartilages | Reference baseline |
| Perkin's line | Vertical line through lateral acetabular edge | Normal head = inferomedial quadrant |
| Shenton's line | Arc along femoral neck to obturator foramen | Broken in dislocation/subluxation |
| Acetabular index | Angle of acetabular roof to Hilgenreiner's line | Normal <30° at birth; <20° by age 2 |
MRI / CT
- Used pre/post-operatively
- MRI: best for cartilaginous structures, confirms reduction in spica cast
- CT: for osseous anatomy planning before osteotomy
8. Treatment
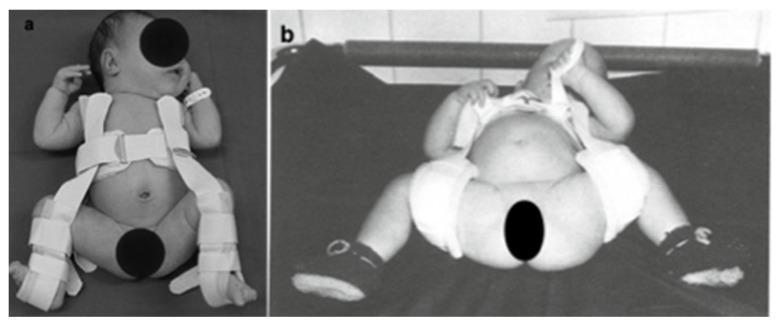
0–6 Months: Pavlik Harness
- First-line treatment
- Keeps hips flexed 100–110° and abducted (human position)
- Worn 23 hours/day; success rate ~85–95%
- Contraindicated in teratologic dislocation or older children
- Complication: avascular necrosis (AVN) of femoral head if over-abducted
6–18 Months: Closed Reduction + Hip Spica Cast
- Done under general anesthesia
- Arthrogram performed to confirm reduction
- Hip held in "safe zone" (human position)
- Spica cast for 3–6 months, changed under anesthesia
- Preceded by traction (2 weeks) to relax soft tissues and reduce AVN risk
18 Months – 4 Years: Open Reduction ± Osteotomy
- Open reduction via anterior (Smith-Petersen) approach
- Obstacles to reduction removed: hourglass capsule, inverted limbus, iliopsoas tendon, pulvinar
- Femoral osteotomy: derotation + shortening (reduces tension on femoral head)
- Pelvic osteotomy (Salter, Pemberton, or Dega): redirects acetabulum to cover femoral head
>4 Years: Salvage Procedures
- Shelf operations, Chiari osteotomy
- Total hip replacement in adulthood for failed cases
9. Complications
| Complication | Details |
|---|---|
| Avascular Necrosis (AVN) | Most serious; disrupts blood supply to femoral head; leads to deformity |
| Redislocation | After reduction; requires reoperation |
| Residual dysplasia | Incomplete acetabular remodeling |
| Limb length discrepancy | Especially in late/unilateral cases |
| Early osteoarthritis | Most common long-term sequela in missed/late-treated cases |
| Stiffness & gait abnormality | Post-operative or from prolonged casting |
10. Screening
- Neonatal clinical screening (Ortolani + Barlow) — all newborns
- Universal ultrasound at 4–6 weeks in countries like Germany/Austria
- Selective ultrasound in high-risk groups (breech, family history, clinical abnormality) — recommended in the UK and USA
- AAP/AAOS guidelines recommend risk-stratified screening
11. Key Differentials
| Condition | How to distinguish |
|---|---|
| Septic arthritis | Acute onset, fever, elevated CRP/WBC, toxic child |
| Perthes disease | Age 4–8, pain, Perthes on X-ray (fragmentation) |
| SCFE | Obese adolescent, "ice cream slipping off cone" on X-ray |
| Neuromuscular hip dislocation (CP) | Spasticity, neurological signs |
12. Key Exam Points for Class Discussion
- DDH is a spectrum, not just dislocation
- Female, firstborn, breech, family history = classic risk profile
- Ortolani = reduces; Barlow = dislocates (remember: O = Out → back in; B = Barlow boots it out)
- Ultrasound is gold standard in infants; X-ray after ossification
- Pavlik harness = <6 months; Open reduction + osteotomy = >18 months
- AVN of femoral head is the most dreaded complication
- Missed DDH → Trendelenburg gait → early OA
One more thing this is our paediatric surgery committee so give details accordingly
paediatric surgery congenital hip dislocation surgical techniques open reduction femoral pelvic osteotomy
DDH spica cast closed reduction arthrogram operative management children complications avascular necrosis
Pavlik harness hip spica cast DDH surgical treatment paediatric
CDH / DDH — Paediatric Surgery Committee Discussion
1. The Surgical Objective (Core Principle)
"The objective is to obtain a stable, congruous reduction of the femoral head within the acetabulum while avoiding damage to the capital epiphysis (Avascular Necrosis), which causes stiffness and proximal femoral deformity." — Bailey & Love's Surgery, 28th Ed., p. 638
- Under-treatment → persistent dislocation → early osteoarthritis
- Over-treatment / forceful reduction → AVN → femoral head destruction
2. Surgical Decision Framework by Age
Age at Diagnosis
│
├── 0–6 months ──────────────► Pavlik Harness (Non-operative)
│
├── 6–18 months ─────────────► Closed Reduction + Spica Cast
│ (± Preliminary Traction)
│
├── 18 months – 4 years ─────► Open Reduction ± Femoral Osteotomy
│ ± Pelvic Osteotomy
│
└── >4 years ────────────────► Open Reduction + Combined Osteotomies
(Salvage procedures in adults)
3. Non-Operative Management (Surgical Awareness Required)
Pavlik Harness (0–6 months)
| Parameter | Detail |
|---|---|
| Mechanism | Gravity + muscle activity spontaneously reduces and holds hip |
| Position | Hip flexion 100–110°, abduction 40–60° ("human position") |
| Duration | Full-time until stable, then part-time; total ~3–6 months |
| Success rate | ~85–95% for Graf IIc–IV in neonates |
| Failure criteria | No reduction within 3–4 weeks → discontinue (risk of Pavlik disease) |
- Age >6 months
- Teratologic dislocation (arthrogryposis, myelomeningocele)
- Failure of reduction after 3–4 weeks trial
4. Closed Reduction Under Anaesthesia (6–18 months)
Pre-operative: Skin or Skeletal Traction (1–3 weeks)
- Gradually stretches soft tissues (iliopsoas, adductors, capsule)
- Brings femoral head down to level of acetabulum
- Reduces the risk of AVN post-reduction
- Some centres have moved away from routine traction; still used selectively
The Procedure:
- General anaesthesia
- Arthrogram — contrast injected into hip joint; confirms position of femoral head, identifies obstacles (inverted labrum = "rose thorn" sign, hourglass capsule)
- Adductor tenotomy — if abduction <45°; performed percutaneously or open to widen safe zone
- Gentle reduction manoeuvre (Ortolani manoeuvre)
- Assess safe zone (Ramsey's zone) — arc between:
- Position where hip redislocates (lateral)
- Position where AVN risk begins (extreme abduction, medially)
- Safe zone must be ≥20–30° wide for closed reduction to be acceptable
- Apply hip spica cast in safe position (typically 45–60° abduction, 90–100° flexion, neutral rotation)
Post-operative:
- MRI or CT to confirm concentric reduction (X-ray unreliable in infants)
- Spica cast changed every 6–8 weeks under GA
- Total casting: 3–6 months
- Followed by Pavlik/abduction brace for further remodeling
5. Open Reduction (18 months and above)
- Closed reduction fails or safe zone inadequate
- Age >18 months (soft tissue obstacles unlikely to resolve)
- Late-presenting cases
- Teratologic dislocations
Obstacles to Reduction (Surgical Anatomy)
| Obstacle | Location | Surgical Action |
|---|---|---|
| Hourglass capsule constriction | Capsule itself | Capsulotomy + capsulorrhaphy |
| Inverted/hypertrophied labrum (limbus) | Acetabular rim | Excised or repositioned |
| Pulvinar | Fibrofatty tissue filling acetabulum | Excised |
| Ligamentum teres | Inside joint | Divided if excessively elongated |
| Iliopsoas tendon | Crosses capsular neck | Lengthened/released |
| Tight adductors | Medial thigh | Adductor tenotomy |
| Shallow acetabulum | Bony deficiency | Pelvic osteotomy |
| Coxa valga + anteversion | Proximal femur | Femoral osteotomy |
Surgical Approaches
A. Medial Approach (Ludloff) — 6 to 24 months
- Between adductor longus and pectineus (or gracilis)
- Excellent access to medial obstacles (pulvinar, ligamentum teres, capsule)
- Cannot perform capsulorrhaphy
- Cannot perform pelvic osteotomy simultaneously
- Used for straightforward open reductions in younger infants
B. Anterior (Anterolateral / Smith-Petersen) Approach — >9–12 months
- Between tensor fascia lata (sup. gluteal nerve) and sartorius/rectus femoris (femoral nerve)
- Preferred for older children
- Allows:
- Complete visualization and removal of all obstacles
- Capsulorrhaphy (tightening of redundant capsule — critical for stability)
- Simultaneous pelvic osteotomy
- Internervous plane: TFL (sup. gluteal n.) / Sartorius (femoral n.)
6. Femoral Osteotomy
Indications:
- Excessive anteversion (>40°) causing instability
- Coxa valga (neck-shaft angle >150°)
- Needed to shorten femur (in late cases — reduces pressure on femoral head, lowers AVN risk)
Types:
| Osteotomy | What it corrects | Notes |
|---|---|---|
| Derotation osteotomy | Excessive anteversion | Most common; brings femoral head forward into acetabulum |
| Varus osteotomy | Coxa valga | Reduces neck-shaft angle to ~120–130° |
| Shortening osteotomy | Limb length + reduces tension | Essential in children >2–3 years; prevents AVN from forceful reduction |
- Performed at the subtrochanteric or intertrochanteric level
- Fixed with a blade plate, DCP, or pediatric hip screw
- Often combined with pelvic osteotomy (triple procedure)
7. Pelvic Osteotomies
Salter Innominate Osteotomy (most commonly discussed)
- Age: 18 months – 6 years (open triradiate cartilage required)
- Mechanism: Single cut through ilium above acetabulum; acetabulum rotated anterolaterally as a unit; bone graft (from iliac crest) holds correction
- Corrects: Anterior and lateral deficiency of coverage
- Limitation: Cannot increase overall acetabular volume
Pemberton Osteotomy
- Incomplete (hinge) osteotomy through ilium curving to triradiate cartilage
- Bends acetabular roof downward — reduces acetabular volume (good for large femoral head coverage)
- Requires open triradiate cartilage as a hinge
Dega Osteotomy
- Similar to Pemberton but hinge is more posterior
- Popular in neuromuscular hip dysplasia (cerebral palsy)
- Good posterior coverage
Triple Pelvic Osteotomy (Steel/Tönnis) — older children with closed triradiate
- Cuts through ilium, ischium, and pubis
- Full mobilization of acetabular fragment
- Used when triradiate cartilage closed (>8 years)
Chiari Osteotomy — salvage
- Medial displacement of ilium above hip joint
- Does not redirect acetabulum; creates a shelf of ilium for coverage
- Used when redirectional osteotomies not possible (older, deformed acetabulum)
Comparison Summary:
| Osteotomy | Age | Triradiate | Mechanism | Best for |
|---|---|---|---|---|
| Salter | 18m–6y | Open | Rotates acetabulum anterolaterally | Anterior + lateral deficiency |
| Pemberton | 18m–8y | Open (hinge) | Tilts roof down, reduces volume | Large femoral heads |
| Dega | 18m–8y | Open | Posterior tilt | Neuromuscular dysplasia |
| Triple (Steel) | >8y | Closed | Full acetabular mobilization | Older child/adolescent |
| Chiari | Any | Any | Medialization shelf | Salvage |
8. The Combined / Triple Procedure
Open Reduction (anterior approach)
+
Femoral Osteotomy (derotation + varus + shortening)
+
Pelvic Osteotomy (Salter or Pemberton)
- Minimise number of GA exposures in children
- Allow simultaneous correction of all deformities
- Improve overall surgical outcome
9. Post-operative Protocol (Surgical)
| Phase | Management |
|---|---|
| Immediate post-op | Hip spica cast (4–6 weeks), neurovascular monitoring |
| Cast removal | Under GA; check X-ray/MRI for reduction quality |
| Rehabilitation | Physiotherapy — hip ROM, muscle strengthening |
| Hardware removal | Plates/screws removed after osteotomy healed (6–12 months) |
| Follow-up | Until skeletal maturity (to monitor for AVN, residual dysplasia, remodeling) |
10. Complications — Surgical Perspective
Avascular Necrosis (AVN) of Femoral Head — Most Critical
- Caused by: forceful reduction, extreme abduction, surgical insult to blood supply
- Blood supply to femoral head: medial circumflex femoral artery (main) → retinacular vessels
- Kalamchi & MacEwen Classification:
| Grade | Description | Outcome |
|---|---|---|
| I | Lateral epiphyseal damage only | Mild; usually remodels |
| II | Central epiphyseal arrest | Shortened femoral neck |
| III | Lateral physeal arrest | Coxa breva + greater trochanter overgrowth |
| IV | Total epiphyseal ischaemia | Severe deformity, poor prognosis |
Other Surgical Complications:
| Complication | Cause | Management |
|---|---|---|
| Redislocation | Poor capsulorrhaphy, inadequate soft tissue release | Reoperation |
| Residual dysplasia | Insufficient acetabular remodeling | Secondary osteotomy |
| Femoral nerve injury | Anterior approach retraction | Careful dissection, usually transient |
| Infection | Deep surgical site | Antibiotics ± washout |
| Implant failure | Hardware loosening in osteotomy | Revision fixation |
| Stiffness | Prolonged immobilization | Physiotherapy |
| Leg length discrepancy | Physeal damage from AVN | Epiphysiodesis / limb lengthening |
| Early osteoarthritis | Residual dysplasia / AVN | THR in adulthood |
11. Surgical Outcomes — Prognostic Factors
| Better Outcome | Worse Outcome |
|---|---|
| Early diagnosis (<6 months) | Late diagnosis (>2 years) |
| Unilateral | Bilateral |
| Concentric reduction achieved | Redislocation / AVN |
| Normal acetabular index by age 2 | Persistent steep acetabulum |
| No AVN | AVN Grade III–IV |
| Adequate soft tissue release | Residual instability |
Key prognostic milestone: If the acetabular index normalises to <25° by age 2, the outcome is likely excellent with no further intervention required.
12. Key Surgical Discussion Points for the Committee
-
Why do we prefer anterior over medial approach in children >12 months? → Allows capsulorrhaphy + simultaneous pelvic osteotomy in one sitting
-
What is the "safe zone" and why does it matter intraoperatively? → Determines feasibility of closed reduction; narrow safe zone = proceed to open
-
Why is femoral shortening osteotomy critical in late-presenting cases? → Reduces lever arm tension on femoral head → prevents AVN
-
What is Pavlik disease and how do we avoid it? → Abandon harness if no reduction in 3–4 weeks; posterior acetabular erosion
-
When do you choose Pemberton over Salter? → Pemberton when femoral head is large relative to acetabulum and you need to reduce volume, not just redirect
-
What is the single most feared complication and why? → AVN — irreversible, leads to femoral head collapse and lifetime disability
Can you give me like detentions pathologies treatment singhs symptoms like that for children with respect to this topic easy to read for class discussion
congenital hip dislocation DDH pathological anatomy acetabulum femoral head changes children
DDH signs symptoms clinical examination Ortolani Barlow Trendelenburg galeazzi children age groups
DDH clinical signs Ortolani Barlow Trendelenburg gait examination child
🦴 CDH / DDH — Quick Class Reference
Congenital Dislocation of the Hip | Paediatric Surgery
📌 DEFINITION
DDH is a spectrum of hip instability — from a mildly shallow socket to a completely dislocated hip that cannot be put back in place.
- Dysplasia → shallow socket, head still inside
- Subluxation → head partially out
- Dislocation → head completely out
- Dislocatable → head in, but can be pushed out
📌 REMEMBER: WHO GETS IT?
| Risk Factor | Why |
|---|---|
| Female | Maternal hormones (relaxin) cause more ligament laxity in girls |
| Firstborn | Tight, unstretched uterus |
| Breech position | Hip forced into extended/adducted position |
| Family history | Genetic predisposition |
| Left hip | Most common fetal position presses left hip against sacrum |
| Tight swaddling | Extended legs force hip out of socket |
📌 PATHOLOGY — WHAT CHANGES INSIDE?
🔴 The Socket (Acetabulum)
- Becomes shallow and steep (can't hold the head)
- Fills with fatty tissue (pulvinar) — blocks reduction
- Labrum (limbus) gets inverted — another block to reduction
🟡 The Femoral Head
- Small and underdeveloped
- Femoral neck too angulated (coxa valga)
- Too much twist (anteversion) — head points wrong way
🟢 Soft Tissues
- Capsule stretches and becomes hourglass-shaped — strangles joint
- Iliopsoas tendon tightens across the front — blocks reduction
- Adductor muscles tighten — limit abduction
- Ligamentum teres becomes elongated and loose
📌 SIGNS & SYMPTOMS — BY AGE
👶 Newborn (0–3 months)
| Sign | How to Test | What it Means |
|---|---|---|
| Ortolani Sign | Flex hip 90°, abduct → feel a clunk | Dislocated hip going back in ✅ |
| Barlow Sign | Flex hip, adduct + push back → feel a clunk | Stable hip being pushed out ✅ |
| Asymmetric skin folds | Look at thigh/buttock creases | Extra folds on dislocated side |
⚠️ Both tests lose value after 3 months — soft tissues tighten and the clunk disappears
🧒 Infant (3–18 months)
| Sign | How to Detect |
|---|---|
| Limited hip abduction | Can't spread legs >60° on affected side — most reliable sign |
| Galeazzi Sign (Allis Sign) | Lay baby flat, flex both hips & knees → knee on affected side is lower |
| Leg length discrepancy | Affected leg looks shorter |
| Asymmetric skin folds | Unreliable alone but supportive |
🚶 Toddler / Walking Child (>1 year)
| Sign/Symptom | Description |
|---|---|
| Trendelenburg Gait | Trunk lurches toward the affected side when walking |
| Trendelenburg Sign | When standing on affected leg — pelvis drops on the other side (weak abductors) |
| Waddling gait | Both sides affected → classic duck walk |
| Limb shortening | One leg visibly shorter |
| Lumbar lordosis | Exaggerated lower back curve (especially bilateral) |
| No pain | Children rarely complain of pain at this age |
🧑 Older Child / Adolescent
| Symptom | Notes |
|---|---|
| Groin or hip pain with exercise | First complaint in missed cases |
| Limp | From leg length discrepancy or muscle weakness |
| Reduced activity tolerance | Gets tired walking |
| Early arthritis signs | Late complication of untreated DDH |
📌 INVESTIGATIONS
| Age | Best Test | Why |
|---|---|---|
| 0–4 months | Ultrasound (USG) | Femoral head not yet ossified — X-ray useless |
| >4–6 months | X-ray (AP Pelvis) | Ossification begins; lines can be drawn |
| Pre/post-op | MRI | Confirms reduction in spica cast; soft tissue detail |
| Surgical planning | CT scan | Bony anatomy for osteotomy planning |
Ultrasound — Graf Classification
| Type | Alpha Angle | Meaning |
|---|---|---|
| I | ≥60° | Normal |
| II | 43–59° | Immature / mild dysplasia |
| III | <43° | Subluxated |
| IV | — | Dislocated |
X-ray — Key Lines to Know
| Line | How to Draw | Normal Finding |
|---|---|---|
| Hilgenreiner's line | Horizontal through both triradiate cartilages | Baseline reference |
| Perkin's line | Vertical from lateral edge of acetabulum | Femoral head = inner lower quadrant |
| Shenton's line | Arc: femoral neck → obturator foramen | Smooth arc = normal; broken = dislocated |
| Acetabular Index | Angle of acetabular roof to Hilgenreiner's | Normal: <30° at birth, <20° by age 2 |
📌 TREATMENT — AGE BY AGE
🟢 0–6 Months → Pavlik Harness
- Soft harness, keeps hips flexed + slightly apart
- Worn 23 hours/day
- Success ~85–95%
- Stop if no reduction in 3–4 weeks → risk of Pavlik disease
🟡 6–18 Months → Closed Reduction + Spica Cast
- Done under general anaesthesia
- Arthrogram (contrast dye) confirms femoral head position
- Adductor tenotomy done if hip won't open enough
- Hip held in safe position in hip spica cast
- Cast changed every 6–8 weeks under GA
🔴 18 Months – 4 Years → Open Reduction ± Osteotomies
- Surgical approach: Anterior (Smith-Petersen)
- Remove all obstacles inside joint (pulvinar, inverted labrum, tight capsule, iliopsoas)
- Tighten loose capsule (capsulorrhaphy)
- Add femoral osteotomy if neck angle or twist is wrong
- Add pelvic osteotomy if socket is still too shallow
🔵 >4 Years → Combined Surgery
- Open reduction + femoral osteotomy + pelvic osteotomy = Triple Procedure in one sitting
- Longer recovery, higher complication risk
- Salvage osteotomies (Chiari) if socket too deformed to redirect
📌 PELVIC OSTEOTOMIES — QUICK COMPARISON
| Name | Age | Key Point |
|---|---|---|
| Salter | 18m–6y | Rotates whole socket forward — most common |
| Pemberton | 18m–8y | Bends roof down — good for large femoral heads |
| Dega | 18m–8y | Posterior tilt — good in cerebral palsy cases |
| Triple (Steel) | >8y | Cuts 3 bones — for older kids with closed growth plate |
| Chiari | Any age | Salvage shelf — last resort |
📌 COMPLICATIONS
| Complication | Key Point |
|---|---|
| ⚠️ AVN (Avascular Necrosis) | Most feared — blood supply to femoral head cut off → head collapses → lifetime disability |
| Redislocation | Reduction doesn't hold → redo surgery |
| Residual dysplasia | Socket never fully develops → secondary osteotomy |
| Leg length discrepancy | From AVN or physeal damage |
| Stiffness | From prolonged casting or surgery |
| Nerve injury | Femoral nerve at risk in anterior approach |
| Early osteoarthritis | End result of all missed/failed cases |
📌 AVN — WHY IT HAPPENS & HOW TO AVOID IT
| Cause | Prevention |
|---|---|
| Forceful reduction | Gentle technique; traction beforehand |
| Extreme abduction in cast | Keep abduction in safe zone (45–60°) |
| Surgical damage to vessels | Careful dissection around femoral neck |
| Pavlik harness over-abduction | Avoid Lorenz (extreme) position |
📌 GOLDEN RULES FOR CLASS
- Earlier = Better — every month of delay = harder surgery + worse outcome
- Ortolani reduces, Barlow dislocates
- USG for babies; X-ray for older children
- Pavlik → Closed reduction → Open reduction → Osteotomies (age ladder)
- AVN is the enemy — every surgical decision aims to reduce this risk
- If acetabular index is <25° by age 2 → excellent prognosis